

Abstract
Congenital hernia of the cord is a different type of ventral abdominal wall defect in which the bowel usually herniates into the base of normally inserted umbilical cord through a patent umbilical ring. It is rare congenital anomaly with incidence of 1 in 5000. Although it was described as a distinct entity since 1920s it is often misdiagnosed as a small omphalocele. We present an unusal case of term male newborn with umbilical cord hernia associated with patent omphalomesenteric duct. The diagnose was made after birth despite antenatal ultrasound scans and it is managed successfully with uneventful recovery. If this is missdiagnosed, it could cause iatrogenic atresia of the ileum by clamping the umbilical cord after birth.
KEY WORDS: Associated pathology, patent omphalomesenteric duct, umbilical cord hernia
Introduction
Congenital hernia of the umbilical cord is a different type of ventral abdominal wall defect, in which the bowel usually herniates into the base of normally inserted umbilical cord through a patent umbilical ring. Its incidence is estimated to be 1 in 5000, and unlike omphalocele, it is not linked with chromosomal anomalies, and association with other anomalies is rare although there is a loose association with intestinal anomalies, malrotation, and volvulus.[1] Cases of umbilical cord hernia associated with extracelomic colonic atresia, short gut, and patent omphalomesenteric duct (OMD) were reported.
Clinical Image
We present a clinical image of congenital umbilical cord hernia associated with patent OMD. A term male newborn, weighing 2480 g, was born by spontaneous vaginal delivery at the 37th gestation week. The prenatal events were normal, and anomaly was not diagnosed during the pregnancy although antenatal ultrasound scans were performed. At first, the patient was thought to have small omphalocele; however, careful examination revealed hernia of umbilical cord with prolapsing bowel evisceration through the umbilical cord. Further examinations showed that there were no other associated anomalies, and genetic screening was normal. The patient was given initial resuscitation in terms of covering the bowel with warm saline soaked gauzes, infusing intravenous fluids, and prophylactic antibiotics. The patient was vitally stable, and surgery was performed on the next day. At operation, patent OMD was confirmed as extruded mucosa, with openings on both sides where meconium has been passed. First umbilical arteries, vein, and urachus were ligated; afterward, amniotic membrane was dissected, and reduction of eviscerated mucosa was done [Figure 1a–c]. Resection of widely patent OMD was performed with end-to-end ileoileal anastomosis. The contents were reduced to the abdomen, and umbilical ring was closed. There were no intraoperative complications, and postoperative recovery was uneventful. He started on feeding after 72 h. The patient was discharged home on the 17th postoperative day in a good clinical condition.
Figure 1.
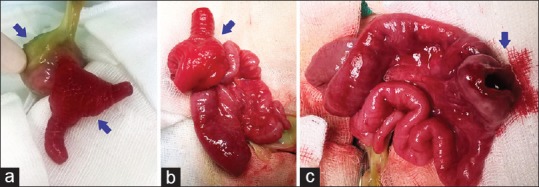
(a) Hernia of the umbilical cord associated with patent omphalomesenteric duct. (b) Intraoperative findings after removing of amniotic sac, small intestines, and omphalomesenteric duct. (c) Presentation of omphalomesenteric duct after reduction of eviscerated mucosa
Discussion
Congenital hernia of the umbilical cord is a herniation of small bowel and occasionally other viscera into umbilical cord while the rest of the anterior abdominal wall is usually normal.[2] During the 3rd week of intrauterine life, there is a communication between the intraembryonic gut and the yolk sac as the development proceeds this communication narrows into a tube known as the OMD, and it usually obliterates by the end of the 7th week. There is physiological herniation of the midgut into the umbilical coelom during 5–6th week of gestation and herniated gut then returns during 10–12th week of gestation into the abdominal cavity. It is the time when a small part of midgut could not return completely into the abdomen and thus retained in the base of umbilicus resulting in hernia of umbilical cord.[2] Last decades, antenatal diagnosis of hernia of umbilical cord was reported on prenatal ultrasound and magnetic resonance imaging findings.[1,3] For correct clinical diagnostics, it is mandatory to look carefully for the presence of any true abdominal wall defect, umbilical ring, and the basis for the presence of skin collar fold so that the condition could not be misdiagnosed.[4] Any unusual thickening of the base of the cord along with even the most minute fistula opening to its side should alert the physician to the existence of these combined anomalies. If this is misdiagnosed, clamping of the umbilical cord after birth can cause iatrogenic atresia of the ileum.[5]
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Achiron R, Soriano D, Lipitz S, Mashiach S, Goldman B, Seidman DS. Fetal midgut herniation into the umbilical cord: Improved definition of ventral abdominal anomaly with the use of transvaginal sonography. Ultrasound Obstet Gynecol. 1995;6:256–60. doi: 10.1046/j.1469-0705.1995.06040256.x. [DOI] [PubMed] [Google Scholar]
- 2.Mirza B, Saleem M. Hernia of umbilical cord with congenital short gut. J Neonatal Surg. 2014;3:26. [PMC free article] [PubMed] [Google Scholar]
- 3.Ono K, Kikuchi A, Takikawa KM, Hiroma T, Yoshizawa K, Sunagawa S, et al. Hernia of the umbilical cord and associated ileal prolapse through a patent omphalomesenteric duct: Prenatal ultrasound and MRI findings. Fetal Diagn Ther. 2009;25:72–5. doi: 10.1159/000200633. [DOI] [PubMed] [Google Scholar]
- 4.Waqas Ali S, Arain A. Large hernia of umbilical cord misdiagnosed as omphalocele. J Neonatal Surg. 2015;4:36. [PMC free article] [PubMed] [Google Scholar]
- 5.Jona JZ. Congenital hernia of the cord and associated patent omphalomesenteric duct: A frequent neonatal problem? Am J Perinatol. 1996;13:223–6. doi: 10.1055/s-2007-994368. [DOI] [PubMed] [Google Scholar]