

Abstract
Background
Distracted pedestrian behavior is a significant public health concern, as research suggests distracted pedestrians have significantly higher risk of injury compared to fully attentive pedestrians. Despite this, efforts to reduce distracted pedestrian behavior are scant.
Objective
Using a repeated measures experimental research design, we implemented a behavioral intervention to reduce distracted pedestrian behavior in the high-risk environment of an urban college campus and simultaneously monitored behavior on a control urban college campus not exposed to the intervention. We had two primary aims: reduce perceived vulnerability to injury among individual pedestrians and reduce distracted pedestrian behavior in the environment through a change in community-based norms.
Methods
The hallmark of the behavioral intervention was a week-long opportunity for community members to experience personally the risks of distracted pedestrian behavior by attempting to cross a virtual pedestrian environment street while text-messaging. This was supplemented by traditional and social marketing and publicity through various campus partners. A sample of 219 individuals completed self-report surveys about perceived vulnerability to distracted pedestrian injury before experiencing the distracted virtual street-crossing and again after 2 weeks and 5 months. Observational assessment of distracted pedestrian behavior was conducted at a busy intersection on the campus as well as at a control campus not exposed to the intervention at baseline, post-intervention, 10 weeks, and 6 months.
Results
The intervention achieved mixed results. Individuals exposed to texting within a simulated pedestrian environment reported changes in their intentions to cross streets while distracted and in perceived vulnerability to risk while crossing streets, but we did not witness evidence of changed community norms based on observed rates of distracted pedestrian behavior before and after the intervention compared to a control campus not exposed to the intervention.
Discussion
The intervention created some change in self-reported intentions and thoughts but did not create significant behavior change on the campus exposed to it. Further efforts to develop interventions that will yield a reduction in distracted pedestrian behavior are needed.
Keywords: distracted walking, pedestrian, virtual reality, intervention, texting
1. Introduction
Over the past decade, about 5000 American pedestrians died each year and another 200,000 were treated annually in emergency departments following a pedestrian injury (Centers for Disease Control [CDC], 2016). About 13% of fatalities were young adults, ages 15–24. Unlike many other public health outcomes, the rate of pedestrian injury in the United States increased through the late 2000s and early 2010s and has decreased only slightly over the past two years (CDC, 2016). Several factors likely play a role in pedestrian injury rate trends, but the growth of distracted behavior by both pedestrians and drivers is hypothesized to play a part (Fischer, 2015).
Cognitive science research demonstrates clearly that multitasking, or attempting to complete two cognitively complex tasks simultaneously, causes attention to and performance on one or both tasks to decrease (Kahneman, 1973). Although automatic for most adults, engagement in traffic requires substantial cognitive processing (Barton, 2006; Thomson, 2016) and the cognitive load dedicated to using mobile devices to talk, text, or browse reduces a pedestrian’s ability to focus needed cognitive effort on crossing streets safely. Beyond cognitive distraction, some types of distraction (e.g., text-messaging) diminish visual attention to the street environment. Others (e.g., listening to music) diminish aural attention. In all cases, reduced cognitive, visual, and/or aural attention impairs pedestrian safety (see Mwakalonge, Siuhi, & White, 2015; Stavrinos et al., in press for reviews).
Given current rates of pedestrian injuries, trends for increasing rates of pedestrian injuries, and the influence of distraction and inattention on pedestrian safety, the National Safety Council highlighted distracted pedestrian behavior as a public health concern in their 2015 edition of Injury Facts (National Safety Council, 2015). However, published efforts to initiate and evaluate such prevention programs are scant. A few jurisdictions worldwide have proposed “distracted walking” laws that mimic more widespread “distracted driving” regulations, but published scholarly research on their implementation or efficacy is unavailable. Similarly, mass media reports about a wide range of public health initiatives to reduce distracted walking are available, but scholarly evaluations of such efforts are unpublished. The present study was designed, therefore, to implement and empirically evaluate a behavioral effort to reduce distracted pedestrian behavior. We focused our efforts in a high-risk location, urban college campuses.
Any initiative to improve health-related behavior must be based in theory. Health behavior theories targeting individual behavior emphasize the need to educate people about their personal vulnerability/susceptibility to the health risk in order to evoke behavior change (e.g., Health Belief Model by Rosenstock, 1974; Transtheoretical Model by Prochaska & Velicer, 1997; unrealistic optimism by Weinstein, 1983, 1984). Specifically, individuals must recognize and believe the target health risk behavior could impact them personally before they alter that behavior. We sought to achieve such change through experiential exposure to the risk of distracted walking: we asked pedestrians to try texting and walking within the context of a safe virtual reality pedestrian environment.
Health behavior change can also be accomplished at the community level. In this case, theoretical models emphasize the need to change behavioral norms. We worked to accomplish a change in community-based norms by creating social contagion (also called diffusion; developed by Burt, 1987 and Rogers, 1995), or the spreading of ideas, behaviors, and practices through local communities via social networks of known individuals. An urban campus environment where intermingled social networks are common and “community” individuals live, work, and study in close geographic proximity offers an ideal setting for social contagion to create health-related behavior change, and we used both traditional face-to-face interaction and social media to accomplish our goals.
As detailed below, our intervention itself was multifaceted. The hallmark was a week-long opportunity for community members to attempt crossing a virtual street while text-messaging. Virtual pedestrian environments were situated in prominent locations in the lobbies of two major campus buildings during working hours for a full week, and students and others were encouraged to try crossing the street while distracted. We supplemented this experiential opportunity with extensive traditional and social media marketing about the risks of distracted pedestrian behavior (e.g., yard signs, local television reports, twitter and Facebook feeds) as well as campus police presence to encourage pedestrian safety and a public event on distracted pedestrian safety behavior that included the university’s cheerleading squad and mascot.
We evaluated the efficacy of the intervention, including both theory-driven goals to increase perceived vulnerability and change community norms, using a quasi-experimental repeated measures research trial with pre-test, post-test, and follow-up assessments of individual-level self-report behavior by survey and community-level observed behavior. We had two specific hypotheses: (a) that we would increase perceived vulnerability to injury while engaging in pedestrian behavior while distracted among individual pedestrians, as assessed through individualized self-report assessments and (b) that we would increase safety by decreasing distracted pedestrian behavior, as assessed through community-level observed behaviors.
2. Methods
2.1 Research Sites
The intervention was implemented on the campus of University of Alabama at Birmingham (UAB), a state university of about 11,000 undergraduate students located in urban Birmingham, AL. We targeted in particular the pedestrian behavior at the corner of University Boulevard and 14th Street. University Boulevard is a major thoroughfare running east-west through downtown Birmingham. It has four lanes of traffic (two lanes each direction) with a center median. 14th Street is a secondary four-lane cross-street.
Old Dominion University (ODU) served as the control campus. ODU, a state university located in urban Norfolk, Virginia, was selected based on a logic-driven process of consultation with experts to create a list of over 50 potential control campuses and then gathering data on relevant characteristics: size of student body, percentage of ethnic minority student enrollment, weather patterns, urban campus location, major thoroughfare crossing campus that is marked with crosswalks and signaled with traffic lights, student housing on one side of the major thoroughfare and classroom buildings on the other side, and secondary cross-streets present. That selection process yielded ODU as the only complete match to UAB. ODU’s observational data were collected at the corner of Hampton Boulevard and 45th Street in Norfolk. Hampton Boulevard is a major north-south thoroughfare with six lanes of traffic (three each direction), divided by a center median. 45th Street is a secondary two-lane cross-street.
2.2 General Protocol
The study had three components: observational assessment, intervention, and individualized assessment. Observational assessment was conducted in both Birmingham and Norfolk, at our targeted street corners, for four two-week segments: pre-intervention baseline (two weeks prior to the weeklong intervention), post-intervention (two weeks following the weeklong intervention), 10 week follow-up (9 and 11 weeks after the intervention; the 10th week was a holiday week for students), and 6-month follow-up (26 and 28 weeks after the intervention; the 27th week was a holiday week for students), Logistical details and behavioral outcomes from the observational assessment appear below.
The intervention was conducted only in Birmingham and lasted a week. Details appear below. The individualized assessment also was conducted only in Birmingham. For the individualized assessment, participants were recruited during the intervention to complete a behavioral survey, and then asked to complete follow-up surveys after 2 weeks and 5 months. A description of the sample and outcomes of the survey appear below. Note that the participants who completed the individualized assessment were also likely to be observed in the behavioral observation assessment, but observational assessment was conducted anonymously among the full community, so many individuals were observed who were not individually assessed and did not participate in the simulated street-crossing while texting (detailed below). Analysis of data from the two assessments was conducted independently and using different strategies appropriate to each data collection strategy.
2.3 Observational Assessment
Trained observers coded pedestrian behavior on a continuous basis during weekdays between 7:45 AM and 5:45 PM. Coding was suspended only in the case of rain or lightning. Logistically, coding was divided into 30-minute segments. Each segment was conducted from a single corner of the intersection and coders moved around the intersection counter-clockwise every 30 minutes. To reduce fatigue, coders rotated regularly.
During each 30-minute segment, coders completed three sets of observations. First, for 5 minutes they counted vehicles. Traffic counts were measured as the total number of vehicles traveling in front of the coder from left to right, on the main boulevard (University Blvd in Birmingham and Hampton Blvd in Norfolk). We multiplied the count by 12 to yield an outcome of vehicles/hour.
Second, coders spent 5 minutes recording safe and unsafe behaviors of single pedestrians crossing toward them across the main boulevard. An approaching pedestrian was selected from the opposing sidewalk following a standardized and randomized pattern (i.e., middle front pedestrian picked first, then left front, right front, middle back, left back, right back, and so on). Pedestrians were chosen regardless of whether they were crossing with or against the walk sign. That single pedestrian’s behavior was observed as he or she approached the coder, during the entirety of the time spent crossing the street from one sidewalk to the other, including across the median. After that pedestrian finished crossing and data were coded, a new pedestrian was selected for observation using the same standardized pattern. This portion of coding was labeled “individualized pedestrian coding” and yielded the following outcomes about each pedestrian and his/her crossing:
apparent gender (male, female);
estimated age (child ages 0 to 12, teen ages 13 to 17, young adult ages 18 to 34, adult ages 35 to 54, older adult ages 55 and older);
crossing with the walk sign, defined as stepping off the sidewalk into the crosswalk when the walk sign was illuminated;
looking left before stepping into the road, defined as the pedestrian turning his/her head left to look at oncoming traffic before stepping into the intersection;
entering the road in the crosswalk, defined as the pedestrian initially stepping into the crosswalk within the painted lines of the crosswalk rather than outside the lines;
looking right at the median, defined as the pedestrian turning his/her head to look right at oncoming traffic before stepping out of the median and into the roadway; and
distracted behavior while crossing, defined as a pedestrian who was distracted by talking on the phone, texting and/or looking down at the phone, wearing headphones, reading, eating, or in other visually apparent ways. Multiple distractions could be marked. Distraction was recorded if it occurred at any point during the crossing while the pedestrian was in the roadway where vehicles might pass, but not on the sidewalk or median.
Third, coders spent 15 minutes observing pedestrians crossing the primary boulevard toward them. During this 15-minute period, we sought to capture all pedestrians to determine whether they were distracted or not, and if distracted by what (talking on phone, texting/looking at phone, headphones, reading, eating, other ways). Multiple distractions could be recorded. Distraction was recorded while pedestrians crossed the roadway from the median to the corner (the second half of the roadway), allowing coders the best view since the pedestrians were the closest to them. Given very substantial pedestrian traffic occurring at ODU during peak hours, coders at that site occasionally omitted groups of pedestrians so they could record information validly. This portion of coding was labeled “all pedestrian coding”.
The final 5 minutes of each segment was used for coders to rest and move counterclockwise to the next coding corner (or to rotate to a new coder). Morning starting positions were rotated across days to assure evenness in assessing behaviors.
2.4 Intervention
The intervention lasted for a full workweek. Themed around the slogan, “Pocket and Walk It” and brightly colored graphic arts, our goal was to create a “buzz” on the UAB campus that raised awareness of the risks of distracted pedestrian behavior, encouraged social contagion to change normative behavior via face-to-face and electronic communication about the topic, and allowed the community to try distracted pedestrian behavior in the safe environment of a virtual world. We addressed reduction of all distracted pedestrian behavior but emphasized especially the risks of distraction by texting.
The hallmark of our intervention was experiential exposure to the risks of distracted texting behavior while crossing the street within a virtual pedestrian environment. Details about the virtual pedestrian environments appear elsewhere (Schwebel, McClure, & Severson, 2014; Schwebel, Combs, Rodríguez, Severson, & Sisiopiku, 2016), but briefly they were both semi-immersive environments depicting an actual street environment, moving traffic, and a wooden curb placed amidst viewing monitors. Users were immersed into the street environment and stepped down off the wooden curb when they judged the simulated roadway to be safe for crossing. At that point, the environment switched from third-person to first-person and the user viewed him/herself crossing the virtual roadway amidst still-moving simulated traffic. Aural and visual feedback about crossing safety was provided. The simulators are programmed in Unity software. Figure 1 shows a photograph of one of the virtual reality pedestrian environment systems.
Figure 1.

Photograph of virtual pedestrian environment system used in intervention
The virtual pedestrian environments were placed in prominent locations in the lobby of two large university classroom buildings located caddy-corner from each other on the target intersection of University Blvd and 14th Street. The environments were manned by study personnel from 9 AM to 6 PM, who encouraged passers-by to try walking while texting in the virtual environment. We also distributed flyers across campus throughout the week, encouraging the community to visit the virtual environments in the classroom buildings. Over 1000 people crossed the virtual street environment while texting over the course of the weeklong intervention. As expected, that experience created “buzz” and it was common during the week to overhear students and others discussing their experience in the virtual environment and encouraging others to try it.
We supplemented the virtual pedestrian environment experiential opportunity with three other intervention components. First, we promoted “Pocket and Walk It” week, including the opportunity for trying the virtual pedestrian environments, via social media. Twitter and Facebook posts were made, and the Facebook post was documented to have reached about 20,000 individuals, yielding over 6,500 video views (in the video, a UAB cheerleader stopped “Blaze”, the university’s dragon mascot character as he began to enter the street while texting and not looking for traffic). The campaign was featured also on the university’s website for the week as the “banner” headline to website visitors. Second, we promoted “Pocket and Walk It” through traditional media. Chalk templates were drawn on sidewalks and branded yard signs were placed throughout the campus area (See Figure 2 for example of media used). Three local television stations covered the event with news stories and it was reported in campus publications and social media. Third, we partnered with several organizations on campus who promoted safe walking behavior among their members; these included student life, student athletic groups, and the Pan-Hellenic societies. We also partnered with the UAB Campus Police Department, who increased their presence on street corners during the week and distributed flyers on pedestrian safety to passers-by.
Figure 2.

Example of “Pocket or Walk It” campaign branding: A “Pocket or Walk It” yard sign
ODU served as the control campus and no special pedestrian safety awareness activities occurred there.
2.5 Individualized Survey Assessment
A sample of 219 individuals at UAB who engaged in the intervention by crossing the virtual pedestrian street while texting agreed to complete a brief survey about their experience (mean age = 22.6 years, SD = 7.2, 63% female, 44% Caucasian, 33% African-American). 151 and 91 of those completed similar follow-up surveys 2 weeks and 5 months after the intervention, respectively.
All three surveys were brief. Along with basic demographic information (pre-intervention only) and background information about walking habits, the surveys addressed three topics: self-report of distracted pedestrian behavior, perceived safety while engaging in distracted pedestrian behavior, and perceptions about the intervention.
Self-reported distracted pedestrian behavior was assessed from four items, each answered on a 6-point scale (1 = never, 6 = always), asking about the frequency of engaging in crossing streets while talking on a phone, text-messaging, using mobile internet applications, and listening to music. Perceived safety while engaging in distracted pedestrian behavior was assessed also with four items using a 5-point scale (1 = very unsafe, 5 = very safe) evaluating perceptions of how the respondent feels when crossing a street and talking on a phone, text-messaging, using mobile internet applications, and listening to music.
Perceptions about the intervention were assessed through five items evaluating the experience of the intervention and whether that experience caused cognitive change and behavioral change.
2.6 Data Analysis Plan
We conducted data analysis in three primary steps. The first step analyzed the individualized survey assessment data to evaluate our first hypothesis of changes in perceived vulnerability to injury while engaging in distracted pedestrian behavior. The second steps analyzed the behavioral observation data to evaluate our second hypothesis of changes in community-level observed distracted pedestrian behavior. The third step also analyzed the behavioral observation data, and addressed a secondary question of whether the intervention created a change in safety among distracted pedestrians at the community level. We detail the three steps below.
First, descriptive analysis of data from the individual surveys at UAB was conducted. We used generalized estimating equations (GEEs) with a logit link with the appropriate contrasts to determine whether there was change in perceived vulnerability/susceptibility to pedestrian injury from pre-to post-intervention and from pre-intervention to follow-up assessment. Second, we considered whether the intervention changed community-based norms about walking across streets while distracted by comparing distracted pedestrian behavior in the intervention UAB community versus in the control ODU community using Poisson regression models with scaled deviance. We used logistic regression to determine whether there were differences between the campuses over time, primarily by examining the interaction between campus site and time. Last, we conducted a secondary analysis to test whether there was change in safe behaviors among distracted pedestrians. We examined the percentage of time distracted pedestrians engaged in three safe behaviors – walking with the walk sign, looking left before entering the near lanes of traffic, and looking right before entering the far lanes of traffic – at both campuses. We used logistic regression models to assess these differences.
3. Results
Table 1 presents descriptive data for the individuals who completed surveys at UAB. As shown, the individual survey data were completed by a sample typical of college campuses in terms of age (mean age = 22.6 years, SD = 7.2), weighted somewhat to females (63%), and racially/ethnically diverse (44% Caucasian, 33% African American, 9% Asian American). The sample had approximately equal numbers of freshman, sophomores and juniors, with slightly fewer seniors and a sprinkling of graduate students, staff members, and others.
Table 1.
Demographics: Survey Respondents (N=218)
| Age (mean, SD) in years (# missing: 8) | 22.6 (7.2) |
| Male (# missing: 4) | 79 (37%) |
| Ethnicity (# missing: 3) | |
| African American | 71 (33%) |
| Asian | 19 (9%) |
| Caucasian | 95 (44%) |
| Hispanic | 3 (1%) |
| Other | 28 (13%) |
| Classification (# missing: 3) | |
| Freshman | 54 (25%) |
| Sophomore | 56 (26%) |
| Junior | 49 (23%) |
| Senior | 34 (16%) |
| Graduate Student | 10 (5%) |
| Staff/Other | 13 (6%) |
Table 2 lists results from individual surveys concerning self-reported distracted pedestrian behavior. These results address our first aim, that the intervention would create an increase in perceived vulnerability to risks of distracted pedestrian behavior. Prior to conducting the analyses, we computed a priori comparisons of those who completed each of the three surveys to address concern about biased attrition. The following baseline characteristics were compared across completers, those who completed only the pre and post surveys, and those who completed only the pre survey: age, gender, race/ethnicity, classification (year in school), and self-reported baseline risk behavior for each of the four distracted pedestrian behaviors (talking, texting, using apps, listening to music). Just one statistically significant result emerged, for classification. Completers were less likely to be freshman in college, perhaps reflecting in part natural attrition from the university rather than from the study. As shown in Table 2, participants self-reported a decrease in talking, texting, and using apps while walking at follow-up compared to their behavior prior to the intervention. Results from Table 3 support this finding, as participants also reported that the intervention caused them to think more carefully about crossing streets while distracted, tended to cause a behavior change, and was a worthwhile experience that they would recommend to others.
Table 2.
Frequency and % for unsafe activities at each time point, odds ratio & 95% confidence intervals for likelihood of engaging in unsafe activity compared to never/rarely engaging in unsafe activity (bold face indicates a pairwise-significant difference)
| Pre (n=200) |
Post (n=150) |
Follow-up (n=91) |
Pre (n=200) |
Post (n=150) |
Follow-up (n=91) |
p-valuea | |
|---|---|---|---|---|---|---|---|
| Talk while walking: Never/Rarely | 104 (52%) |
74 (49%) |
61 (67%) |
REF | 1.15 (0.85, 1.58) |
0.60 (0.41, 0.88) |
0.0036 |
| Text while walking: Never/Rarely | 89 (45%) |
76 (51%) |
52 (57%) |
REF | 0.79 (0.58, 1.07) |
0.59 (0.39, 0.89) |
0.040 |
| Apps while walking: Never/Rarely | 100 (50%) |
85 (57%) |
58 (64%) |
REF | 0.78 (0.57, 1.06) |
0.48 (0.32, 0.73) |
0.0037 |
| Music while walking: Never/Rarely | 95 (48%) |
70 (46%) |
47 (52%) |
REF | 1.05 (0.81, 1.36) |
1.09 (0.76, 1.55) |
0.88 |
Note: n=151 for the talking while walking variables at post
Overall p-value, representing at least two time-points differ
Table 3.
Assessing the influence of the intervention
| Post (n=150) |
Follow-up (n=91) |
|
|---|---|---|
| Did participating in the virtual street environment make you think more carefully about crossing streets while distracted? | ||
| Yes | 125 (83%) | 79 (87%) |
| No | 17 (11%) | 5 (5%) |
| Not sure | 8 (5%) | 7 (8%) |
| Since participating in the virtual environment, have you changed your behavior while crossing streets? | ||
| Yes | 91 (61%) | 60 (65%) |
| No | 37 (25%) | 22 (24%) |
| Not sure | 22 (15%) | 11 (12%) |
| Do you think participating in the virtual environment was a worthwhile experience to improve your health and safety? | ||
| Yes | 126 (84%) | 76 (82%) |
| No | 10 (7%) | 3 (3%) |
| Not sure | 14 (9%) | 14 (15%) |
| Would you recommend other people try crossing the virtual environment while distracted to see how it influences their safety? | ||
| Yes | 143 (95%) | 89 (96%) |
| No | 5 (3%) | 1 (1%) |
| Not sure | 2 (1%) | 3 (3%) |
The next step of data analysis was to consider observed pedestrian behavior, which addressed our second study aim, to alter community norms about distracted pedestrian behavior at UAB in comparison to ODU. Table 4 presents descriptive data about the campus environments. The universities had relatively comparable student body sizes and compositions, daily temperatures, and traffic and pedestrian patterns, although ODU experienced somewhat higher traffic and pedestrian volume than UAB.
Table 4.
Demographics: Campus Environments
| Variable | UAB | ODU |
|---|---|---|
| Number of students | 18,333 | 24,672 |
| Student body: % non-white | 38 | 52 |
| Average daily temperature, degrees | 63 | 60 |
| Baseline traffic volume at study site, vehicles/hour mean (SD); median (range) | 856(204) 864 (168–1560) |
964 (232) 972 (1081500) |
| Baseline pedestrian count at study site, pedestrians/hour mean (SD); median (range) | 69 (76) 44 (0–400) |
146 (111) 120 (0–580) |
Note: UAB = University of Alabama at Birmingham; ODU = Old Dominion University; SD = Standard Deviation
In examining distracted pedestrian behavior on both campuses, we considered both general distraction and also texting behavior, as our intervention focused especially on reducing texting while crossing streets. We focused on the “all pedestrians” coding sessions of 15-minute blocks. Over time following the intervention, the overall rate of distraction at UAB was largely unchanged from 27/100 pedestrians distracted at pre-intervention to 28/100 pedestrians at post-intervention, 25/100 pedestrians at 10 weeks, and 24/100 at the 6-month observation period. The rate at ODU was also fairly stable: it began at 36/100 pedestrians at pre-intervention and was 40/100 pedestrians at post-intervention, 39/100 pedestrians at 10 weeks, and 38/100 pedestrians 6 months later. The differences across sites were statistically significant (all ps<.05), as were effects over time within campuses (ps < .01) and the interaction between site and time (p=0.013). However, no behaviorally meaningful trends were detected by these statistically significant results. Figure 3 shows similar values for the rate of pedestrian behavior while texting on both campuses. As shown, the pattern at UAB decreased slightly over time (9.4/100, 9.1/100, 8.3/100, 9.0/100) but the change was not statistically significant. Rates at ODU remained fairly stable over time (7.0/100, 9.6/100, 7.5/100, 8.8/100). Again, the differences between sites were statistically significant, as was the interaction between site and time (p=0.0025), but no behaviorally meaningful trends were detected.
Figure 3.
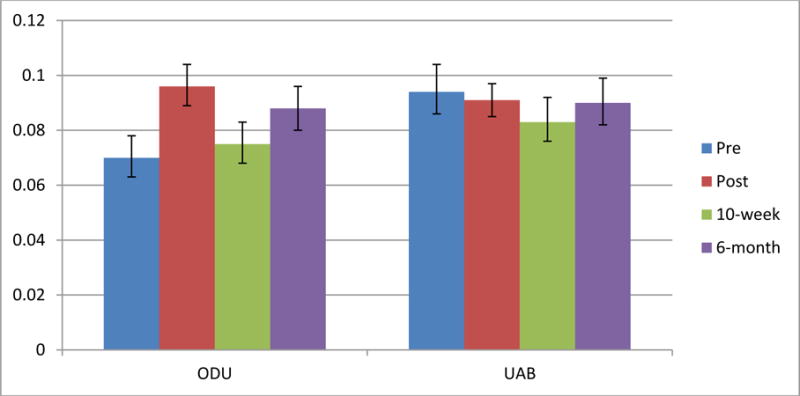
Observed Texting while Walking, All Pedestrians
To ensure these findings were valid, we also examined the patterns among the data collected during the 5-minute blocks of individual pedestrians. Results were very similar, so we conducted a secondary analysis to examine whether there may have been improved safety among distracted pedestrians at UAB compared to ODU after the intervention even though the rate of distraction did not decrease significantly. To do this, using data from the individualized pedestrian observations (5 minute blocks), we considered three measures of safe pedestrian behavior: walking when the walk signal was displayed, looking left before entering the near lanes of traffic, and looking right before entering the far lanes of traffic after crossing the median. As shown in Table 5, there was no evidence that safe behaviors changed among distracted pedestrians at UAB compared to ODU.
Table 5.
Percentage of safe behaviors among pedestrians observed to be texting and followed individually, across time points and universities
| Variable | Pre | Post | 10-week | 6-month | p1 |
|---|---|---|---|---|---|
| Walk with walk sign | |||||
| ODU | 56 | 35 | 40 | 49 | .16 |
| UAB | 91 | 88 | 88 | 89 | .99 |
| Look left when entering | |||||
| ODU | 63 | 64 | 63 | 56 | .85 |
| UAB | 28 | 21 | 21 | 35 | .41 |
| Look right leaving median | |||||
| ODU | 63 | 57 | 60 | 40 | .11 |
| UAB | 32 | 18 | 36 | 28 | .23 |
p-value over time within university. All p-values across universities significant at p<.05 level except 6-month look right at median. All p-values for site × time interaction effects nonsignificant (p>.10)
4. Discussion
This study represents an initial attempt to use behavioral strategies to reduce distracted pedestrian behavior in the high-risk environment of an urban college campus. We used a multifaceted intervention approach hallmarked by the opportunity for pedestrians to experience the risk of distracted pedestrian behavior by trying to text while crossing a virtual street and supplemented by traditional and social media efforts across the campus community. Results from the effort were mixed. We were successful in eliciting change in self-reported intentions to cross streets while distracted and in perceived vulnerability to risk while crossing streets distracted among individuals exposed to the intervention, but we were unsuccessful in changing community-based norms based on observed rates of distracted pedestrian behavior, including texting, before and after the intervention compared to a control campus not exposed to the intervention.
Health behavior interventionists recognize the challenge of changing behaviors, and the addictive lure of smartphones and technology presents a particularly challenging obstacle to health-related behavior change. The fact that we succeeded in changing self-reports of perceived vulnerability is encouraging. Citing the Transtheoretical model (Prochaska & Velicer, 1997), we apparently moved many individuals to the stages of preparation and action, thus yielding some individual-level change toward safety. This result offers promise for the development of future interventions, as it demonstrates the fact that the most active aspect of our intervention, asking people to try texting within the safe environment of a simulated roadway, created change in cognitive perceptions and intended behaviors. Efforts to extend this finding through other novel, experiential situations like virtual reality could be fruitful to reduce distracted pedestrian and other risky or negative health behaviors.
Contrary to our hypothesis, we did not create significant behavioral change at the community level. There are at least a few possible explanations for this failure. First, we may have only achieved change among those individuals who were exposed to trying to text within the simulated pedestrian environment. About 1,000 individuals were exposed to that experience over the course of our week-long intervention, but the campus includes close to 20,000 students and thousands more staff, faculty, and community members who cross the streets regularly near campus. Thus, our reach for the most active part of the intervention – personal experience trying to text while crossing a simulated street – was comparatively small. Many of the individuals we observed crossing the street to assess community-level change were not exposed to the simulated street crossing while texting and we did not assess directly the behavior of those exposed to the simulation. Our secondary intervention strategies that were delivered via social and traditional media were designed to supplement rather than create change, and would not be likely to create significant behavior change based on previous intervention research.
A second possible explanation for our failure to create community-wide change is that we may not have accomplished the social contagion or diffusion (Burt, 1987; Rogers, 1995) effect we sought, whereby ideas, behaviors and practices would spread through the campus community via social networking. Much as an urban campus environment is a close-knit community with an elaborate web of interpersonal relationships, and anecdotal evidence suggested people around campus were commenting about and discussing the “Pocket and Walk It” campaign while it occurred, a transition from awareness and discussion to action and cultural shift is a significant one that requires substantial community involvement, time and effort. When successful, such community-wide shifts are frequently supported by policy or other external influences (Doll, Bonzo, Mercy, & Sleet, 2007).
Our study had strengths and weaknesses. Strengths included use of a control campus site, observational measures to collect behavioral outcomes, and an innovative, theory-based intervention strategy. Weaknesses included the limitation to just one intervention community and two communities of study, focus on a single intersection at each campus, and some attrition from the sample providing self-report data on perceived vulnerability. To overcome these limitations and extend our knowledge about behavioral strategies to reduce distracted pedestrian behavior, further research is recommended. Distracted pedestrian behavior is and will continue to be a significant public health challenge. Interventions that target both individual-and community-level change are needed. Our intervention offers an excellent starting point for scholars to consider innovative and effective means to increase safety by reducing distracted pedestrian behavior on roadways.
Highlights.
Distracted pedestrian behavior is a significant public health challenge.
Few programs addressing distracted pedestrians have been evaluated rigorously.
We evaluated a behavioral intervention to reduce distracted pedestrian behavior.
Individuals texted within a virtual pedestrian environment
We increased perceived vulnerability to risk but observed no behavior change.
Acknowledgments
Thanks to the Anna Johnston, the UAB Youth Safety Lab, and the team at Old Dominion University for assistance with data collection and entry. Thanks to Joan Severson and Digital Artefacts for support of the virtual pedestrian environments. Thanks to our many partners at UAB to promote ‘Pocket and Walk It’ week. Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health & Human Development of the National Institutes of Health under Award Number R21HD078371. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Barton BK. Integrating selective attention into developmental pedestrian safety research. Canadian Psychology. 2006;47:203–210. [Google Scholar]
- Burt RS. Social contagion and innovation: Cohesion versus structural equivalence. American Journal of Sociology. 1987;92:1287–1335. [Google Scholar]
- Centers for Disease Control and Prevention [CDC] Injury Prevention & Control: Data & Statistics (WISQARS) 2016 Accessed 9/13/16 from: http://www.cdc.gov/iniury/wisqars/
- Doll LS, Bonzo SE, Sleet DA, Mercy JA, editors. Handbook of Injury and Violence Prevention. New York: Springer; 2007. [Google Scholar]
- Fischer P. Everyone walks. Understanding and addressing pedestrian safety. 2015 Accessed 9/16/16 from: http://www.ghsa.org/html/publications/sfped.html.
- Kahneman D. Attention and effort. Englewood Cliffs, NJ: Prentice-Hall; 1973. [Google Scholar]
- Mwakalonge J, Siuhi S, White J. Distracted walking: Examining the extent to pedestrian safety problems. Journal of Traffic and Transportation Engineering. 2015;2:327–337. [Google Scholar]
- National Safety Council. Injury Facts, 2015 Edition. Itasca, IL: Author; 2015. [Google Scholar]
- Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. American Journal of Health Promotion. 1997;12:38–48. doi: 10.4278/0890-1171-12.1.38. [DOI] [PubMed] [Google Scholar]
- Rogers EM. Diffusion of Innovations. 4th. New York: Free Press; 1996. [Google Scholar]
- Rosenstock IM. The health belief model and preventive health behavior. Health Education Monographs. 1974;2:354–386. doi: 10.1177/109019817800600406. [DOI] [PubMed] [Google Scholar]
- Schwebel DC, Combs T, Rodriguez D, Severson J, Sisiopiku V. Community-based pedestrian safety training in virtual reality: A pragmatic trial. Accident Analysis and Prevention. 2016;86:9–15. doi: 10.1016/j.aap.2015.10.002. [DOI] [PubMed] [Google Scholar]
- Schwebel DC, McClure LA, Severson J. Teaching children to cross streets safely: A randomized controlled trial. Health Psychology. 2014;33:628–638. doi: 10.1037/hea0000032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stavrinos D, Pope CN, Shen J, Schwebel DC. Systematic review of mobile technology and pediatric injury risk: Cognitive and developmental considerations. Child Development (in press) [Google Scholar]
- Thomson JA. Promoting pedestrian skill development in young children: Implementation of a national community-centered behavioral training scheme. In: Durkin K, Schaffer HR, editors. The Wiley Handbook of Developmental Psychology in Practice: Implementation and Impact. 1st. Hoboken, NJ: Wiley; 2016. pp. 311–340. [Google Scholar]
- Weinstein ND. Reducing unrealistic optimism about illness susceptibility. Health Psychology. 1983;2:11–20. [Google Scholar]
- Weinstein ND. Why it won’t happen to me: Perceptions of risk factors and susceptibility. Health Psychology. 1984;3:431–457. doi: 10.1037//0278-6133.3.5.431. [DOI] [PubMed] [Google Scholar]