

Abstract
Stress fractures are a frequent cause of lower extremity pain in athletes, and especially in runners. Plain imaging has a low sensitivity. Magnetic resonance imaging (MRI) or bone scan scintigraphy is the criterion standard, but expensive. We present the case of a young female distance runner with left shin pain. Plain radiography was unremarkable. Ultrasound showed focal hyperechoic elevation of the periosteum with irregularity over the distal tibia and increased flow on Doppler. These findings were consistent with a distal tibia stress fracture and confirmed by MRI. Examination of our case will highlight the utility of considering an ultrasound for diagnosis of tibial stress fracture.
Keywords: Stress fracture, tibia, ultrasound
Introduction
Stress injuries are the most common cause of lower extremity pain in athletes.1 Bone stress injuries account for approximately 8.2% of all injuries in elite track and field athletes.2 Bone stress injuries may mature into stress fractures.3 Stress fractures are a result of accelerated physiologic change from excessive loading applied to a normal bone.4,5 This is the sequelae of high intensity, duration of training, nutrition, and biomechanical, muscular, and hormonal imbalance.2,3 Typically, the metatarsal bones in the lower extremity are involved. However, the tibia is the most commonly implicated in runners.6 Differential diagnosis includes fracture of the tibia, muscle sprain or contusion, periostitis, bur-sitis, medial tibial stress syndrome, and compartment syndrome.2
The diagnosis of tibia stress fractures requires high level of clinical suspicion, and confirmation is needed with imaging. Plain radiographs have often times yielded negative results until 3 weeks to 3 months when bone callus is formed.6,7 The criterion standard for diagnosis of stress fractures is magnetic resonance imaging (MRI) or bone scan scintigraphy.8,9 The high cost of these 2 imaging modalities has paved way for research into other less diagnostic tests such as ultrasonography.10 Ultrasonography has been shown to be beneficial in the diagnosis of lower extremity stress fractures, primarily in metatarsal bones and ankle malleoli.5,11,12 The diagnosis of tibia stress fractures with ultrasound has only been reported in a few cases.13,14 The purpose of this case report is to contribute to the limited evidence in literature regarding the diagnosis of tibia stress fractures with ultrasonography.
Case Presentation
The patient was an otherwise healthy 19-year-old white female division 1 collegiate mid-distance runner who came to the office complaining of left shin pain. She had been an athlete throughout high school and recollected having pain in the same area for several months. However, 3 weeks prior to coming to the office, she had increased her intensity in training and noted increased pain. She described the pain as a sharp pain and initially rated it as a 3/10 in intensity (measured by visual analog scale of 1-10, where 10 is worst pain). The pain, however, had progressed to a 9/10 in intensity prior to being seen in clinic. The pain was constant and radiated to the calf region. It was worsened by walking and running. The pain was alleviated temporarily by ibuprofen and ice. She denied any swelling, numbness, or tingling in the foot. She had no medical or surgical history and was not currently taking any medications. Family history was negative for musculoskeletal disease.
Patient’s examination revealed tenderness on the left mid-shaft of the tibia along the anterior border. Neurological examination was within normal limits. After a trial of conservative management with rest, ice, and nonsteroidal anti-inflammatory drugs, plain radiography of the left lower extremity was performed and was unremarkable (Figure 1). Ultrasound of the left tibia showed focal hyperechoic elevation of periosteum with irregularity over the left distal tibia measuring about 3 cm with a positive Doppler over the area (Figures 2 and 3). An MRI was ordered that confirmed periosteal reaction consistent with stress fracture over the distal tibia with no fracture line (Figure 4).
Figure 1.

Normal x-ray findings of the left lower extremity in the posterior anterior view.
Figure 2.
Ultrasound image with transverse view of tibia showing increased periosteal inflammation. Increased periosteal Doppler flow is also seen (hyperemia/hypervascularity).
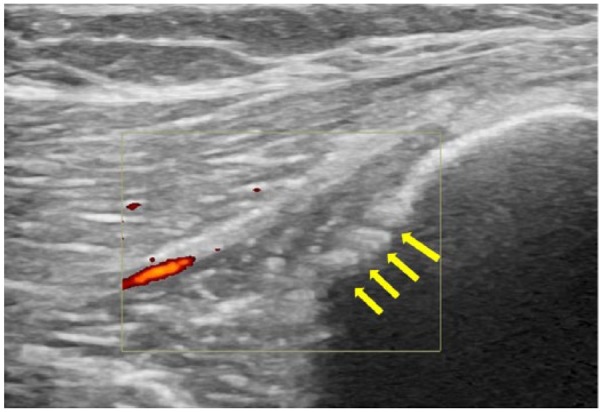
Figure 3.

Longitudinal view of the anterior tibia showing discontinuity of hyperechoic line representing disruption of bony cortex (green arrow) and periosteal edema (yellow arrows). On the left-hand side is a diagram showing the orientation of the probe.
Figure 4.
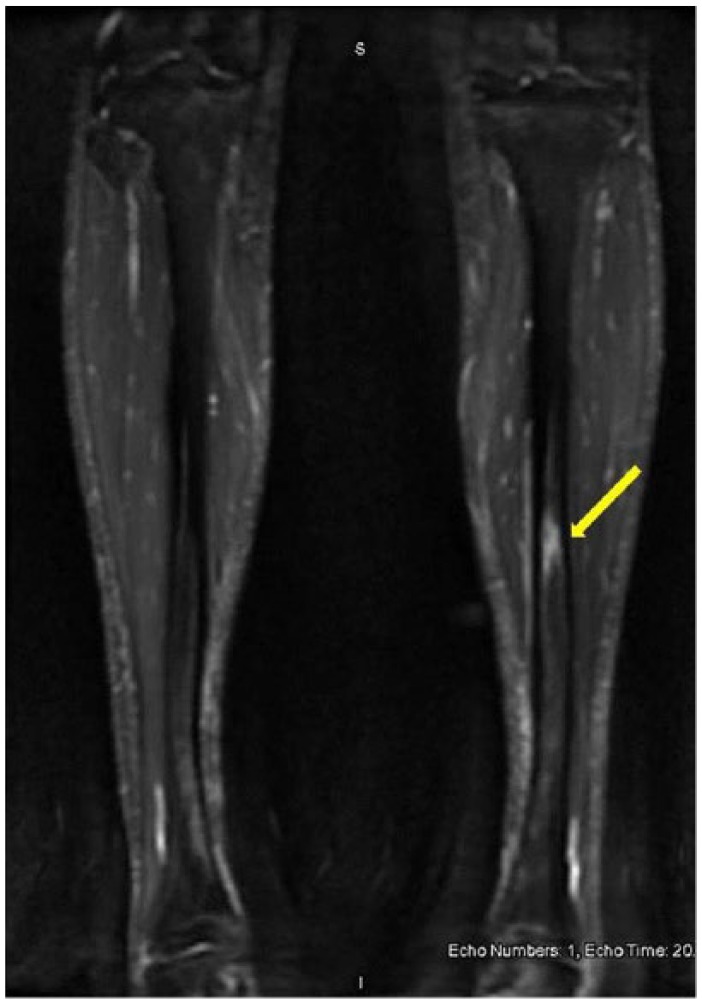
T2 coronal (left) image shows a lucent appearance at site of pain, and axial (right) image reveals marrow edema (green arrow) and periosteal edema (yellow arrows) of the tibia.
Patient was advised to stop running and use ibuprofen as needed. She was also given a Velcro walking boot to wear that provided leg support. On 3 weeks of follow-up, the patient was doing well without any significant symptoms (Figure 5).
Figure 5.
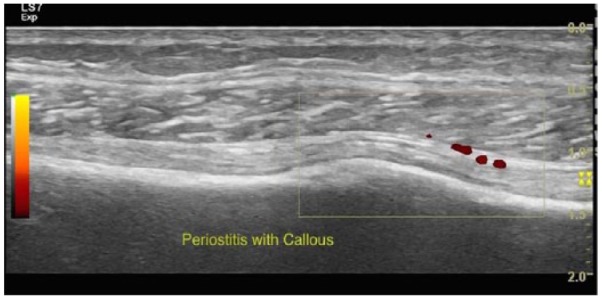
Follow-up longitudinal view at 3 weeks shows callous formation at site of injury which signifies healing.
Discussion
Stress fractures are especially prominent in individuals who suddenly increase physical activity. It is important to diagnose stress fractures early to prevent bone remodeling, nonunion injuries, and loss of function.2,6 The sensitivity of standard radiography which can miss fractures in the early stages of stress fractures due to the absence of callus formation can be as low as 10%.15 Bone scan with technetium Tc 99m diphosphonate allows for early diagnosis but is coupled with high costs, lengthy procedure times, and exposure to ionizing radiation.4 Magnetic resonance imaging provides a noninvasive method of detecting stress fractures with good sensitivity, but its high cost and poor accessibility in some rural areas prevent routine use.8 Both are highly sensitive and provide optimal depiction of bone marrow edema, periosteal inflammation, and cortical fractures.16
Although these modalities have become the standard for diagnosis, ultrasonography is becoming more accepted as a first-line imaging modality for soft tissues, muscles, and tendon pathologies.17,18 Cortical irregularities and hypertrophic changes may be visualized before they are seen on plain radiographs or MRI.18 In stress fractures, ultrasound offers dynamic images in a noninvasive, fast, and inexpensive manner.19 Its sensitivity and specificity compared with MRI remain inferior despite its 81.8% sensitivity and 66.6% specificity of ultrasound in the diagnosis of metatarsal stress fractures.2 Hallmark findings are present in the diagnosis of stress fractures using ultrasound and were likewise found in this case report. These findings include the following:
Hyperechogenicity of the surrounding soft tissue which indicates soft tissue edema and inflammatory reaction12,20;
Thickening of the periosteum10;
Increased periosteal color Doppler flow.22
Widespread use of the ultrasound in stress fractures varies by circumstance and is still an area of ongoing research. Its major drawback is that it is heavily operator dependent, requiring skill to recognize normal anatomy and pathology. Given its small field of view, nearby anatomical structures are often unavailable. However, the current imaging modalities are cost intensive, poorly accessible, and invasive and are linked with increased patient discomfort. Continued improvements in ultrasound resolution quality have increased its clinical utility. In the hands of a skilled technician, ultrasound can provide real-time unparalleled images to detect stress fractures in a safe and portable manner. This case emphasizes that in cases where there is suspicion of stress fracture, diagnostic ultrasound can provide a good alternative.
Footnotes
Peer review:Six peer reviewers contributed to the peer review report. Reviewers’ reports totaled 649 words, excluding any confidential comments to the academic editor.
Funding:The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions: Case conception and design: AAm, RM, AS. Acquisition of data: AAm, RM, AS. Analysis and interpretation of data: AAm, AAb, RM, AS. Drafting of manuscript: AAm, AAb, RM, AS. Critical revision: AAm, AAb, RM, AS.
References
- 1. Dobrindt O, Hoffmeyer B, Ruf J, et al. Blinded-read of bone scintigraphy: the impact on diagnosis and healing time for stress injuries with emphasis on the foot. Clin Nucl Med. 2011;36:186–191. [DOI] [PubMed] [Google Scholar]
- 2. Papalada A, Malliaropoulos N, Tsitas K, et al. Ultrasound as a primary evaluation tool of bone stress injuries in elite track and field athletes. Am J Sports Med. 2012;40:915–919. [DOI] [PubMed] [Google Scholar]
- 3. Reeder MT, Dick BH, Atkins JK, Pribis AB, Martinez JM. Stress fractures: current concepts of diagnosis and treatment. Sports Med. 1996;22:198–212. [DOI] [PubMed] [Google Scholar]
- 4. Geslien GE, Thrall JH, Espinosa JL, et al. Early detection of stress fractures using 99mTC-polyphosphonate. Radiol. 1976;121:683–687. [DOI] [PubMed] [Google Scholar]
- 5. Bianchi S, Luong DH. Stress fractures of the ankle malleoli diagnosed by ultrasound: a report of 6 cases. Skeletal Radiol. 2014;43:813–818. [DOI] [PubMed] [Google Scholar]
- 6. Romani WA, Perrin DH, Dussault RG, Ball DW, Kahler DM. Identification of tibial stress fractures using therapeutic continuous ultrasound. J Orthop Sports Phys Ther. 2000;30:442–452. [DOI] [PubMed] [Google Scholar]
- 7. Krestan C, Hojreh A. Imaging of insufficiency fractures. Eur J Radiol. 2009;71:398–405. [DOI] [PubMed] [Google Scholar]
- 8. Ishibashi Y, Okamura Y, Otsuka H, Nishizawa K, Sasaki T, Toh S. Comparison of scintigraphy and magnetic resonance imaging for stress injuries of bone. Clin J Sport Med. 2002;12:79–84. [DOI] [PubMed] [Google Scholar]
- 9. Stafford SA, Rosenthal DI, Gebhardt MC, Brady TJ, Scott JA. MRI in stress fracture. Am J Roentgenol. 1986;147:553–556. [DOI] [PubMed] [Google Scholar]
- 10. Sofka CM. Imaging of stress fractures. Clin Sport Med. 2006;25:53–62. [DOI] [PubMed] [Google Scholar]
- 11. Bodner G, Stöckl B, Fierlinger A, et al. Sonographic findings in stress fractures of the lower limb: preliminary findings. Eur Radiol. 2005;15:356–359. [DOI] [PubMed] [Google Scholar]
- 12. Banal F, Gandjbakhch F, Foltz V, et al. Sensitivity and specificity of ultrasonography in early diagnosis of metatarsal bone stress fractures: a pilot study of 37 patients. J Rheumatol. 2009;36:1715–1719. [DOI] [PubMed] [Google Scholar]
- 13. Khy V, Wyssa B, Bianchi S. Bilateral stress fracture of the tibia diagnosed by ultrasound: a case report. J Ultrasound. 2012;15:130–134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Jones SL, Phillips M. Early identification of foot and lower limb stress fractures using diagnostic ultrasonography: a review of three cases. Foot Ankle Online J. 2010;3:3. [Google Scholar]
- 15. Greaney RB, Gerber FH, Laughlin RL, et al. Distribution and natural history of stress fractures in U.S. Marine recruits. Radiology. 1983;146:339–346. [DOI] [PubMed] [Google Scholar]
- 16. Fredericson M, Bergman AG, Hoffman JL, Dillingham MS. Tibial stress reaction in runners. Correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med. 1995;23:472–481. [DOI] [PubMed] [Google Scholar]
- 17. Blankstein A. Ultrasound in the diagnosis of clinical orthopedics: the orthopedic stethoscope. World J Orthop. 2011;2:13–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Backhaus M, Burmester G, Gerber T, et al. Guidelines for musculoskeletal ultrasound in rheumatology. Ann Rheum Dis. 2011;60:641–649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Patel DS, Roth M, Kapil N. Stress fracture: diagnosis, treatment, and prevention. Am Fam Physician. 2011;83:39–46. [PubMed] [Google Scholar]
- 20. Arni D, Lambert V, Delmi M, Bianchi S. Insufficiency fracture of the calcaneum: sonographic findings. J Clin Ultrasound. 2009;37:424–427. [DOI] [PubMed] [Google Scholar]
- 21. Pohl M, Mullineaux D, Milner C, Hamill J, Davis IS. Biomechanical predictors of retrospective tibial stress fractures in runners. J Biomech. 2008;41:1160–1165. [DOI] [PubMed] [Google Scholar]
- 22. Warden S, Burr D, Brukner P. Stress fractures: pathophysiology, epidemiology, and risk factors. Curr Osteoporos Rep. 2006;4:103–109. [DOI] [PubMed] [Google Scholar]