

Abstract
Background
Oral hygiene care is of key importance among stroke patients to prevent complications that may compromise rehabilitation or potentially give rise to life-threatening infections such as aspiration pneumonia.
Objective
The aim of this study was to evaluate the effectiveness of a Web-based continuing professional development (CPD) program on “general intention” of the health carers to perform daily mouth cleaning for stroke patients using the theory of planned behavior (TPB).
Methods
A double-blind cluster randomized controlled trial was conducted among 547 stroke care providers across 10 hospitals in Malaysia. The centers were block randomized to receive either (1) test intervention (a Web-based CPD program on providing oral hygiene care to stroke patients using TPB) or (2) control intervention (a Web-based CPD program not specific to oral hygiene). Domains of TPB: “attitude,” “subjective norm” (SN), “perceived behavior control” (PBC), “general intention” (GI), and “knowledge” related to providing oral hygiene care were assessed preintervention and at 1 month and 6 months postintervention.
Results
The overall response rate was 68.2% (373/547). At 1 month, between the test and control groups, there was a significant difference in changes in scores of attitude (P=.004) and subjective norm (P=.01), but not in other TPB domains (GI, P=.11; PBC, P=.51; or knowledge, P=.08). At 6 months, there were significant differences in changes in scores of GI (P=.003), attitude (P=.009), SN (P<.001) and knowledge (P=.001) between the test and control groups. Regression analyses identified that the key factors associated with a change in GI at 6 months were changes in SN (beta=.36, P<.001) and changes in PBC (beta=.23, P<.001).
Conclusions
The Web-based CPD program based on TPB increased general intention, attitudes, subjective norms, and knowledge to provide oral hygiene care among stroke carers for their patients. Changing subjective norms and perceived behavioral control are key factors associated with changes in general intention to provide oral hygiene care.
Trial Registration
National Medical Research Register, Malaysia NMRR-13-1540-18833 (IIR); https://www.nmrr.gov.my/ fwbLoginPage.jsp
Keywords: oral hygiene; computer-aided learning; cerebrovascular accident; theory of planned behavior; health care providers, Internet
Introduction
Provision of oral hygiene care is often underemphasized and underpracticed in the acute hospital setting [1]. This is despite growing acceptance of the importance of oral hygiene to general health, because of its potential link with bacteremia and aspiration pneumonia [2,3]. For stroke patients in the acute hospital setting, it is recognized that oral hygiene care is of key importance to prevent complications that may compromise rehabilitation or potentially give rise to a recurrent stroke [4]. There is a growing interest in how to effectively increase the practice of providing oral hygiene care in the hospital setting through clinical interventions [5,6] and through education and training of caregivers [7,8]. Unfortunately, however, all this has met with limited success and a persistence of poor knowledge and attitudes toward providing oral hygiene care in the acute hospital setting typically prevails [9].
Despite the acknowledged importance of dental education and oral health promotion activities, the effectiveness to change practices with respect to oral hygiene care has met with limited success among carers and patients [10,11]. To this end, the need to plan and implement oral health promotion programs based on psychological models has advocated the need to “translate theory into practice” [12]. One of the most widely used theories (model) is the theory of planned behavior (TPB), which emphasizes the importance of changing the “general intention”’ (GI) to perform a health behavior and its relationship to attitude (positive or negative views of a behavior), subjective norm (SN, perceived of social pressure to perform a behavior) and perceived behavior control (PBC, one’s control to perform a behavior) [13,14].
Providing dental health education and oral health promotion through continuing professional development (CPD) programs is an important and practical way to promote oral hygiene care practices in hospital settings [15]. The use of Web-based and computer-aided learning (CAL) has been widely used in CPD programs for health carers, owing to its ability to implement programs across wide geographical areas at relatively low costs and because of the reported effectiveness of such programs in changing health care practices [16-20] and health behavior [21]. Increasingly, Web-based and CAL programs are being used to enhance oral hygiene care in hospital and other institutionalized setting, and there are several reports of their ability to positively bring about change in knowledge [22], attitudes [18], and oral health behavior [23].
We aimed to evaluate the effectiveness of a Web-based (CPD) program to change the GI of health carers to perform daily mouth cleaning for stroke patients using TPB in a large randomized controlled trial across Malaysia. In addition, the study aimed to identify key factors associated with changes in GI among health care workers to provide oral hygiene care to stroke patients.
Methods
Study Design and Sample
This study was a double-blind, cluster-randomized, controlled trial with 1 month and 6 months follow-ups. The study involved 10 public hospitals in Malaysia, which have participated in a survey of oral hygiene practice for stroke patients. These hospitals were selected because they provide rehabilitation services that are led by rehabilitation medicine specialists. Hospitals were first stratified by size into either large, medium, or small in terms of number of health care providers. From each stratified group, hospitals were block-randomized in groups of 4 (“ABBA”) by a computer-generated randomization method. In total, 5 hospitals were assigned to the test group (277 registered nurses) and 5 hospitals were assigned to the control group (270 registered nurses). The allocation sequence was concealed from the investigator coordinating the trial (who had contact with the centers). Through concealment, the assessor was “blind” as to what group participants had been assigned and participants were also blind as to what groups they were assigned to, as both received a form of Web-based CPD.
The study population was registered nurses caring for stroke patients at the hospitals, mainly from the rehabilitation and general medical wards. All the registered nurses from these identified wards were invited to take part in this trial. Information sheet related to the study and written informed consent were given to all the nurses before commencing the study. The forms were distributed to the nurses by the ward managers or chief nurses. Nurses who provided their written consent were those who participated in the trial from the study population. Participation was voluntary and no contact was made with the nurses to ensure confidentiality and reduce the potential for “social bias.”
Ethics Approval
This clinical trial was registered with the National Institutes of Health, Ministry of Health, Malaysia; NMRR-13-1540-18833(IIR). Before the commencement of the study, ethical approval was obtained from the Institute for Health Behavioral Research and Medical Research and Ethics Committee of the National Institutes of Health, Ministry of Malaysia. Permissions to conduct the study were also obtained from the directors of the respective hospitals. Recruitment and baseline assessments were from September 2014 to November 2014 at 10 hospitals across the country (both the Peninsular Malaysia and island of Borneo Malaysia). This study followed CONSORT guidelines.
Data Collection
The nurses self-completed a questionnaire on the practice of providing oral hygiene care to stroke patients, which contained 12 items specific to attitudes, SN, PBC, and GI to providing oral hygiene care related to TPB. These items were derived from the manual of “Constructing Questionnaires Based on the Theory of Planned Behavior” developed by the Centre of Health Services Research, University of New Castle, UK (2004) [24]. Items related to direct measure of the domains were chosen and modified to the oral health context. For example, in the GI domain, “I expect to measure the blood pressure of my patients with diabetes in each consultation” was modified to “I expect to perform oral care (including denture) for patients in every session.” Each domain had 3 items that were rated on a 5-point Likert scale (strongly disagree, disagree, not disagree or agree, agree, and strongly agree). Domain scores can range from 3 to 15, with higher scores reflecting more positive attitude, stronger subjective norms, greater perceived behavior control, and greater general intention to provide oral hygiene care. Sociodemographic and environmental characteristic (eg, attended oral care training, availability of oral health guidelines and oral hygiene kits, and having dental professional support in the ward) information were also obtained from the participants.
In addition, knowledge of oral health care was assessed using 5 items related to dental plaque, gum bleeding, consequences of dental plaque, how to prevent gingivitis, and how oral health affects general health [25]. Knowledge scores can range from 0 to 5, with higher scores indicative of greater oral health knowledge. Assessments were carried out preintervention and at 1 month and 6 months postintervention.
Intervention
A Web-based CPD program was developed for the test and control groups. The test group program was specific to provision of oral hygiene care to stroke patients and covered details of oral health knowledge, attitudes, subjective norms, means of behavioral control, and intention (ie, based on TPB). The test group contents include, for example, information on good oral condition and the importance of having good oral health, the consequences of poor oral hygiene, and the importance of nurse’s roles and care of stroke patients. The development of the contents was guided by the definition of the TPB domains and scope of the study. The control group received an analogous Web-based CPD program related to “bundles of care” for stroke patients that included some details on oral hygiene care but not specific to TPB [26]. The CPD programs were developed by stroke physicians (rehabilitation medicine) and dentists and followed good practices of CAL for oral health [27]. Following the assignment to the groups, the participants were provided with details of the Web-based programs through a secure internet portal. Participants were reminded and encouraged to complete the Web-based CPD program every 6 weeks.
Sample Size
With the assumption that this practice is at 50% and that it will not change without education intervention, whereas there will be a 25% improvement in practices following CAL intervention (ie, 63% of nurses will practice oral care in rehabilitation). Then a proposed sample size of 247 in each group is required with sample power at 80%. Allowing for nonparticipation and a dropout rate of ~20%, thus it was prudent to attempt to recruit over 600 nurses (300 per group) in total to test the hypothesis.
Data Analysis
The changes in knowledge, attitudes, SN, PBC, and GI were determined overtime and compared between the test and control groups using Friedman two-way analysis of variance (ANOVA) and Mann-Whitney U test analysis, respectively. Multiple linear regression analyses were performed to determine key factors associated with changes in GI to provide oral hygiene care at 1 month and 6 months.
Results
The response rate of the trial was 68.2% (373/547); mostly loss to follow-up was because nurses were transferred to other wards or hospitals (Figure 1). The response rate among the test group was 70.4% (195/277) and among the control group was 65.0% (178/270); there was no significant difference between the response rate among those in the test and control groups (P>.05). The majority of nurses were female (95.7%, 357/373), had a certificate or diploma in nursing (81.5%, 304/373), worked in general medical wards (78.6%, 293/373), and reported to have worked for less than 5 years (59.0%, 220/373; Table 1).
Figure 1.
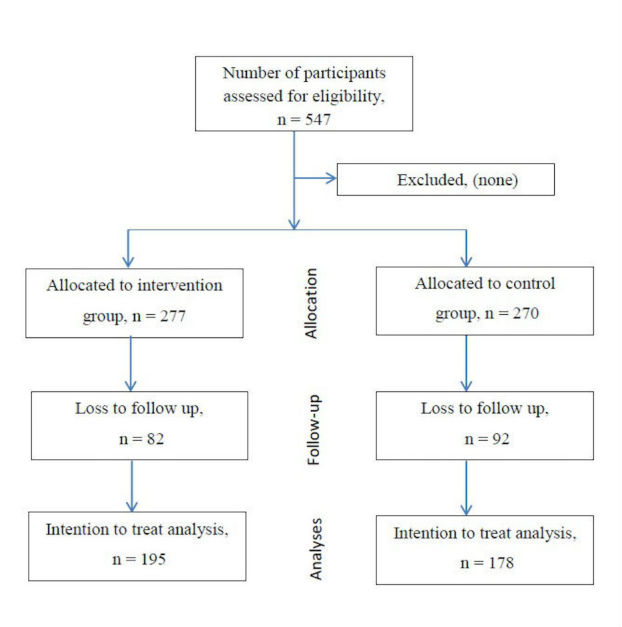
Flow diagram phases of the two-group randomized controlled trial.
Table 1.
Health care provider and environmental characteristics (n=373)
| Characteristics | n (%) | |||
| Provider characteristics |
|
|
||
|
|
Gender |
|
|
|
|
|
|
Male | 16 (4.3) | |
|
|
|
Female | 357 (95.7) | |
|
|
Years worked |
|
|
|
|
|
|
Less than 5 years | 220 (59.0) | |
|
|
|
More than 5 years | 153 (41.0) | |
|
|
Qualification |
|
|
|
|
|
|
Certificate or diploma | 304 (81.5) | |
|
|
|
Post basic or degree | 69 (18.5) | |
|
|
Working wards |
|
|
|
|
|
|
Rehabilitation ward | 80 (21.4) | |
|
|
|
Medical ward | 293 (78.6) | |
| Environmental |
|
|
|
|
|
|
Oral care training |
|
|
|
|
|
|
Yes | 108 (29.0) | |
|
|
|
No | 265 (71.0) | |
|
|
Oral health care guidelines |
|
|
|
|
|
|
Yes | 296 (79.4) | |
|
|
|
No | 77 (20.6) | |
|
|
Oral hygiene kit |
|
|
|
|
|
|
Yes | 253 (67.8) | |
|
|
|
No | 120 (32.2) | |
|
|
Dental professional support |
|
|
|
|
|
|
Yes | 52 (13.9) | |
|
|
|
No | 321 (86.1) | |
Among all participants, there was a significant difference in knowledge scores over time (P<.05; Table 2). There was a significant improvement in knowledge scores between baseline and 1 month (P<.01), but no significant change between baseline and 6 months (P>.05), and between 1 month and 6 months (P>.05).
Table 2.
Changes in knowledge and theory of planned behavior domains scores over time.
| Time | General intention Mean (SD) |
Attitudes Mean (SD) |
Subjective norm Mean (SD) |
Perceived behavior control Mean (SD) |
Knowledge Mean (SD) |
| Baseline | 10.8 (2.1) | 13.1 (1.7) | 9.7 (1.7) | 10.5 (1.7) | 3.0 (1.0) |
| 1 month | 11.0 (1.9) | 12.9 (1.6) | 9.9 (1.7) | 10.3 (1.9) | 3.2 (1.1) |
| 6 months | 10.7 (2.2) | 13.0 (1.6) | 9.7 (1.8) | 10.3 (1.9) | 3.2 (1.1) |
| P value | .36 | .11 | .05 | .28 | .005a |
aBaseline<1 month, P=.02.
In the test group, there was a significant difference in knowledge scores over time (P<.001; Table 3). There was a significant improvement in knowledge scores between baseline and 1 month (P<.01) and between baseline and 6 months (P<.01), but no significant change between 1 month and 6 months (P>.05). There was a significant change in GI scores between baseline and 1 month (P<.05). A significant improvement in SN scores was observed between baseline and 1 month (P<.05) and between baseline and 6 months (P<.01), but no significant change between 1 month and 6 months (P>.05). However, no significant changes over time were observed in attitude scores (P>.05) and PBC scores (P>.05).
Table 3.
Test and control group changes in knowledge and theory of planned behavior (TPB) domain scores overtime.
| Group | General intention Mean (SD) |
Attitude Mean (SD) | Subjective norm Mean (SD) | Perceived behavior control Mean (SD) | Knowledge Mean (SD) | ||
| Test group |
|
|
|
|
|
|
|
|
|
Baseline | 10.6 (2.0) | 12.9 (1.6) | 9.5 (1.7) | 10.5 (1.7) | 2.9 (1.0) | |
|
|
1 month | 11.0 (2.0) | 12.9 (1.8) | 10.0 (1.8) | 10.2 (2.1) | 3.3 (1.1) | |
|
|
6 months | 10.9 (1.9) | 13.2 (1.6) | 10.1 (1.5) | 10.2 (1.9) | 3.3 (1.1) | |
|
|
P value | .045a |
.43 | .001b |
.42 | <.001c |
|
| Control group |
|
|
|
|
|
|
|
|
|
Baseline | 11.0 (2.1) | 13.3 (1.8) | 9.8 (1.8) | 10.6(1.7) | 3.0 (1.0) | |
|
|
1 month | 11.0 (1.9) | 12.8 (1.5) | 9.7 (1.6) | 10.5 (1.6) | 3.1 (1.0) | |
|
|
6 months | 10.6 (2.5) | 12.9(1.7) | 9.3 (2.0) | 10.4 (1.8) | 3.0 (1.1) | |
|
|
P value | .03 |
.002d |
.22 |
.57 | .16 |
|
aBaseline<1 month, P=.03.
bBaseline<1 month, P=.02; Baseline<6 months, P=.004.
cBaseline<1 month, P=.009; Baseline<6 months, P=.003.
dBaseline>1 month, P=.01.
Among the control group (Table 3), there was a significant change in GI scores (P<.05) and attitude scores (P<.01), no significant changes between baseline, 1 month, and 6 months, and significant changes between baseline and 1 month with lower score at 1 month (P<.05), respectively. No significant changes over time were observed in SN scores (P>.05), PBC scores (P>.05), and knowledge scores (P>.05) among the control group.
At 1 month, between the test and control groups, there were significant differences in the change (∆) of attitude scores (P<.01) and SN scores (P<.05), but not in other TPB domains (P>.05) nor in knowledge scores (P>.05; Table 4). At 6 months, between the test and control group, there were significant differences in the change (∆) of GI scores (P<.01), attitude scores (P<.01), and SN scores (P<.001), but not in PBC (P>.05). In addition, there were significant differences in the change of knowledge scores (P<.01).
Table 4.
Changes in knowledge and theory of planned behavior domain between test and control groups from baseline to 1 month and baseline to 6 months.
| Time | ∆GI | ∆Attitude | ∆SN | ∆PBC | ∆Knowledge | |
|
|
|
Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) |
| 1 month |
|
|
|
|
|
|
|
|
Test | .42 (2.57) | .01 (2.23) | .45 (2.18) | −.33 (2.68) | .39 (1.37) |
|
|
Control | .02 (2.61) | −.47 (2.21) | −.13 (2.45) | −.07 (2.11) | .08 (1.46) |
|
|
P value | .11a | .004a | .01a | .51a | .08a |
| 6 months |
|
|
|
|
|
|
|
|
Test | .29 (2.45) | .24 (2.01) | .54 (2.16) | -.33 (2.51) | .41 (1.36) |
|
|
Control | −.40 (2.94) | −.35 (2.42) | −.51 (2.71) | −.12 (2.44) | −.08 (1.46) |
|
|
P value | .003a | .009a | <.001a | .51a | .001a |
aP values derived from the Mann–Whitney U test.
Findings of the regression analyses are presented in Table 5. At 1 month, predictors of GI were attitude at 1 month (beta= .40, P<.001) and SN at 1 month (beta= .40, P<.001). At 6 months, predictors of GI were SN at 6 months (beta= .43, P<.001) and PBC (beta= .29, P<.001). Predictors of ∆ in GI scores between baseline and 1 month were ∆ (between baseline and 1 month) in attitude (beta= .31, P<.001) and ∆ (between baseline and 1 month) in SN (beta= .34, P<.001). Predictors of ∆ in GI scores between baseline and 6 months were ∆ (between baseline and 6 months) in SN (beta= .36, P<.001) and ∆ (between baseline and 6 months) in PBC (beta= .23, P<.001; Table 6).
Table 5.
Multiple linear regression analyses to predict general intention to provide oral care at 1 month and 6 months.
| Model 1 (1 month) | Model 2 (6 months) | ||||||
| Items | Ba | SEb | P value | Ba | SEb | P value | |
| Group | −.16 | .18 | .38 | −.01 | .21 | .98 | |
| Knowledge at 1 month | .01 | .08 | .96 | .06 | .09 | .49 | |
| TPBc |
|
|
|
|
|
|
|
| Attitude at 1 month | .40 | .05 | <.001 | .10 | .06 | .12 | |
| SNd at 1 month | .40 | .05 | <.001 | .43 | .06 | <.001 | |
| PBCe at 1 month | .05 | .05 | .34 | .29 | .05 | <.001 | |
|
|
R2-adjusted model =.23 | R2-adjusted model 1=.22 | |||||
aB: parameter estimate.
bSE: standard error.
cTPB: theory of planned behavior.
dSN: subjective norm.
ePBC: perceived behavior control.
Table 6.
Multiple linear regression analyses to predict changes in general intention between baseline and 1 month, and baseline and 6 months to provide oral care
|
|
Model 3 (Baseline and 1 month) | Model 4 (Baseline and 6 months) | ||||
| Items | Ba | SEb | P value | Ba | SEb | P value |
| Group | .07 | .25 | .79 | .30 | .26 | .25 |
| ∆fKnowledge | .01 | .09 | .96 | .01 | .09 | .96 |
| TPBc |
|
|
|
|
|
|
| ∆Attitude | .31 | .06 | <.001 | .10 | .06 | .09 |
| ∆SNd | .34 | .05 | <.001 | .36 | .05 | <.001 |
| ∆PBCe | .07 | .05 | .21 | .23 | .05 | <.001 |
|
|
R2-adjusted model =.20 | R2-adjusted model 1=.21 | ||||
aB: parameter estimate.
bSE: standard error.
cTPB: theory of planned behavior.
dSN: subjective norm.
ePBC: perceived behavior control.
f∆ denotes change.
Discussion
Principal Findings
As mentioned before, there is a need to improve the practice of oral hygiene care in the acute hospital setting, and some would argue particularly for stroke patients [28-31]. CAL has been used widely to deliver information and educate patients and caregivers in the medical field but few were reported to be related to oral health [32,33]. Thus, this study aimed to evaluate the effectiveness of a Web-based (CPD) program to change the GI of health carers to perform daily mouth cleaning for stroke patients using TPB and to identify the key factors associated with changes in GI among health care workers to provide oral hygiene care to stroke patients. Increasingly, there are calls to consider theory-based health promotion strategies in implementing programs and to provide evidence of whether theory does, in fact, dictates practice [34,35].
This study provided support for the application of TPB among stroke carers to perform oral care daily. Over time, in the test group, there was evidence of significant improvements in general intentions to perform oral hygiene care, SN, and knowledge. Even by 1 month, there was a significant improvement in GI, SN, and knowledge, and between 1 month and 6 months this persisted. Whereas in the control group there was a significant change in GI and attitudes, but it was transient; a significant difference was between 1 month and baseline but not between 6 months and baseline. At 1 month, there were significant differences in the change of attitude scores and in the change of SN scores between the test and control groups. By 6 months, significant differences in the change in GI, attitudes, and SN to provide oral hygiene care were evident in all TPB domains except in PBC. In addition, a significant difference in the change of knowledge scores over the 6-month period was also evident between the test and control groups. This provides evidence of the effectiveness of the Web-based intervention and suggests that its effectiveness increases over time. Nonetheless, PBC did not significantly change. It is plausible that this may take longer to change or needs to be supported by environment changes [36].
Regression analyses identified that the key factors associated with GI (to provide oral hygiene care) at 1 month were attitudes (at 1 month) and SN (at 1 month); and that general intention at 6 months was associated with SN (at 6 months) and PBC (at 6 months). Furthermore, the change in GI (between baseline and 1 month) was associated with the changes that occurred in attitudes and SN; and the change in GI (between baseline and 6 months) was associated with the changes that occurred in SN and PBC. The fact that several of TPB domain scores were associated with GI at the respective time periods and that the changes in several of the TPB scores were associated with changes in GI at the respective periods provide evidence of the interrelationship between domains of TPB and GI as the theory hypothesizes. The findings of this trial support other findings with respect to predictors of GI at specific time periods [37] and changes in GI [13]. Thus in line with TPB, carers who had positive attitudes, perceived positive social pressure, and were in control of their action would have high intention of performing oral care daily to patients with stroke [13]. Of note, some domains did not change nor were some domains associated with GI or change in GI, thus the influence of the domains varies across the study [37]. This is not an unusual feature in studies as not all domain changes are associated with GI over time [38,39]. This perhaps can be attributed to the context-specific settings of the study, the type of intention, and indeed the general intention practice [40,41].
Studies have shown that a significant improvement in GI, SN, and knowledge among the participants increased their confidence in promoting oral health and educating patients [19]. A noteworthy finding of this study was that both groups were given the CAL program, but only the intervention group had detailed information on oral health related to stroke patients. Thus this contributed to a significant increase in specific knowledge and GI among the intervention group compared with the control group [18].
The study benefits from its relatively large sample size, the diverse geographical areas within a country (major centers for stroke rehabilitation), and being a double-blind randomized controlled clinical trial. The response rate was close to 70% and loss to follow-up was largely attributed to nurses having changed working environments because of being assigned to other wards or hospitals. There was no significant difference in response rate between the test and control groups.
In this trial, participants were block-randomized by hospital (stratified by size) rather than by participants to avoid the potential of bias of participants discussing the Web-based CPD program within centers. The use of Web-based CPD in both the test and control group interventions allowed for a double-blind trial. In the test group, the program was built on TPB and included specific information to promote increases in knowledge, attitudes, SN, PBC, and GI to provide oral hygiene care. Although the control group program did contain some information on oral hygiene care, it was limited and not based on the TPB.
Going forward, it would be worth investing if changes in the practice of provision of oral hygiene care do occur and that the practice is maintained over time. Furthermore, studies can be done to examine the pathways that influence changes in behavior by considering specific beliefs of TPB attributes and the impact of Web-based CPD. The impact of CPD depends on various factors such as individual carer characteristics (eg, personal compliance or interest to update themselves with new information) [42,43], and environmental factors (eg, lack of Internet access or software compatibility) [22,44]. It would also be useful to monitor engagement in the Web-based learning (which at the time keeping anonymity) to determine how this effects outcomes or indeed other methods of learning.
Conclusions
A Web-based CPD program based on TPB was effective in increasing GI to perform oral hygiene care for stroke survivors in the acute hospital setting. In addition, the program was effective in changing attitudes and SN. Furthermore, the study found that changing SNs and PBC are key factors associated with changes in GI to provide oral hygiene care. These findings support and have implications for the use of theory-based health education CPD programs and oral health promotion programs.
Acknowledgments
We would like to thank all the personnel involved in this study for their assistance and contribution. We would also like to thank the Director General of Health Malaysia for his permission to have this paper published. This study was funded by The University of Hong Kong.
Abbreviations
- CAL
computer-aided learning
- CPD
continuing professional development
- GI
general intention
- PBC
perceived behavior control
- TPB
theory of planned behavior
- SN
standard norm
Footnotes
Conflicts of Interest: None declared.
References
- 1.Friese CR, Kalisch BJ, Lee KH. Patterns and correlates of missed nursing care in inpatient oncology units. Cancer Nurs. 2013;36(6):E51–7. doi: 10.1097/NCC.0b013e318275f552. http://europepmc.org/abstract/MED/23151503 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.El-Solh AA, Pietrantoni C, Bhat A, Okada M, Zambon J, Aquilina A, Berbary E. Colonization of dental plaques: a reservoir of respiratory pathogens for hospital-acquired pneumonia in institutionalized elders. Chest. 2004 Nov;126(5):1575–82. doi: 10.1378/chest.126.5.1575.S0012-3692(15)31374-X [DOI] [PubMed] [Google Scholar]
- 3.Azarpazhooh A, Leake JL. Systematic review of the association between respiratory diseases and oral health. J Periodontol. 2006 Sep;77(9):1465–82. doi: 10.1902/jop.2006.060010. [DOI] [PubMed] [Google Scholar]
- 4.Brady M, Furlanetto D, Hunter RV, Lewis S, Milne V. Staff-led interventions for improving oral hygiene in patients following stroke. Cochrane Database Syst Rev. 2006 Oct 18;(4):CD003864. doi: 10.1002/14651858.CD003864.pub2. [DOI] [PubMed] [Google Scholar]
- 5.Lam OL, McMillan AS, Samaranayake LP, Li LS, McGrath C. Effect of oral hygiene interventions on opportunistic pathogens in patients after stroke. Am J Infect Control. 2013 Feb;41(2):149–54. doi: 10.1016/j.ajic.2012.02.020.S0196-6553(12)00268-4 [DOI] [PubMed] [Google Scholar]
- 6.Lam OL, McMillan AS, Samaranayake LP, Li LS, McGrath C. Randomized clinical trial of oral health promotion interventions among patients following stroke. Arch Phys Med Rehabil. 2013 Mar;94(3):435–43. doi: 10.1016/j.apmr.2012.10.024.S0003-9993(12)01082-9 [DOI] [PubMed] [Google Scholar]
- 7.Kuo Y, Yen M, Fetzer S, Chiang L, Shyu Y, Lee T, Ma H. A home-based training programme improves family caregivers' oral care practices with stroke survivors: a randomized controlled trial. Int J Dent Hyg. 2016 May;14(2):82–91. doi: 10.1111/idh.12138. [DOI] [PubMed] [Google Scholar]
- 8.Smith CJ, Horne M, McCracken G, Young D, Clements I, Hulme S, Ardron C, Hamdy S, Vail A, Walls A, Tyrrell PJ. Development and feasibility testing of an oral hygiene intervention for stroke unit care. Gerodontology. 2016 May 16;34(1):110–120. doi: 10.1111/ger.12232. [DOI] [PubMed] [Google Scholar]
- 9.Horne M, McCracken G, Walls A, Tyrrell PJ, Smith CJ. Organisation, practice and experiences of mouth hygiene in stroke unit care: a mixed-methods study. J Clin Nurs. 2015 Mar;24(5-6):728–38. doi: 10.1111/jocn.12665. [DOI] [PubMed] [Google Scholar]
- 10.Kay E, Locker D. A systematic review of the effectiveness of health promotion aimed at improving oral health. Community Dent Health. 1998 Sep;15(3):132–44. [PubMed] [Google Scholar]
- 11.McGrath C, Zhang W, Lo EC. A review of the effectiveness of oral health promotion activities among elderly people. Gerodontology. 2009 Jun;26(2):85–96. doi: 10.1111/j.1741-2358.2008.00232.x.GER232 [DOI] [PubMed] [Google Scholar]
- 12.Kay E, Vascott D, Hocking A, Nield H, Dorr C, Barrett H. A review of approaches for dental practice teams for promoting oral health. Community Dent Oral Epidemiol. 2016 Aug;44(4):313–30. doi: 10.1111/cdoe.12220. [DOI] [PubMed] [Google Scholar]
- 13.Ajzen I. The Theory of Planned Behaviour. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi: 10.1016/0749-5978(91)90020-T. [DOI] [Google Scholar]
- 14.Ajzen I. The theory of planned behaviour: reactions and reflections. Psychol Health. 2011 Sep;26(9):1113–27. doi: 10.1080/08870446.2011.613995. [DOI] [PubMed] [Google Scholar]
- 15.Shah N, Mathur VP, Kathuria V, Gupta T. Effectiveness of an educational video in improving oral health knowledge in a hospital setting. Indian J Dent. 2016;7(2):70–5. doi: 10.4103/0975-962X.184646. http://www.ijdentistry.com/article.asp?issn=0975-962X;year=2016;volume=7;issue=2;spage=70;epage=75;aulast=Shah .IJDENT-7-70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bachman MW, Lua MJ, Clay DJ, Rudney JD. Comparing traditional lecture vs. computer-based instruction for oral anatomy. J Dent Educ. 1998 Aug;62(8):587–91. [PubMed] [Google Scholar]
- 17.Messecar DC, Van Son C, O'Meara K. Reading statistics in nursing research: a self-study CD-ROM module. J Nurs Educ. 2003 May;42(5):220–6. doi: 10.3928/0148-4834-20030501-09. [DOI] [PubMed] [Google Scholar]
- 18.Albert D, Barracks SZ, Bruzelius E, Ward A. Impact of a Web-based intervention on maternal caries transmission and prevention knowledge, and oral health attitudes. Matern Child Health J. 2014 Sep;18(7):1765–71. doi: 10.1007/s10995-013-1421-8. [DOI] [PubMed] [Google Scholar]
- 19.George A, Duff M, Ajwani S, Johnson M, Dahlen H, Blinkhorn A, Ellis S, Bhole S. Development of an online education program for midwives in australia to improve perinatal oral health. J Perinat Educ. 2012;21(2):112–22. doi: 10.1891/1058-1243.21.2.112. http://europepmc.org/abstract/MED/23449750 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Yardley L, Miller S, Schlotz W, Little P. Evaluation of a Web-based intervention to promote hand hygiene: exploratory randomized controlled trial. J Med Internet Res. 2011;13(4):e107. doi: 10.2196/jmir.1963. http://www.jmir.org/2011/4/e107/ v13i4e107 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sassen B, Kok G, Mesters I, Crutzen R, Cremers A, Vanhees L. A web-based intervention for health professionals and patients to decrease cardiovascular risk attributable to physical inactivity: development process. JMIR Res Protoc. 2012;1(2):e21. doi: 10.2196/resprot.1804. http://www.researchprotocols.org/2012/2/e21/ v1i2e21 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.George A, Duff M, Johnson M, Dahlen H, Blinkhorn A, Ellis S, Ajwani S, Bhole S. Piloting of an oral health education programme and knowledge test for midwives. Contemp Nurse. 2014;46(2):180–6. doi: 10.5172/conu.2014.46.2.180. [DOI] [PubMed] [Google Scholar]
- 23.Jerreat M, Youssouf N, Barker C, Jagger DC. Denture care of in-patients: the views of nursing staff and the development of an educational programme on denture care. J Res Nurs. 2007 Mar 01;12(2):193–199. doi: 10.1177/1744987106074504. [DOI] [Google Scholar]
- 24.Francis JJ, Eccles MP, Johnston M, Walker A, Grimshaw J, Foy R, Kaner EF, Smith L, Bonetti D. Web.fmk. 2004. [2017-03-04]. Constructing questionnaires based on the theory of planned behaviour: A manual for health services researchers http://web.fmk.edu.rs/files/blogs/2010-11/Psihologija/Socijalna/TPB.pdf .
- 25.Al-Omiri MK, Al-Wahadni AM, Saeed KN. Oral health attitudes, knowledge, and behavior among school children in North Jordan. J Dent Educ. 2006 Feb;70(2):179–87. http://www.jdentaled.org/cgi/pmidlookup?view=long&pmid=16478932 .70/2/179 [PubMed] [Google Scholar]
- 26.Resar R, Pronovost P, Haraden C, Simmonds T, Rainey T, Nolan T. Using a bundle approach to improve ventilator care processes and reduce ventilator-associated pneumonia. Jt Comm J Qual Patient Saf. 2005 May;31(5):243–8. doi: 10.1016/s1553-7250(05)31031-2. [DOI] [PubMed] [Google Scholar]
- 27.Ab MN, Zhang J, Lam OL, Jin L, McGrath C. Effectiveness of computer-aided learning in oral health among patients and caregivers: a systematic review. J Am Med Inform Assoc. 2017 Jan;24(1):209–217. doi: 10.1093/jamia/ocw045.ocw045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Salamone K, Yacoub E, Mahoney A, Edward K. Oral care of hospitalised older patients in the acute medical setting. Nurs Res Pract. 2013;2013:827670. doi: 10.1155/2013/827670. doi: 10.1155/2013/827670. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Purvis T, Hill K, Kilkenny M, Andrew N, Cadilhac D. Improved in-hospital outcomes and care for patients in stroke research: an observational study. Neurology. 2016 Jul 12;87(2):206–13. doi: 10.1212/WNL.0000000000002834.WNL.0000000000002834 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ajwani S, Jayanti S, Burkolter N, Anderson C, Bhole S, Itaoui R, George A. Integrated oral health care for stroke patients - a scoping review. J Clin Nurs. 2016 Aug 18;:-. doi: 10.1111/jocn.13520. Epub ahead of print. [DOI] [PubMed] [Google Scholar]
- 31.Edwards M. Staff training improved oral hygiene in patients following stroke. Evid Based Dent. 2008;9(3):73. doi: 10.1038/sj.ebd.6400593.6400593 [DOI] [PubMed] [Google Scholar]
- 32.Lewis D. Computers in patient education. Comput Inform Nurs. 2003;21(2):88–96. doi: 10.1097/00024665-200303000-00010. [DOI] [PubMed] [Google Scholar]
- 33.Schittek M, Mattheos N, Lyon HC, Attström R. Computer assisted learning. A review. Eur J Dent Educ. 2001 Aug;5(3):93–100. doi: 10.1034/j.1600-0579.2001.050301.x.eje050301 [DOI] [PubMed] [Google Scholar]
- 34.Moore SE, Holaday B, Meehan N, Watt PJ. Exploring mHealth as a new route to bridging the nursing theory-practice gap. Res Theory Nurs Pract. 2015;29(1):38–52. doi: 10.1891/1541-6577.29.1.38. [DOI] [PubMed] [Google Scholar]
- 35.Newton JT. Interdisciplinary health promotion: a call for theory-based interventions drawing on the skills of multiple disciplines. Community Dent Oral Epidemiol. 2012 Oct;40(Suppl 2):49–54. doi: 10.1111/j.1600-0528.2012.00720.x. [DOI] [PubMed] [Google Scholar]
- 36.Ajzen I. Action Control. Berlin Heidelberg: Springer Berlin Heidelberg; 1985. From Intentions to Actions: A Theory of Planned Behavior; pp. 11–39. [Google Scholar]
- 37.Armitage CJ, Conner M. Efficacy of the theory of planned behaviour: a meta-analytic review. Br J Soc Psychol. 2001 Dec;40(Pt 4):471–99. doi: 10.1348/014466601164939. [DOI] [PubMed] [Google Scholar]
- 38.Plotnikoff RC, Lubans DR, Costigan SA, McCargar L. A test of the theory of planned behavior to predict physical activity in an overweight/obese population sample of adolescents from Alberta, Canada. Health Educ Behav. 2013 Aug;40(4):415–25. doi: 10.1177/1090198112455642.1090198112455642 [DOI] [PubMed] [Google Scholar]
- 39.Andrykowski MA, Beacham AO, Schmidt JE, Harper FW. Application of the theory of planned behavior to understand intentions to engage in physical and psychosocial health behaviors after cancer diagnosis. Psychooncology. 2006 Sep;15(9):759–71. doi: 10.1002/pon.1007. [DOI] [PubMed] [Google Scholar]
- 40.McDermott MS, Oliver M, Svenson A, Simnadis T, Beck EJ, Coltman T, Iverson D, Caputi P, Sharma R. The theory of planned behaviour and discrete food choices: a systematic review and meta-analysis. Int J Behav Nutr Phys Act. 2015 Dec 30;12:162. doi: 10.1186/s12966-015-0324-z. https://ijbnpa.biomedcentral.com/articles/10.1186/s12966-015-0324-z .10.1186/s12966-015-0324-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.McDermott MS, Oliver M, Simnadis T, Beck EJ, Coltman T, Iverson D, Caputi P, Sharma R. The theory of planned behaviour and dietary patterns: a systematic review and meta-analysis. Prev Med. 2015 Dec;81:150–6. doi: 10.1016/j.ypmed.2015.08.020.S0091-7435(15)00272-8 [DOI] [PubMed] [Google Scholar]
- 42.Peels DA, Bolman C, Golsteijn RH, De Vries H, Mudde AN, van Stralen MM, Lechner L. Differences in reach and attrition between Web-based and print-delivered tailored interventions among adults over 50 years of age: clustered randomized trial. J Med Internet Res. 2012;14(6):e179. doi: 10.2196/jmir.2229. http://www.jmir.org/2012/6/e179/ v14i6e179 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Norman CD, Skinner HA. eHealth Literacy: essential skills for consumer health in a networked world. J Med Internet Res. 2006 Jun;8(2):e9. doi: 10.2196/jmir.8.2.e9. http://www.jmir.org/2006/2/e9/ v8i2e9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Naganandini S, Rao R, Kulkarni SB. Survey on the use of the Internet as a source of oral health information among dental patients in Bangalore City, India. Oral Health Prev Dent. 2014;12(2):141–7. doi: 10.3290/j.ohpd.a31218.31218 [DOI] [PubMed] [Google Scholar]