

Abstract
Background:
Dentinogenesis imperfecta is a genetic disorder of the dentin occurring during the tooth development. It leads to many structural changes that can be identified clinically (brownish colored teeth, cracked enamel) and radiologically (globular crown, cervical constriction, short roots, and obliterated pulp chamber and/or root canals). The aim of this study was to determine by panoramic radiographs assessment the incidence of dentinogenesis imperfecta in a group of patients attending a specialized maxillofacial imaging center in Paris, France.
Material and Methods:
A retrospective observational study was conducted using panoramic radiographs of 8830 patients (3723 males and 5107 females), which were used to search the radiological criteria of dentinogenesis imperfecta.
Results:
In our sample, the prevalence of dentinogenesis imperfecta was 0.057%. Out of the 8830 subjects, 0.080% of the males presented the radiological signs of the dentinogenesis imperfecta against 0.039% of the females.
Conclusion:
In our study, we found that dentinogenesis imperfecta is a relatively rare dental anomaly in France, with a rate different from the rates reported in other studies and with no disparity in prevalence among genders.
Keywords: Dentinogenesis imperfecta, French, panoramic radiography
Introduction
Tooth structure anomalies may affect the enamel, the dentin, and the cementum. Dentinogenesis imperfecta (DI) is a genetic disorder of the dentin occurring during the tooth development. It was first described in the 19th century and may affect the temporary and the permanent dentitions.[1] Literature reports only few studies on the epidemiology of DI (Witkop et al.,[2] Gupta et al.[3]). Furthermore, no such previous study was conducted on a French population.
Genetically, DI is inherited in a simple autosomal dominant mode.[4]
Shields et al.[5] classified DI into three types:
Type 1: DI associated with osteogenesis imperfecta.
Type 2: DI identical clinically, radiologically, and histologically to type 1 but without being associated to osteogenesis imperfecta.
Type 3: A rare DI involving, unlike types 1 and 2, teeth with shell-like appearance and multiple pulp exposures.
Many authors suggested that both type 2 and type 3 of DI are different expressions of the same gene.[6,7,8]
Clinically, the teeth color changes from brown to blue, occasionally described as amber or gray, with an opalescent sheen. Hypoplastic or hypocalcified defects may attack the enamel in about one-third of the patients causing it to crack away from the affected dentin. The latter becoming exposed may undergo severe and rapid attrition.[4,9,10]
Radiologically, the signs are pathognomonic of the affection. The crown is globular with marked cervical constriction, the roots are short, and the pulp chamber and/or the root canals are partially or totally obliterated [Figure 1].[9,11]
Figure 1.
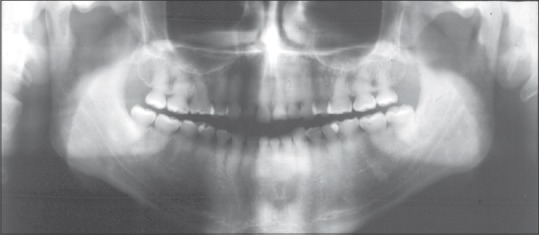
Panoramic radiograph showing the globular crowns with cervical constrictions and the partial/total obliteration of the pulp cavities and/or the root canals
The aim of this study was to determine, radiologically, the incidence of DI in France in patients attending a specialized maxillofacial imaging center located in Paris.
Materials and Methods
In a retrospective statistical study including almost all the dental development anomalies, more precisely the dental agenesis, hypergenesis, dysmorphia, structural anomalies and transpositions, the archived panoramic radiographs of 8830 patients were assessed.
These patients were referred by their dentists to a specialized maxillofacial imaging center for multiple indications (e.g., impacted teeth, pre-prosthetic dental examinations, sinus diagnosis, etc.).
By the policy of the center, all patients were informed that the radiographs might be anonymously used for research purposes at a later stage and their consent was obtained. The study got the approval of the Center Institutional Board.
The exclusion criteria included all the radiographs presenting pathological changes or deformities in the mandible and/or maxilla. Random selection of radiographs in a reverse chronological order was followed until the desired number was reached.
The sample examined was formed of 3723 (42.16%) males and 5107 (57.83%) females.
The minimum needed sample size was calculated according to the following formula:
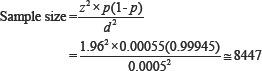
where:
z= z-score (1.96 for a confidence level of 95%)
p= expected proportion (estimated 0.055% as it belongs to the range of prevalence rates in previous studies (prevalence ranged between 0.01 and 0.09)
d= marginal error (we chose it to be 0.05% in our study)
Therefore, our sample comprising 8830 subjects can be considered statistically representative.
The radiographs were assessed by two oral diagnosis specialists having more than 15 years of experience. Detailed discussion and standardization of diagnostic criteria between both examiners preceded image evaluation. Concerning evaluation period, it extended for one year (30 sessions of an average of 300 cases each with a period of one week existing between the sessions).
In this paper, we only discuss the presence of the DI among all the radiographically searched dental anomalies.
In order to make the radiologic diagnosis of the DI. three elements were searched:
The short dental roots
The globular crowns with cervical constrictions
The partial/total obliteration of the pulp cavities and/or the root canals.
For data entry and analysis, The Statistical Package for Social Sciences for Windows version 24 (IBM Corp., Armonk, New York) was used. Chi-square test and Fischer's exact test were used to test statistical significance; t-tests were used for hypotheses testing.
Results
In our study, we examined the panoramic radiographs of 8830 patients [3723 (42.16%) males and 5107 (57.83%) females]. We found 5 patients with radiological signs of DI including 2 members (brother and sister) of the same family. Two of these patients had complete obliteration of the pulp chambers and root canals. The other 3 patients (including brother and sister) had a partial obliteration at each tooth or at the level of the entire dentition. The prevalence rate in our sample can be calculated as:
Prevalence of DI = (number of cases/sample size) × 100 = 0.057%
Dentinogenesis imperfecta is slightly more frequent in our population, in the male sex [3/5 (60%) against 2/5 (40% in females)]. It was not associated with any other teeth developmental anomaly.
Discussion
Although several researchers have determined the prevalence of several dental anomalies, few have statistically analyzed DI prevalence and distribution; moreover, no such previous study was done in the French population. Since prevalence rate is very low, we can consider it approximately equal to the relative risk of DI.
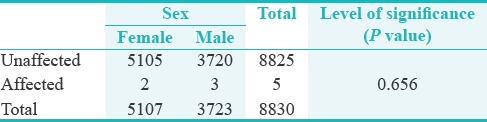
The gender difference seems to be statistically insignificant (P > 0.05) [Table 1]. This suggests that DI is independent of sex. However, we cannot confirm independence due to the possibility of type II error. Therefore, a larger sample size, which decreases the risk of committing a type II error, would give more insight on this parameter.
Table 1.
Gender distribution of individuals affected with DI along with P value from two-sided Fischer's exact Test showing no significance in difference (P>0.05)
According to de La Dure-Molla,[12] the only epidemiological data concerning DI was published in 1975. Witkop stated that DI estimated incidence was between 1/6000 and 1/8000.[2] These data only came from the United States. In other countries, case reports concerned smaller cohorts.[9,13,14,15] A study on Indian population had a prevalence rate of DI of 0.09%; their results consisted of only one affected individual who was a male.[3] Therefore, gender difference could not be evaluated.[10]
Some data retrieved from the literature regarding the prevalence of DI are summarized in Table 2.
Table 2.
Prevalence rates of DI in the literature

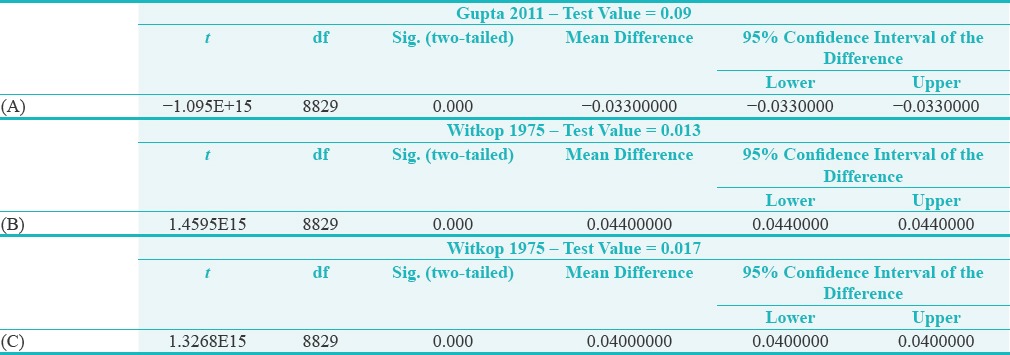
Our study shows that the prevalence rate of DI in France is not in accordance with that in the aforementioned US and Indian populations. In all of the t-tests done to compare our prevalence rate with that of previous studies, null hypotheses were rejected and hence difference between rates was established (P < 0.05) [Table 3].
Table 3.
t-tests to compare our study's prevalence rate with Gupta 2011 (A) and Witkop 1975 (B and C) prevalence rates of DI; the significant difference in the three tests (P<0.05)
Aside from being the first study to evaluate DI prevalence rate in France, another strong point in our research is its statistically reliable sample size. Previous studies that assessed DI had questionable sample sizes. Our sample is statistically representative with an extremely low margin of error (0.05%). This allows us to claim that our results represent, by far, the most reliable numbers in literature on the prevalence of DI currently and can be considered a new and reliable reference for the prevalence rate for future epidemiological studies.
Despite that our study comprised a representative and reliable sample, one of its limitations is that a larger sample size would provide more definitive information on the prevalence of DI and, in particular, its gender predisposition; this was evident when we failed to prove or refute the gender difference. In addition, the absence of wide epidemiological studies in the literature and the variation of small studies results make it difficult to compare and analyze the obtained results with reference values.
Conclusion
Dentinogenesis imperfecta is a hereditary developmental disorder of dentin that leads to structural changes of the affected teeth. It represents a very rare dental anomaly whose rate, in France, is different than that reported in other countries. DI incidence is gender neutral; there is no higher prevalence in one sex over another. The variation in the prevalence of our study in comparison with previous ones may be caused by consanguineous marriages in populations with higher prevalence rate, difference in diagnostic criteria of DI or due to racial differences. Despite being a relatively large study in a population that has not been assessed for DI before, larger epidemiological studies distributed in different populations would provide more insight on the distribution and predisposition of DI.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The authors would like to thank Dr. Ibrahim Nasseh for his technical help during the write up of the study.
References
- 1.Talbot ES. Arrests of development and decalcification of enamel and dentin. JADA. 1983;20:30. [Google Scholar]
- 2.Witkop CJ., Jr Hereditary defects of dentin. Dent Clin North Am. 1975;19:25–45. [PubMed] [Google Scholar]
- 3.Gupta SK, Saxena P, Jain S, Jain D. Prevalence and distribution of selected developmental dental anomalies in an Indian population. J Oral Sci. 2011;53:231–8. doi: 10.2334/josnusd.53.231. [DOI] [PubMed] [Google Scholar]
- 4.Witkop CJ, Rao S. Inherited Defects in Tooth Structure. Baltimore: Williams and Wilkins; 1971. p. 153. [PubMed] [Google Scholar]
- 5.Shields ED, Bixler D, El-Kafrawy AM. A Proposed classification for heritable human dentin defects with a description of a new entity. Arch Oral Biol. 1973;18:543–53. doi: 10.1016/0003-9969(73)90075-7. [DOI] [PubMed] [Google Scholar]
- 6.Boughman JA, Halloran SL, Roulston D, Schwartz S, Suzuki JB, Weitkamp LR, et al. An autosomal-dominant form of juvenile periodontitis: Its localization to chromosome 4 and linkage to dentinogenesis imperfecta and Gc. J Craniofac Genet Dev Biol. 1986;6:341–50. [PubMed] [Google Scholar]
- 7.Witkop CJ., Jr Amelogenesis imperfecta, dentinogenesis imperfecta and dentin dysplasia revisited: Problems in classification. J Oral Pathol. 1988;17:547–53. doi: 10.1111/j.1600-0714.1988.tb01332.x. [DOI] [PubMed] [Google Scholar]
- 8.Devaraju D, Devi BY, Vasudevan V, Manjunath V. Dentinogenesis imperfecta type I: A case report with literature review on nomenclature system. J Oral Maxillofac Pathol. 2014;18:S131. doi: 10.4103/0973-029X.141363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pintor A, Alexandria A, Marques A, Abrahao A, Guedes F, Primo L. Histological and Ultrastructure Analysis of Dentin Dysplasia Type I in Primary Teeth: A Case Report. Ultrastruct Pathol. 2015;39:281–5. doi: 10.3109/01913123.2014.1002960. [DOI] [PubMed] [Google Scholar]
- 10.Akhlaghi N, Eshghi AR, Mohamadpour M. Dental Management of a Child with Dentinogenesis Imperfecta: A Case Report. J Dent. 2016;13:133. [PMC free article] [PubMed] [Google Scholar]
- 11.Barron MJ, McDonnell ST, MacKie I, Dixon MJ. Hereditary dentine disorders: Dentinogenesis imperfecta and dentine dysplasia. Orphanet J Rare Dis. 2008;3:31. doi: 10.1186/1750-1172-3-31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.de La Dure-Molla M, Philippe Fournier B, Berdal A. Isolated dentinogenesis imperfecta and dentin dysplasia: Revision of the classification. Eur J Hum Genet. 2015;23:445–51. doi: 10.1038/ejhg.2014.159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Poorolajal J, Khajeh S, Faramarzi F, Kahnamoui HM. Prevalence of dental anomalies among 7-to 35-year-old people in Hamadan, Iran in 2012-2013 as observed using panoramic radiographs. Imaging Sci Dent. 2014;44:7–13. doi: 10.5624/isd.2014.44.1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Yassin SM. Prevalence and distribution of selected dental anomalies among Saudi children in Abha, Saudi Arabia. J Clin Exp Dent. 2016;8:e485. doi: 10.4317/jced.52870. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Seow WK. Developmental defects of enamel and dentine: Challenges for basic science research and clinical management. Aust Dent J. 2014;59:143–54. doi: 10.1111/adj.12104. [DOI] [PubMed] [Google Scholar]