

Abstract
Background
There are many mechanisms in which stress can lead to weight gain thus high a BMI. The endocrine and inflammatory pathway can directly increase abdominal adiposity. Another way in which stress leads to weight gain is through changes in health behaviors. The study aimed to investigate the prevalence of musculoskeletal disorders (MSDs) among healthy students of Ahlia University, and to determine the relationship between the development of MSDs and academic stressors and body mass index.
Methods
Self-administered questionnaires were distributed to 94 students aged 18-26 years who were enrolled at various Ahlia University colleges and met other inclusion criteria. The students responded to the standardized Nordic musculoskeletal questionnaire and the modified College Student Stress Inventory regarding musculoskeletal symptoms and academic stressors. Height and weight measurements were also obtained to determine body mass index.
Results
A total of 77.66% reported MSDs in one or more body part, with the prevalence being higher among women than among men. The 7-day prevalence of MSDs severe enough to interfere with activities of daily living was 60.64%, and 44.68% by female and male students, respectively. There was a significant relationship between academic stress and MSDs in the neck, shoulders, lower back, and hips, while the relationship between MSDs, and body mass index, academic stress, and grade point average was not significant.
Conclusions
The prevalence of MSDs among Ahlia University students was found to be high. Apart from the positive correlation between academic stress and MSDs in certain body parts, other correlations were not significant.
Keywords: Achievement, Body mass index, Daily living activity, Musculoskeletal disease, Pain measurement, Psychological stress, Survey and questionnaires
INTRODUCTION
Musculoskeletal disorders (MSDs) are defined as a group of inflammatory and degenerative conditions that affect muscles, tendons, joints, ligaments, peripheral nerves, and the supporting blood vessels [1].
MSDs are considered to be the most common cause of severe long-term pain and disability, affecting hundreds of millions of people around the world. MSDs include a large spectrum of diseases that range from acute conditions to lifelong disorders [2].
The most common type of MSDs is low back pain, which is considered to be the number one cause of disability among workers [3]. Other common MSDs include shoulder, neck, knee, and wrist pain, with a prevalence of > 10% in the selected populations [3,4].
MSDs have a financial impact. The Health and Safety Executive (HSE) in the United Kingdom has estimated that MSDs would impose a burden of £2.2 billion in the United Kingdom alone, due to associated medical costs and short and long-term work absenteeism [5].
Moreover, in developed and less developed countries, one in every four persons has chronic musculoskeletal pain [2]. The prevalence of MSDs among college students has been estimated to range between 32.9% and 89.3% in different parts of the world [6].
The pathology of MSDs has always been associated with physical risk factors, such as performing high repetition tasks, exposure to vibrations, improper posture while working, and static work posture, which increase the physical loading on the joints and soft tissues, leading to injuries. However, the severity of the injuries depends on various factors, such as the frequency, duration, and intensity of the physical exposure [1].
Other physical risk factors, such as prolonged sitting, static awkward posture, overhead work, excessive demands on the worker, and poor control over working patterns, are closely related to upper limb MSDs [7].
Recently, studies have shown that psychological risk factors might have the same impact on MSDs as do physical risk factors [8]. Psychological disorders like anxiety, high distress levels, and depression have been shown to lead to the occurrence of MSDs [9,10].
Stress, as described by the HSE (UK), is the adverse reaction that people experience when faced with excessive pressure or demands placed on them. University students are at great risk of becoming stressed due to several environmental factors, such as academic demands, examinations, finances, mental pressure, time pressure, health concerns, self-imposed stressors, and relationships with colleagues, friends, and family [11,12,13].
Stress affects both male and female students [14], and it may have either positive or negative effects. Stress can be positively used as motivator for an improved quality of life, while negative stress becomes destructive as a result of how an individual negatively perceives it and reacts to it [15]. Chronic psychosocial stress may lead to obesity through increasing cortisol secretion, caloric intake and sedentary lifestyle [16].
Further, body mass index (BMI), which is a measure of body adiposity and is described as the weight (in kilograms) divided by height (in square meters), is also known to be related to the development of MSDs [17]. It is known that people with an increased body weight (elevated BMI) tend to have more musculoskeletal pain than do people with a lower body weight. BMI has been shown to be an independent risk factor for the development of MSDs, and it can also increase the 12-month prevalence of MSDs [18].
Further, some studies have reported a relationship between MSDs and stress, and confirmed that stress, especially high levels of stress, can lead to an increase in body weight and, therefore, an increase in BMI [19]. Individuals with high levels of perceived stress and those who lead stressful lives are at a greater risk of increased BMI over time as compared to those with lower stress levels [20].
Many studies have investigated the prevalence of MSDs among students, but most studies confined their student population to a single academic program. Apart from determining the prevalence of MSDs among the students, the current study also aimed to reveal the relationship between MSDs, academic stressors, and BMI. Many studies have reported the positive effect of these two risk factors separately (academic stressors and BMI) on the development of MSDs; however, the search parameters that were used in this study did not reveal studies that investigated all three components together. In addition, there is a lack of research on this topic in Bahrain, in particular. Therefore, the current study, which aimed to investigate the prevalence of MSDs among Ahlia University students and determine the relationship between MSDs, academic stressors and BMI, may contribute valuable information to the body of research on this topic.
MATERIALS AND METHODS
A total of 134 students with ages ranging between 18–26 years from various Ahlia University colleges were recruited to participate in this study. To be included in the study, all subjects had to be enrolled in an undergraduate program at Ahlia University, Kingdom of Bahrain. In addition, they had to be relatively healthy with no diagnosed medical conditions that would cause pain.
Exclusion criteria included a history of any injury or trauma to body parts, any surgical intervention, psychological disorders prior to enrolment at the university, and severe physical disability causing pain. In addition, students with blood disorders, such as sickle cell anaemia and thalassaemia, were excluded.
The study was approved by the Ethical and Research Subcommittee from the Academic Research and Intellectual Contribution Committee, Ahlia University with ID number 2015/16001. The ethical considerations applied in this study were as follows; the subjects were provided with a detailed explanation about the content and purpose of the study and were enrolled after signing a consent form. Participation was voluntary, and subjects could withdraw from the study at any time.
1. Demographic data
A questionnaire was used to collect demographic data (i.e. age, gender, marital status, grade point average (GPA), dominant hand, BMI, academic year and academic program).
The participants were assessed by the following:
1) The standardized Nordic musculoskeletal questionnaire: This questionnaire includes an image of the human body, viewed from the back, which is divided into nine anatomical regions that are usually affected by MSDs [21]. It is a binary response questionnaire, with ‘yes’ and ‘no’ indicating the presence and absence of MSDs, respectively [9]. Participants were asked to indicate whether they had an episode of pain/discomfort in any of the body parts mentioned in the questionnaire (neck, shoulder, elbows, wrists and hands, upper back, lower back, hip, knee, ankle, and feet) in the past 12 months (period prevalence), and past 7 days (point prevalence); information on the severity of MSDs in the past 12 months (if MSDs affected their normal daily activities) was also obtained [6].
2) The Modified College Student Stress Inventory: This part of the questionnaire is extracted from the College Student Stress Inventory for Women that is based on the Student-Life Stress Inventory questionnaire, which is one of the most commonly used questionnaires for evaluating stress in undergraduate populations [22,23].
3) The questionnaire consists of two parts. Part 1 measures stress susceptibility through questions on the frequency of experiencing emotions related to stress (0 = never, 1 = rarely, 2 = sometimes, 3 = frequently, 4 = always) [23]. Part 2 of the questionnaire measures current stress levels of the subject by listing situations, such as financial troubles, graduating from university, and increased responsibility, that have been identified to be stressful to students. The subjects are then asked to indicate how stressful they found these situations (0 = not at all stressful, 1 = a little stressful, 2 = somewhat stressful, 3 = moderately stressful, 4 = very stressful) [23]. The questionnaire scores range from 0 to 52, and a score of 0–27 indicates a low response to stress, while a score of 28–52 indicates a high response to stress. Scores can also be calculated separately for each part of the questionnaire [23].
4) Weight, height, and BMI measurements were obtained for each subject in this study.
2. Statistical analysis
Descriptive and inferential statistics were applied to the collected data using SPSS version 23. Pearson correlation was used to determine the relationship between MSDs, BMI, academic stress, and GPA. An independent sample t-test for marital status comparisons and ANOVA to make comparison among academic programs were employed. The P value was set at 5%.
RESULTS
Out of 134 students recruited, 30 did not meet the inclusion criteria. The demographic data of the 94 (28 male and 66 female) students are presented in Table 1. Marital status had a significant impact (P = 0.034) in terms of academic stress, but no significant impact on BMI, or 12 month and 7 day MSD prevalence (P = 0.22, 0.08 & 0.43) respectively.
Table 1. The Demographic Data.

All values are mentioned in the table are mean ± SD and frequency (percentage). BMI: Body mass index, GPA: grade point average. *Significant difference.
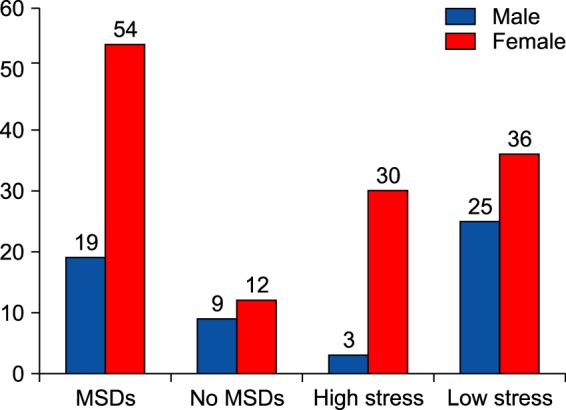
The standardized Nordic musculoskeletal questionnaire showed that seventy-three students (77.66%) reported having MSDs in one or more body parts, while 21 students (22.34%) had no complaints. The prevalence of MSDs was higher among women than among men (Fig. 1).
Fig. 1. The gender distribution of MSDS and academic stress.
The 12-month prevalence of MSDs was found to be 77.66%, with the neck being the most common site (39.36%), followed by the upper back (35.11%), lower back (34.04%) and shoulders (30.85%). Among the participants, 44.68% reported that the MSDs were severe enough to interfere with their activities of daily living, and the lower back was the most common site (18.09%) followed by the shoulders (13.83%), upper back (12.77%), and neck (11.7%). The 7-day point prevalence was found to be 60.64%, and the most common sites were both the upper and lower back (31.91%), followed by the neck (21.28%) and shoulders (15.96%) (Table 2).
Table 2. The Prevalence of MSDs among Ahlia University Students.

%: Percentage, n: Number.
The academic program showed a significant impact (F = 4.42 & P = 0.006) on MSDs development. Physiotherapy students showed a significant difference (P = 0.003) in 12-month prevalence but there was no significant difference (P = 0.6) among all programs at 7-day point prevalence.
The level of academic stress according to the Modified College Student Stress Inventory ranged between 2 and 43 (mean, 23.28 ± 8.90). Of the participants, 61 (64.89%) were within the low stress category and 33 (35.10%) were within the high stress category. The prevalence of academic stress was higher among the female participants than among the male participants (Fig. 1)
BMI values ranged from 16.7 kg/m2 to 55.7 kg/m2 (mean, 24.8 ± 6.34 kg/m2), many students (42.55%) were within the normal range (Table 1).
Pearson correlation revealed a positive correlation between academic stress and neck, shoulder, wrist and hand, upper back, lower back, hip, knee, ankle, and feet MSDs. However, the correlation was only significant (P < 0.05) for neck, shoulder, lower back, and hip MSDs. In contrast, a negative correlation was observed between academic stress and elbow MSDs, but it was not statistically significant (P > 0.05) (Table 3).
Table 3. The Relationship between Academic Stress, BMI and MSDs.

BMI: Body mass index. *Positive significant relationship, †Negative relationship.
There was a positive correlation between BMI and MSDs in all body parts (neck, shoulders, elbow, wrists and hands, upper back, lower back, knees, ankles, and feet), with the exception of the hips, for which a negative correlation was observed. However, none of the correlations were statistically significant (Table 3).
A negative correlation, although not statistically significant (P = 0.85), was observed between academic stress and BMI. A positive correlation was found between academic stress and GPA, but it was not significant (P = 0.26).
DISCUSSION
The 12-month period prevalence of 77.66% observed in the current study falls within the range of 32.9% to 89.3% reported by other studies that investigated the prevalence of MSDs in undergraduate university students, worldwide [6]. With regard to the 12-month period prevalence, the most commonly reported body part was the neck with a prevalence of 39.36% followed by the upper back (35.11%), lower back (34.04%), shoulders (30.85%), wrists and hands (20.21%), and knees (19.15%). Further, 44.68% of the participants reported that the pain was severe enough to interfere with their activities of daily living, and low back pain was found to be the most common cause.
The current results were somewhat consistent with the findings of Hayes and Smith, who reported a prevalence of 64.3% for neck pain, followed by pain in the lower back (57.9%), shoulders (48.4%), wrists and hands (42%), upper back (41.2%), and knees (26.2%) among dental hygiene students in an Australian university [24].
Abledu and Offei [6] also reported a similar 12-month period prevalence of 70.1% among undergraduate nursing students in Ghana, with neck pain being the most common (28%) followed by pain in the upper back (27.4%), lower back (23.6%), wrists and hands (22.9%), and hips and thighs (21%); in addition, 56.1% reported functional impairment due to pain.
In the current study, the 7-day point prevalence was 60.64%, with the most common sites being the upper and lower back (31.91%) followed by the neck (21.28%) and shoulders (15.96%). Smith et al. [25], reported a very similar 7-day prevalence of 67.6% among Chinese medical students, with low back pain being the most common (20.8%) followed by the knees and neck (12.1%).
In addition, Abledu and Offei [6], reported a point prevalence of 44.6% among freshmen nursing students, with wrist and hand and low back pain having the highest rate (15.3%) followed by upper back (14%) and neck pain (13.4%). With regard to differences between the sexes, the prevalence of MSDs was higher among women (81.8%) than among men (67.9%). This finding was supported by a previous study, which also reported the same association [26].
Ekpenyong et al. [26] found that MSDs were common in both male and female undergraduate Nigerian students, but the association between MSDs and the female sex was higher, with 64.8% of all female participants reporting musculoskeletal conditions as compared to only 35.2% of all male participants.
The observed higher prevalence among the female sex can be attributed to the comparatively smaller body frame and reduced muscle tone of females [27].
In contrast, in a study conducted on Australian subjects aged between 20 and 64 years, a negative association was found between the female sex and MSDs, indicating a lower prevalence of MSDs among females [28].
In addition, Abledu and Offei [6] reported no significant difference in the prevalence of MSDs between male and female freshmen Ghanaian nursing students.
In the current study, 35.1% of students were within the high academic stress category, with the prevalence being significantly higher among women (45.45% of all female participants) as compared to men (10.71% of all male participants). These results are supported by previous studies, which also found differences between the sexes with regard to perceived academic stress [26,29].
Sani et al. [29] reported a stress prevalence of 71.9% among medical students in Jizan University in Saudi Arabia, with a higher prevalence among females (77%) than among males (64%).
In the study by Ekpenyong et al. [26] 33.26% of undergraduate students reported high levels of stress, and the prevalence was higher among females (35.1%) than among males (30.7%). These values increased at the time of undergoing academic examinations to 43% in females and 38.4% in males, and this difference in perceived academic stress was attributed to the fact that women are psychologically predisposed to depression; anxiety disorders; and chronic pain, which might be sex-hormone mediated.
The current study revealed a positive relationship between academic stress and MSDs in all body parts, except the elbows; however, the relationship was only significant for neck, shoulder, lower back, and hip MSDs. This positive correlation can be attributed to psychological stress leading to an increase in muscle tension, especially in central body areas such as the neck and shoulder, thus increasing the risk of MSDs [30,31]. This finding was supported by the study of Nahit et al. [10], which reported a general musculoskeletal sensitivity to mental stress. Another study reported a strong association between the upper limbs and psychologically induced MSDs [9].
Smith et al. [25] showed that Chinese medical students who reported higher levels of mental pressure were 2.9 times more likely to develop low back pain over 12 months, thus indicating that high mental pressure is a risk factor for low back pain.
The relationship between BMI and MSDs observed in this study shows that BMI is positively associated with MSDs in all body parts, except the hip; however, the relationships were not statistically significant. This non-significant correlation can be explained as the majority of the current study participants (42.55%) had normal BMI. So their BMI was not a risk factor for developing MSDs and including more subjects with higher BMI is needed to test this relationship further. There is debate about BMI and MSD correlation, as some found no association [25] while other study found that higher BMI correlated to MSD development, especially in the lower extremities with a lower rate of recovery [18].
The current study showed no significant relationship between BMI and academic stress. The same finding was observed in a previous study applied to biomedical students in Kuala Lumpur [32]. In contrast, another study reported that individuals with higher levels of perceived stress and those who had experienced stressful life events had higher BMI values, and had greater mean changes in BMI as compared to those with lower stress levels after a 5-year follow-up [20].
The present study showed no significant relationship between academic stress and GPA. However, Inam et al. [33] reported that students with low to moderate levels of stress had a higher academic performance, and students with extreme levels of stress showed a decrease in academic performance as compared to non-stressed students. On the contrary, it was found that higher levels of stress were significantly associated with lower academic performance among undergraduate students in Wollongong University and New South Wales, Australia [34].
Regarding the impact of academic program in respect to academic stress and 12 month MSD prevalence, physiotherapy student' rates were higher than those in other programs. This is supported in the literature [6,25,29] as it is a medical program, and it can be attributed to the physical stress of clinical training and the long study hours demanded in this specialty. The strength of the current study is the comparison made among different academic program as the previous studies concentrated on only one discipline.
The current study concluded that the prevalence of MSDs and academic stress was high among the study participants, with a positive correlation between academic stress and MSDs in some body parts. However, there were no significant relationship between MSDs and BMI, BMI and academic stress, and academic stress and GPA. Academic stress should be considered when evaluating young adults with musculoskeletal disorders.
1. Limitations
The results of this study are limited because of the use of a self-reported questionnaire which is affected by the subject status of the students and a recall bias. Most of the subjects had a normal BMI, and there was an unequal number of males and females. Also, Physical activity level was not included, but should be considered in future research.
ACKNOWLEDGEMENTS
The authors would like to thank the students of Ahlia University for their participation in the study.
Footnotes
CONFLICT OF INTEREST: The authors declare that they have no competing interests.
References
- 1.Bernard BP, editor. Musculoskeletal disorders and workplace factors: a critical review of epidemiologic evidence for work-related musculoskeletal disorders of the neck, upper extremity, and low back. Washington, D.C.: U.S. Department of Health and Human Services; 1997. pp. 97–141. [Google Scholar]
- 2.Woolf AD, Akesson K. Understanding the burden of musculoskeletal conditions. The burden is huge and not reflected in national health priorities. BMJ. 2001;322:1079–1080. doi: 10.1136/bmj.322.7294.1079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences, consequences and risk groups, the DMC(3)-study. Pain. 2003;102:167–178. doi: 10.1016/s0304-3959(02)00372-x. [DOI] [PubMed] [Google Scholar]
- 4.Guo HR, Chang YC, Yeh WY, Chen CW, Guo YL. Prevalence of musculoskeletal disorder among workers in Taiwan: a nationwide study. J Occup Health. 2004;46:26–36. doi: 10.1539/joh.46.26. [DOI] [PubMed] [Google Scholar]
- 5.Deeney C, O'Sullivan L. Work related psychosocial risks and musculoskeletal disorders: potential risk factors, causation and evaluation methods. Work. 2009;34:239–248. doi: 10.3233/WOR-2009-0921. [DOI] [PubMed] [Google Scholar]
- 6.Abledu JK, Offei EB. Musculoskeletal disorders among first-year Ghanaian students in a nursing college. Afr Health Sci. 2015;15:444–449. doi: 10.4314/ahs.v15i2.18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Walker-Bone K, Cooper C. Hard work never hurt anyone: or did it? A review of occupational associations with soft tissue musculoskeletal disorders of the neck and upper limb. Ann Rheum Dis. 2005;64:1391–1396. doi: 10.1136/ard.2003.020016. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 8.Warren N. Causes of musculoskeletal disorders in dental hygienists and dental hygiene students: a study of combined biomechanical and psychosocial risk factors. Work. 2010;35:441–454. doi: 10.3233/WOR-2010-0981. [DOI] [PubMed] [Google Scholar]
- 9.Magnavita N, Elovainio M, De Nardis I, Heponiemi T, Bergamaschi A. Environmental discomfort and musculoskeletal disorders. Occup Med (Lond) 2011;61:196–201. doi: 10.1093/occmed/kqr024. [DOI] [PubMed] [Google Scholar]
- 10.Nahit ES, Hunt IM, Lunt M, Dunn G, Silman AJ, Macfarlane GJ. Effects of psychosocial and individual psychological factors on the onset of musculoskeletal pain: common and site-specific effects. Ann Rheum Dis. 2003;62:755–760. doi: 10.1136/ard.62.8.755. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ross SE, Niebling BC, Heckert TM, Teresa MH. Sources of stress among college students. Coll Stud J. 1999;33:312–317. [Google Scholar]
- 12.Ekpenyong CE, Davis KJ, Akpan UP, Daniel NE. Academic stress and menstrual disorders among female undergraduates in Uyo, South Eastern Nigeria - the need for health education. Niger J Physiol Sci. 2011;26:193–198. [PubMed] [Google Scholar]
- 13.Westerman GH, Grandy TG, Ocanto RA, Erskine CG. Perceived sources of stress in the dental school environment. J Dent Educ. 1993;57:225–231. [PubMed] [Google Scholar]
- 14.Salami SO. Psychological correlates of career indecision among secondary school adolescents. Niger J Appl Psychol. 2001;6:116–125. [Google Scholar]
- 15.Blonna R. Coping with stress in a changing world. 3rd ed. Boston (MA): McGraw Hill; 2005. pp. 254–268. [Google Scholar]
- 16.Wurtman RJ, Wurtman JJ. Carbohydrates and depression. Sci Am. 1989;260:68–75. doi: 10.1038/scientificamerican0189-68. [DOI] [PubMed] [Google Scholar]
- 17.Yang TC, Matthews SA, Chen VY. Stochastic variability in stress, sleep duration, and sleep quality across the distribution of body mass index: insights from quantile regression. Int J Behav Med. 2014;21:282–291. doi: 10.1007/s12529-013-9293-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Viester L, Verhagen EA, Oude Hengel KM, Koppes LL, van der Beek AJ, Bongers PM. The relation between body mass index and musculoskeletal symptoms in the working population. BMC Musculoskelet Disord. 2013;14:238. doi: 10.1186/1471-2474-14-238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dallman MF, Pecoraro N, Akana SF, La Fleur SE, Gomez F, Houshyar H, et al. Chronic stress and obesity: a new view of “comfort food”. Proc Natl Acad Sci U S A. 2003;100:11696–11701. doi: 10.1073/pnas.1934666100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Harding JL, Backholer K, Williams ED, Peeters A, Cameron AJ, Hare MJ, et al. Psychosocial stress is positively associated with body mass index gain over 5 years: evidence from the longitudinal AusDiab study. Obesity (Silver Spring) 2014;22:277–286. doi: 10.1002/oby.20423. [DOI] [PubMed] [Google Scholar]
- 21.Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18:233–237. doi: 10.1016/0003-6870(87)90010-x. [DOI] [PubMed] [Google Scholar]
- 22.Gadzella BM, Baloglu M. Confirmatory factor analysis and internal consistency of the student-life stress inventory. J Instr Psychol. 2001;28:84. [Google Scholar]
- 23.Brown AL, Blankson N. Developing the college student stress inventory for black women (CSSI-BW) Pap Pub. 2013;2:Article 5. [Google Scholar]
- 24.Hayes MJ, Smith DR, Cockrell D. Prevalence and correlates of musculoskeletal disorders among Australian dental hygiene students. Int J Dent Hyg. 2009;7:176–181. doi: 10.1111/j.1601-5037.2009.00370.x. [DOI] [PubMed] [Google Scholar]
- 25.Smith DR, Wei N, Ishitake T, Wang RS. Musculoskeletal disorders among Chinese medical students. Kurume Med J. 2005;52:139–146. doi: 10.2739/kurumemedj.52.139. [DOI] [PubMed] [Google Scholar]
- 26.Ekpenyong CE, Daniel NE, Aribo EO. Associations between academic stressors, reaction to stress, coping strategies and musculoskeletal disorders among college students. Ethiop J Health Sci. 2013;23:98–112. [PMC free article] [PubMed] [Google Scholar]
- 27.Khan SA, Chew KY. Effect of working characteristics and taught ergonomics on the prevalence of musculoskeletal disorders amongst dental students. BMC Musculoskelet Disord. 2013;14:118. doi: 10.1186/1471-2474-14-118. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kortt M, Baldry J. The association between musculoskeletal disorders and obesity. Aust Health Rev. 2002;25:207–214. doi: 10.1071/ah020207. [DOI] [PubMed] [Google Scholar]
- 29.Sani M, Mahfouz MS, Bani I, Alsomily AH, Alagi D, Alsomily NY, et al. Prevalence of stress among medical students in Jizan University, Kingdom of Saudi Arabia. Gulf Med J. 2012;1:19–25. [Google Scholar]
- 30.Sjøgaard G, Lundberg U, Kadefors R. The role of muscle activity and mental load in the development of pain and degenerative processes at the muscle cell level during computer work. Eur J Appl Physiol. 2000;83:99–105. doi: 10.1007/s004210000285. [DOI] [PubMed] [Google Scholar]
- 31.Westgaard RH, Jensen C, Hansen K. Individual and work-related risk factors associated with symptoms of musculoskeletal complaints. Int Arch Occup Environ Health. 1993;64:405–413. doi: 10.1007/BF00517946. [DOI] [PubMed] [Google Scholar]
- 32.Mohd Saat NZ, Ishak I, Lubis SH, Wen SH, Mohd SN, Zakaria NS, et al. Stress and its relationship with body mass index among biomedical science students in Kuala Lumpur, Malaysia. ASEAN J Psychiatr. 2010;11:190–197. [Google Scholar]
- 33.Inam QU, Shireen E, Haider S, Haleem DJ. Perception of academic examination stress: effects on serum leptin, cortisol, appetite and performance. J Ayub Med Coll Abbottabad. 2011;23:97–99. [PubMed] [Google Scholar]
- 34.Akgun S, Ciarrochi J. Learned resourcefulness moderates the relationship between academic stress and academic performance. Educ Psychol. 2003;23:287–294. [Google Scholar]