

Abstract
Low-grade inflammation is associated with an increased risk of chronic degenerative disease, but its relationship with mortality is less well explored. We aimed at evaluating, at a large epidemiological level, the possible association of low-grade inflammation, as measured by a composite score, with overall mortality risk. We conducted a population-based prospective investigation on 20,337 adult subjects free from major hematological disease and acute inflammatory status, randomly recruited from the general population of the Moli-sani study. A low-grade inflammation score was obtained from the sum of 10-tiles of plasmatic (C-reactive protein) and cellular (leukocyte and platelet counts, granulocyte/lymphocyte ratio) biomarkers of low-grade inflammation; higher levels indicated increased low-grade inflammation. Hazard ratios were calculated using multivariable Cox proportional hazard models with 95% confidence intervals. At the end of follow-up (median 7.6 years), 837 all-cause deaths were recorded. As compared to subjects in the lowest quartile of the low-grade inflammation score, those in the highest category had a significantly increased risk in overall mortality (HR=1.44; 1.17–1.77), independently of possible confounders, including the presence of chronic diseases and a number of health-related behaviors. The magnitude of the association of low-grade inflammation with mortality was relatively higher in type 2 diabetic patients (HR=2.90; 1.74–4.84) and in individuals with a history of cardiovascular disease (HR=2.48; 1.50–4.11) as compared to their counterparts who were free from the disease. In conclusion, an elevated degree of low-grade inflammation, as measured by a composite score of inflammatory biomarkers, is an independent risk factor for total mortality in an apparently healthy adult general population.
Introduction
Low-grade inflammation is a condition not yet consistently defined or measured. A number of plasmatic (e.g. C-reactive protein) or cellular biomarkers (e.g. white blood cell and platelet counts) have been proposed as reliable indicators of such a condition.1,2
This subclinical disorder has been recognized as a risk factor for a number of chronic diseases including cancer, cardiovascular (CVD) and neurodegenerative disease.3–6 In contrast, its relationship with mortality has been poorly investigated, at least in the general population,7,8 while evidence within high-risk groups is more robust.9–11
Low-grade inflammation has also been proposed as an underlying pathophysiological mechanism linking risk factors or metabolic disorders (e.g. oxidative stress, obesity, diabetes, dyslipidemia), to an increased risk of chronic degenerative disease1 as well as a common pathogenic denominator in age-related diseases.12
Pioneering large-scale studies focused on circulating fibrinogen, C-reactive protein (CRP), and white blood cell (WBC) counts as reliable inflammatory biomarkers, mostly in relation to cardiovascular events.6,13–16 More recently, a pro-inflammatory action of blood platelets has been proposed,17 whereas the neutrophil-to-lymphocyte ratio better expresses an early inflammatory cellular response.18,19 Evidence of the individual contribution of each of the above mentioned inflammatory biomarkers to different health outcomes is scarce.7,14,17 Previous data suggest that some inflammation biomarkers are associated with lifestyle modifications (e.g. dietary habits17) or electrocardiographic parameters,19 emphasizing the need for further study on their association with clinical outcomes, such as the incidence of chronic degenerative disease and mortality rates. In this context, a comprehensive approach to measure a low-grade inflammation condition has been proposed in high cardiovascular risk subjects.20,21 Lately, a significant inverse association of a composite low-grade inflammation score with dietary polyphenol intake has been observed by our group in a population-based cohort.22
The purpose of the present study was to evaluate whether this composite low-grade inflammation score would be associated with overall mortality in an adult population cohort with no overt acute inflammation or major hematological diseases. In addition, we also dissected the specific contribution of each component of the score and performed sensitivity analysis, to test whether the association with mortality varied across subgroups at different health risks.
Methods
Study population
This study analyzed data from the population-based cohort of 24,325 men and women aged ≥35 years enrolled in the Moli-sani study from March 2005 to April 2010.23
We excluded from the analysis individuals lost to follow-up (1.3%), those reporting unreliable anamnestic questionnaires at baseline (1%), or having hepatitis B or C (2.9%) or any hematological disease (2.2%), or having missing data on platelet count (2.7%), WBC (2.7%), high-sensitivity (hs) CRP (0.12%), granulocytes or lymphocytes (3.2%). Subjects with CRP≥ 10 mg/l (4%) were also excluded to avoid confounding due to an acute inflammatory condition; we also eliminated those included in the percentiles of either highest (1%) or lowest (99%) values for platelet (1.9%) or WBC counts (1.9%). The final sample was of 20,337 (48.2% men) participants.
The Moli-sani study was approved by the Ethics Committee of the Catholic University of Rome, Italy. See the Online Supplementary Methods for further information.
INFLA-score
The low-grade inflammation (INFLA) score had been used previously within the Moli-sani cohort22 and allows one to evaluate the possible synergistic effects of inflammation biomarkers. 10-tiles of each biomarker levels (CRP, WBC, platelets, G/L ratio) were generated. For all four components, being in the highest deciles (7 to 10) gave a score which increased from 1 to 4, while being in the lowest deciles (1 to 4) was negatively scored from −4 to −1. Being in the deciles 5 or 6 got zero points. In such a way, the INFLA-score ranged from between −16 and 16 and came up as the sum of the four biomarkers. An increase in the score represented an increase in low-grade inflammation intensity. For analysis purposes, quartiles of the INFLA-score were also generated.
Statistical analysis
Age and sex adjusted multivariable analysis of variance for continuous or categorical variables was applied to test the associations in Table 1. Potential covariates were included in the multivariable model when they resulted as associated with P<0.20 with both the INFLA-score and mortality.
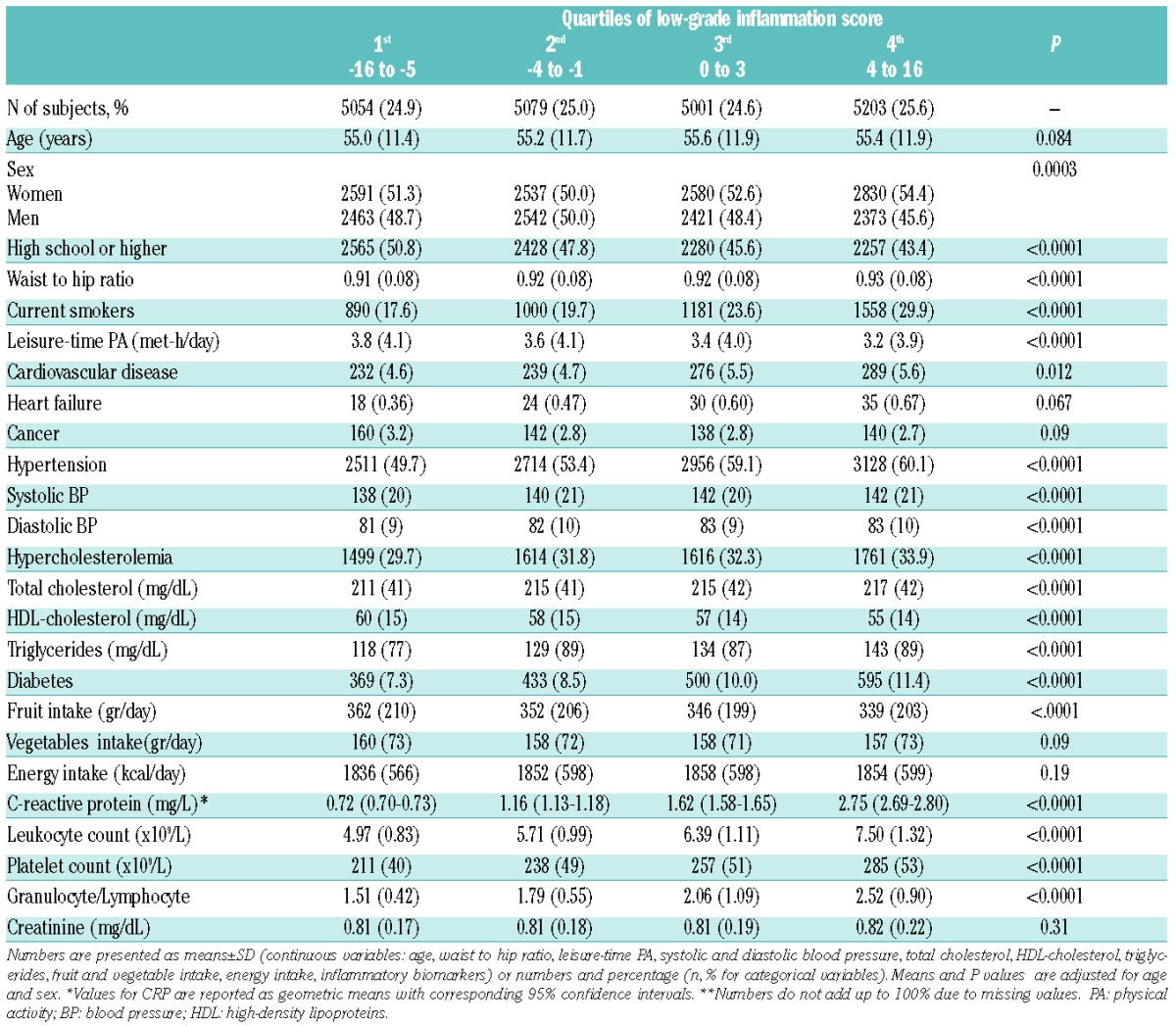
Table 1.
Baseline characteristics of the study population according to low-grade inflammation.
Age and sex adjusted and multivariable hazard ratios with corresponding 95% confidence intervals (95%CI) were calculated using the Cox proportional hazards model, considering subjects in the lowest quartile of the INFLA-score as the reference group. To highlight the specific role of each component within the INFLA-score in relation to mortality, hazard ratios were calculated by removing one component at a time from the original score. The models with and without individual components of the score were compared using Akaike’s information criterion (AIC).24 Harrell’s C-index was used to quantify the prediction capacity of the model.
Sensitivity analyses were undertaken to estimate possible differences in the magnitude of the association between low-grade inflammation and mortality within subgroups at different health risks. Appropriate interaction terms were added to the Cox regression models to test for a difference of the effect of low-grade inflammation across subgroups. For subgroup analyses, all variables were dichotomised (no/yes), and missing categories excluded.
Tests for a violation of the proportional hazards assumption were conducted through the introduction of linear interaction between categories of the INFLA-score and the time variable (P=0.66). A two-sided P-value of <0.05 was considered as statistically significant.
Results
Baseline characteristics of the Moli-sani cohort according to quartiles of the INFLA-score are reported in Table 1. Compared to subjects in the lowest category, those with an increasing INFLA-score were mainly women, had a lower level of education, a higher prevalence of unhealthy lifestyles (smoking, poor leisure-time PA, higher WH-ratio, lower intake of fruit), and an increased prevalence of CVD, diabetes, hypercholesterolemia and hypertension (P<0.05).
During a median follow-up of 7.6 years (interquartile range: 6.7 to 8.6 years; 153,897 person/years), 837 deaths occurred overall. Subjects in the higher quartiles of low-grade inflammation score had a 44% (23% to 83%) increased risk of all-cause mortality in the multivariable analyses, in comparison with subjects in the lowest quartile (Table 2, Figure 1). Harrell’s C-index for the model was equal to 0.86 (95%CI 0.84–0.86).
Table 2.
Risk of all-cause mortality associated with quartiles of low-grade inflammation and after alternate subtraction of each component.
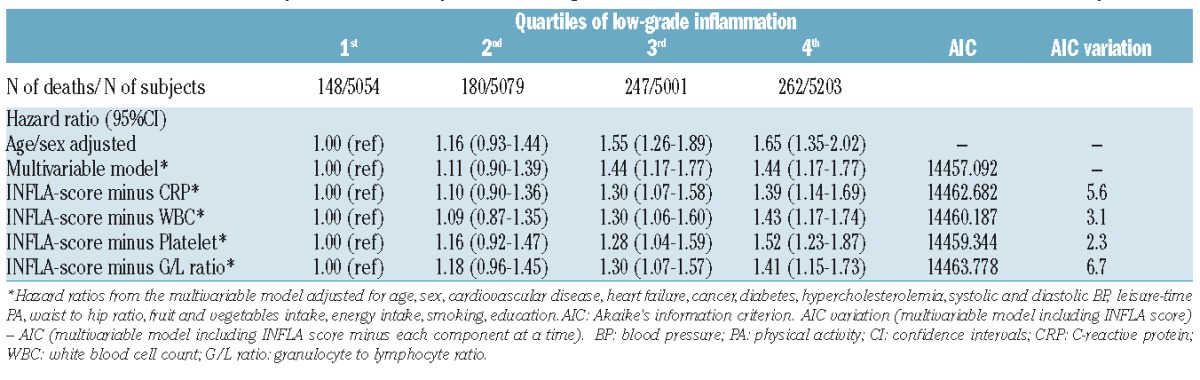
Figure 1.
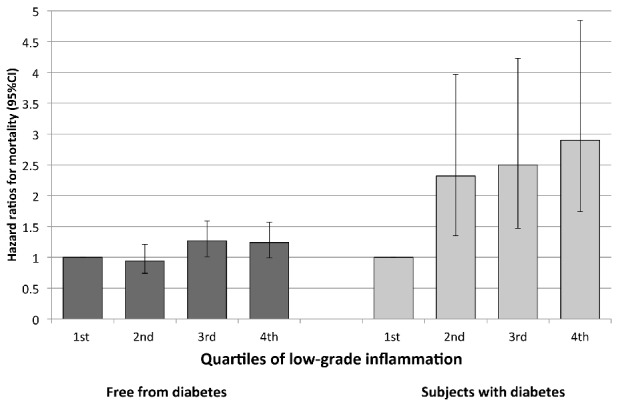
Relative risk of all-cause death for each quartile of low-grade inflammation score according to the presence of diabetes at baseline. The reference group is the lowest quartile for each subgroup. Hazard ratios are adjusted for age, sex, cardiovascular disease, heart failure, cancer, hypercholesterolemia, systolic and diastolic BP, leisure-time PA, waist to hip ratio, fruit and vegetables intake, energy intake, smoking, education. Vertical bars indicate 95% confidence intervals. PA: physical activity; BP: blood pressure.
The INFLA-score was alternately deprived of its components in order to assess the relative contribution of each biomarker. Models deprived of one component at a time have an AIC which is lower than models which have a score that includes all of the components (Table 2). These differences are strong enough to support the hypothesis that the model including the full score is the best, and that each component adds some value to the full score. In particular, CRP and G/L ratio contributed most, since their exclusion from the score resulted in a more pronounced AIC decrease (Table 2).
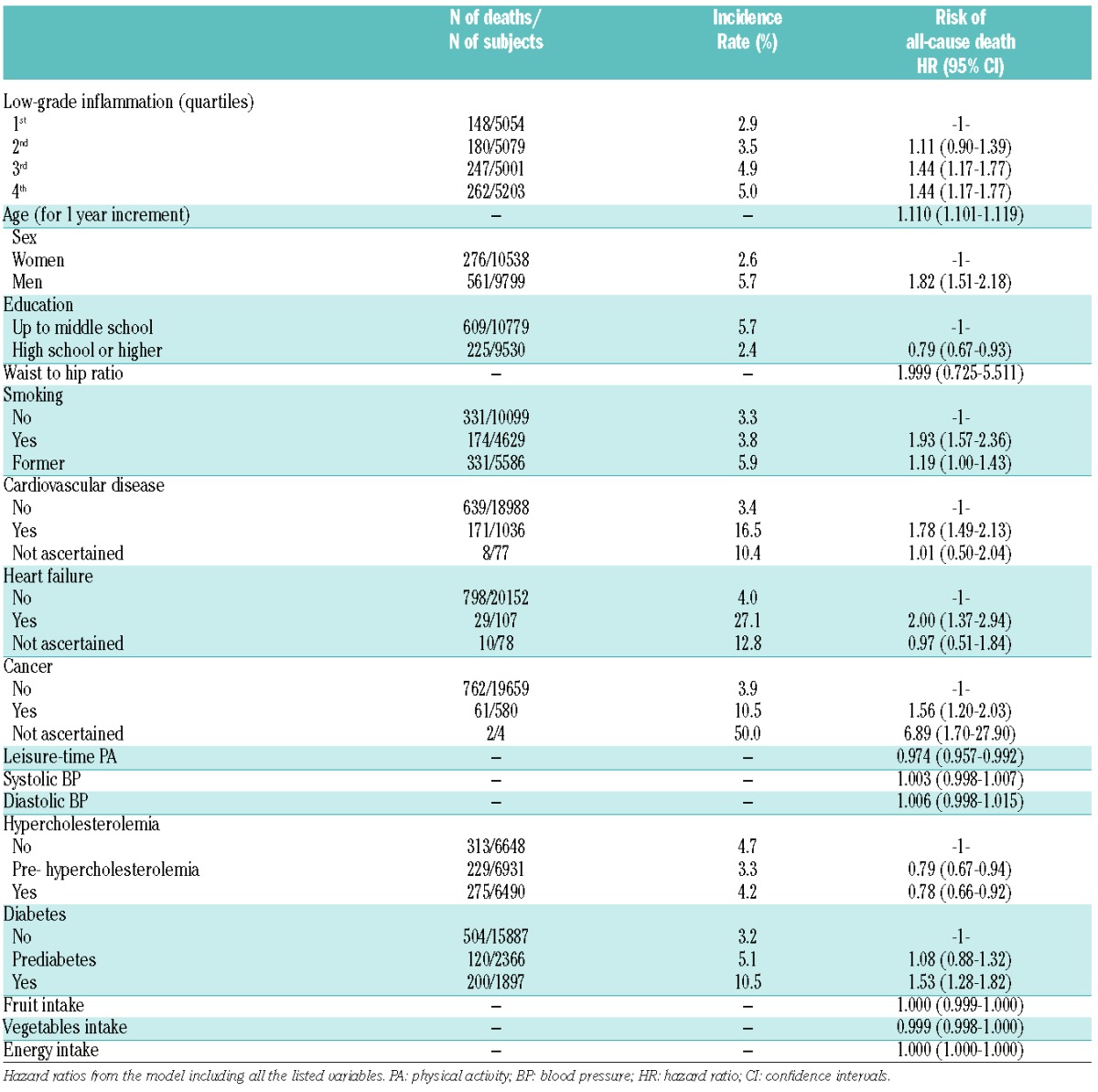
Table 3 shows potential predictors of all-cause death in the study population. Major risk factors positively associated with death were age, sex (men), a low level of education, waist to hip ratio, smoking habit, poor leisure-time physical activity, and major chronic diseases at baseline, with the exception of hypercholesterolemia. It is noteworthy that the relative risk associated with the highest category of the INFLA-score is comparable to that of cancer-or diabetes-related risk.
Table 3.
Risk factors associated with all-cause mortality in the study population.
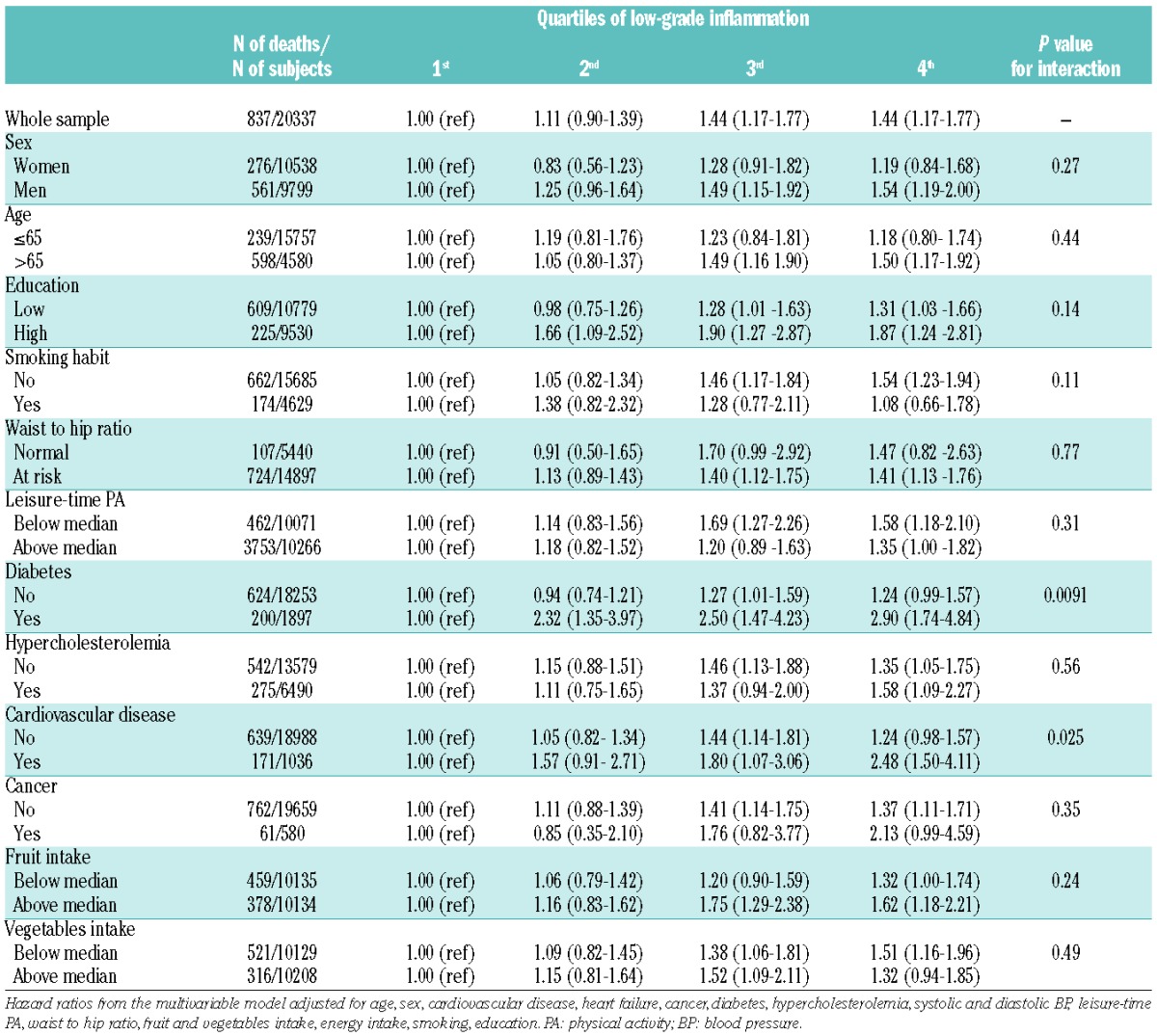
Sensitivity analysis is reported in Table 4. A higher risk linked to an increased INFLA-score was found for subjects with diabetes or CVD as compared to their counterparts (P for interaction = 0.0091 and 0.025, respectively, Figure 1), suggesting a significant interaction between a subclinical chronic inflammation and the presence of major diseases at baseline in relation to the risk of death. As far as all other subgroups are concerned, the strength of the association of the INFLA-score with mortality did not significantly differ (P>0.05) (Table 4).
Table 4.
Sensitivity analyses for the association of low-grade inflammation and all-cause mortality.
Discussion
Non-communicable diseases (such as cardiovascular, cancer and neurodegenerative disease) account for 80% of deaths in Europe,25 and each of these conditions is associated with a pro-inflammatory state.26 The concomitant presence of inflammatory biomarkers in diseases with apparently different pathogenesis supports the hypothesis of a common inflammatory soil underlying the pathogenetic mechanisms involved.27,28 Yet, the low-grade inflammation status has not been clearly and uniformly defined, and its association with mortality has principally been explored using a single biomarker approach8,29 rather than considering a panel of combined selected biomarkers.2,7
In the present study, increased low-grade inflammation as measured by a score including plasmatic and cellular biomarkers, was found to be associated with a 44% increased risk of all-cause mortality in a large population cohort, in the absence of an acute inflammation status or major hematological diseases. The INFLA-score tested in our population included four markers of inflammation that have been previously reported in association with an increased risk of adverse health outcomes.
To the best of our knowledge, this study is the first to have explored the risk of total mortality in a general population in association with a clinically silent low-grade inflammation condition measured by a composite score.
In the conceptual framework of our analyses, low-grade inflammation was conceived as a subclinical condition (systemic or local, often chronic), characterized by increased levels of plasmatic and/or cellular biomarkers of inflammation without any apparent clinical sign. Of note, the population under study was selected to exclude from the analyses all subjects with acute inflammation or any kind of hematological diseases that may lead to an overestimation of the risk; therefore our findings have to be interpreted as related to variations within the ranges of normality for each biomarker of inflammation.
This approach has been previously proposed and tested within the Moli-sani cohort in relation to dietary polyphenol intake.22 As remarked previously, the advantages of using a composite assessment of low-grade inflammation is to summarize the variability of inflammation as a plasmatic and cellular phenomenon at an epidemiological scale. In addition, the use of a score allowed for the evaluation of a possible synergistic effect of inflammation biomarkers that are usually autocorrelated, and may thus produce multi-collinearity when simultaneously studied in a regression model.
We also addressed the question of the specific contribution of each biomarker, in order to exclude a training role of one biomarker over others: both CRP and G/L ratio contributed most to the association of the INLFLA-score with mortality. Nonetheless, the contribution of both leukocyte and platelet counts were not negligible, thus justifying their inclusion in the score. The excess of risks associated with the top quartile of the INFLA-score was comparable to that of common risk factors, thus reinforcing the need to take into account a low-grade inflammation condition when dealing with health outcomes.
The nature of the association between inflammatory markers and health outcomes is still a matter of debate.29 Regarding CVD onset, some studies support the hypothesis that the inflammatory markers, or the underlying inflammatory processes they represent, are directly involved in the development of atherosclerosis and plaque rupture,30,31 and more recently, two large-scale trials have been testing whether targeted inhibition of inflammation may reduce cardiovascular event rates by the use of targeted anti-inflammatory agents for the secondary prevention of myocardial infarction.32
On the other hand, others claim that rather than being independent risk factors, inflammation biomarkers confound the ultimate association with adverse CVD outcomes, due to the strict association of inflammatory markers with many cardiovascular risk factors, such as smoking or hypertension.33 However, our findings were controlled for a wide panel of possible confounders, including dietary factors and health-related behaviors, that should support the independence of low-grade inflammation in predicting overall mortality.
Sensitivity analyses revealed that the magnitude of the association of low-grade inflammation with mortality was higher in high-risk subjects, such as those with type 2 diabetes or a history of cardiovascular disease. To the best of our knowledge, few studies have investigated the likely heterogeneous effect of low-grade inflammation across groups at different health risks. Sanchez et al.34 found that inflammation appears more evident in diabetic than in non-diabetic patients with acute coronary syndrome, and that inflammatory markers constitute independent predictors of cardiovascular death in diabetics with unstable coronary disease. Results from the Hoorn study suggest that endothelial dysfunction and low-grade inflammation were associated with greater risks of cardiovascular mortality, especially in those with diabetes.35
Increased levels of inflammatory markers have been reported in patients with CVD, and it has been shown that the risk of death associated with high levels of IL-6 is dependent on the patients history of CVD, whereas for those without CVD the risk completely disappeared after adjustment for potential confounders.36
The strong relationship of low-grade inflammation with mortality in high-risk individuals is attributable to a procoagulant effect associated with inflammation.36 In addition, pro-inflammatory cytokines may be involved in promoting atherosclerotic plaque development and its disruption, an occurrence that is particularly plausible in CVD or diabetic patients.36–38
Strengths and limitations of this study
The major strengths of this study include a large community-based cohort, a prospective design and a quite long follow-up period. In addition, further controls of all analyses by a wide panel of possible confounding factors, including health-related behaviors, should assure consistency with the observed associations.
A major limitation of the present study is the lack of information on specific causes of death that prevents us from exploring the association of low-grade inflammation with different health outcomes. Since information about the participants were collected at baseline only, life course changes which possibly occurred during the follow-up may influence the strength of the findings. We acknowledge the lack of other biomarkers of inflammation, for example fibrinogen or interleukin-6,14,16 that were not included in the INFLA-score because of the unavailability of the data.
Conclusions
A high degree of low-grade inflammation, as measured by a composite score accounting for possible synergistic effects of selected inflammation biomarkers, is an independent risk factor for total mortality in a general population with no acute inflammation at baseline. Despite being associated with all major health risk conditions, a low-grade inflammation retains a significant independent health predictive value per se. The strength of the observed association was higher in diabetic patients and in individuals with a history of CVD.
Supplementary Material
Acknowledgments
The Moli-sani research group thanks the Associazione Cuore Sano Onlus (Campobasso, Italy) for its financial support and the Azienda Sanitaria Regionale del Molise (ASReM, Campobasso, Italy), the Offices of vital statistics of the Molise region and the Molise Dati Spa (Campobasso, Italy) for their collaboration and support provided during the follow-up activities.
Appendix 1. Moli-sani Study Investigators
The enrolment phase of the Moli-sani study was conducted at the Research Laboratories of the Catholic University in Campobasso (Italy), the follow up of the Mol-sani cohort is being conducted at the IRCCS Neuromed, Pozzilli, Italy. Steering Committee: Licia Iacoviello (Neuromed, Pozzilli, Italy), Chairperson, Maria Benedetta Donati and Giovanni de Gaetano (Neuromed, Pozzilli, Italy). Safety and data monitoring Committee: Jos Vermylen (Catholic University, Leuven, Belgium), Chairman, Ignacio De Paula Carrasco (Accademia Pontificia Pro Vita, Roma, Italy), Simona Giampaoli (Istituto Superiore di Sanità, Roma, Italy), Antonio Spagnuolo (Catholic University, Roma, Italy). Event adjudication Committee: Deodato Assanelli (Brescia, Italy), Vincenzo Centritto (Campobasso, Italy), Pasquale Spagnuolo and Dante Staniscia (Termoli, Italy). Scientific and organizing secretariat: Francesco Zito (Coordinator), Americo Bonanni, Chiara Cerletti, Amalia De Curtis, Augusto Di Castelnuovo, Licia Iacoviello, Roberto Lorenzet, Antonio Mascioli, Marco Olivieri and Domenico Rotilio. Data management and analysis: Augusto Di Castelnuovo (Coordinator), Marialaura Bonaccio, Simona Costanzo and Francesco Gianfagna. Informatics: Marco Olivieri (Coordinator), Maurizio Giacci, Antonella Padulo and Dario Petraroia. Biobank and biomedical analyses: Amalia De Curtis (Coordinator), Federico Marracino, Maria Spinelli, Christian Silvestri. Communication and Press Office: Americo Bonanni (Coordinator), Marialaura Bonaccio and Francesca De Lucia. Moli-family Project: Francesco Gianfagna, Branislav Vohnout. Recruitment staff: Franco Zito (General Coordinator), Secretariat: Mariarosaria Persichillo (Coordinator), Angelita Verna, Maura Di Lillo, Irene Di Stefano, Blood sample: Agostino Pannichella, Antonio Rinaldo Vizzarri, Branislav Vohnout, Agnieszka Pampuch; Spirometry: Antonella Arcari (Coordinator), Daniela Barbato, Francesca Bracone, Simona Costanzo, Carmine Di Giorgio, Sara Magnacca, Simona Panebianco, Antonello Chiovitti, Federico Marracino, Sergio Caccamo, Vanesa Caruso; Electrocardiograms: Livia Rago (Coordinator), Daniela Cugino, Francesco Zito, Francesco Gianfagna, Alessandra Ferri, Concetta Castaldi, Marcella Mignogna; Tomasz Guszcz; Questionnaires: Romina di Giuseppe (Coordinator), Paola Barisciano, Lorena Buonaccorsi, Floriana Centritto, Antonella Cutrone, Francesca De Lucia, Francesca Fanelli, Iolanda Santimone, Anna Sciarretta, Maura Di Lillo, Isabella Sorella, Irene Di Stefano, Emanuela Plescia, Alessandra Molinaro and Christiana Cavone. Call Center: Giovanna Galuppo, Maura Di Lillo, Concetta Castaldi, Dolores D’Angelo and Rosanna Ramacciato. Follow-up: Simona Costanzo (Coordinator); Data management: Simona Costanzo, Marco Olivieri; Event adjudication: Livia Rago (Coordinator), Simona Costanzo, Amalia De Curtis, Licia Iacoviello, Mariarosaria Persichillo. Regional Health Institutions: Azienda Sanitaria Regionale del Molise (ASReM, Campobasso, Italy), UOC Servizio Igiene e Sanità Pubblica-Dipartimento di Prevenzione; Offices of vital statistics of the Molise region and Molise Dati Spa (Campobasso, Italy). Hospitals: Presidi Ospedalieri ASReM (Presidio Ospedaliero A. Cardarelli - Campobasso, Ospedale F. Veneziale - Isernia, Ospedale San Timoteo - Termoli (CB), Ospedale Ss. Rosario. Venafro (IS), Ospedale Vietri – Larino (CB), Ospedale San Francesco Caracciolo - Agnone (IS), Istituto di cura Villa Maria - Campobasso; Fondazione di Ricerca e Cura Giovanni Paolo II - Campobasso; IRRCS Neuromed - Pozzilli (IS), Italy.
Footnotes
Check the online version for the most updated information on this article, online supplements, and information on authorship & disclosures: www.haematologica.org/content/101/11/1434
Funding
The enrolment phase of the Moli-sani study was supported by research grants from Pfizer Foundation (Rome, Italy), the Italian Ministry of University and Research (MIUR, Rome, Italy)–Programma Triennale di Ricerca, Decreto no.1588 and Instrumentation Laboratory, Milan, Italy. Marialaura Bonaccio was supported by a Fondazione Umberto Veronesi Fellowship. The present analyses were partially supported by the Italian Ministry of Health 2013 [Grant number GR-2013-02356060] and by the Italian Association for Cancer Research (A.I.R.C.) with grant AIRC“5×1000” Ref. n. 12237.
Funders had no role in study design, collection, analysis, and interpretation of data; in the writing of the manuscript and in the decision to submit the article for publication. All authors were and are independent from funders.
References
- 1.Barbaresko J, Koch M, Schulze MB, Nöthlings U. Dietary pattern analysis and biomarkers of low-grade inflammation: a systematic literature review. Nutr Rev. 2013;71 (8):511–527. [DOI] [PubMed] [Google Scholar]
- 2.Danesh J, Whincup P, Walker M, et al. Low grade inflammation and coronary heart disease: prospective study and updated meta-analyses. BMJ. 2000;321(7255):199–204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Engstrom G, Hedblad B, Stavenow L, et al. Inflammation-Sensitive Plasma Proteins and Incidence of Myocardial Infarction in Men With Low Cardiovascular Risk. Arterioscler Thromb Vasc Biol. 2004;24(8):1498–1502. [DOI] [PubMed] [Google Scholar]
- 4.Lind L. Circulating markers of inflammation and atherosclerosis. Atherosclerosis. 2003;169(2):203–214. [DOI] [PubMed] [Google Scholar]
- 5.Coussens LM, Werb Z. Inflammation and cancer. Nature. 2002;420(6917):860–867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Samuels Martin A. Inflammation and neurological disease. Curr Opin Neurol. 2004;17(3):307–309. [DOI] [PubMed] [Google Scholar]
- 7.Schnabel RB, Yin X, Larson MG, et al. Multiple inflammatory biomarkers in relation to cardiovascular events and mortality in the community. Arterioscler Thromb Vasc Biol. 2013;33(7):1728–1733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mendall MA, Strachan DP, Butland BK, et al. C-reactive protein: relation to total mortality, cardiovascular mortality and cardiovascular risk factors in men. Eur Heart J. 2000;21(19):1584–1590. [DOI] [PubMed] [Google Scholar]
- 9.Matsumoto K, Sera Y, Abe Y, Ueki Y, Tominaga T, Miyake S. Inflammation and insulin resistance are independently related to all-cause of death and cardiovascular events in Japanese patients with type 2 diabetes mellitus. Atherosclerosis. 2003;169(2):317–321. [DOI] [PubMed] [Google Scholar]
- 10.Pierce BL, Ballard-Barbash R, Bernstein L, et al. Elevated biomarkers of inflammation are associated with reduced survival among breast cancer patients. J Clin Oncol. 2009;27(21):3437–3444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rathcke CN, Raymond I, Kistorp C, Hildebrandt P, Faber J, Vestergaard H. Low grade inflammation as measured by levels of YKL-40: association with an increased overall and cardiovascular mortality rate in an elderly population. Int J Cardiol. 2010;143 (1):35–42. [DOI] [PubMed] [Google Scholar]
- 12.Candore G, Caruso C, Jirillo E, Magrone T, Vasto S. Low grade inflammation as a common pathogenetic denominator in age-related diseases: novel drug targets for anti-ageing strategies and successful ageing achievement. Curr Pharm Des. 2010;16 (6):584–596. [DOI] [PubMed] [Google Scholar]
- 13.Rienstra M, Sun JX, Magnani JW, et al. White blood cell count and risk of incident atrial fibrillation (from the Framingham Heart Study). Am J Cardiol. 2012;109(4):533–537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Danesh J, Collins R, Appleby P, Peto R. Association of fibrinogen, C-reactive protein, albumin, or leukocyte count with coronary heart disease: meta-analyses of prospective studies. JAMA. 1998;279(18): 1477–1482. [DOI] [PubMed] [Google Scholar]
- 15.Danesh J, Wheeler JG, Hirschfield GM, et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N Engl J Med. 2004;35 (14):1387–1397. [DOI] [PubMed] [Google Scholar]
- 16.Arcari A, Zito F, Di Castelnuovo A, et al. C reactive protein and its determinants in healthy men and women from European regions at different risk of coronary disease: the IMMIDIET Project. J Thromb Haemost. 2008;6(3):436–443. [DOI] [PubMed] [Google Scholar]
- 17.Bonaccio M, Di Castelnuovo A, De Curtis A, et al. Adherence to the Mediterranean diet is associated with lower platelet and leukocyte counts: results from the MOLI-SANI study. Blood. 2014;123(19):3037–3044. [DOI] [PubMed] [Google Scholar]
- 18.Bhat T, Teli S, Rijal J, et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther. 2013;11(1):55–59. [DOI] [PubMed] [Google Scholar]
- 19.Bonaccio M, Di Castelnuovo A, Rago L, et al. T-wave axis deviation is associated with biomarkers of low-grade inflammation. Findings from the MOLI-SANI study. Thromb Haemost. 2015;114(6):1199–1206. [DOI] [PubMed] [Google Scholar]
- 20.Yudkin JS, Juhan-Vague I, Hawe E, et al. Low-grade inflammation may play a role in the etiology of the metabolic syndrome in patients with coronary heart disease: the HIFMECH study. Metabolism. 2004;53(7): 852–857. [DOI] [PubMed] [Google Scholar]
- 21.van Bussel BC, Henry RM, Ferreira I, et al. A healthy diet is associated with less endothelial dysfunction and less low-grade inflammation over a 7-year period in adults at risk of cardiovascular disease. J Nutr. 2015;145(3):532–540. [DOI] [PubMed] [Google Scholar]
- 22.Pounis G, Bonaccio M, Di Castelnuovo A, et al. Polyphenol intake is associated with low-grade inflammation, using a novel data analysis from the Moli-sani study. Thromb Haemost. 2015;115(2):344–352. [DOI] [PubMed] [Google Scholar]
- 23.Di Castelnuovo A, Costanzo S, Persichillo M, et al. Distribution of short and lifetime risks for cardiovascular disease in Italians. Eur J Prev Cardiol. 2012;19(4):723–730. [DOI] [PubMed] [Google Scholar]
- 24.Murtaugh PA. In defense of P values. Ecology. 2014;95(3):611–617. [DOI] [PubMed] [Google Scholar]
- 25. [Accessed on December 2015]. http://www.euro.who.int/__data/assets/pdf_file/0004/185215/Leading-causes-of-death-in-Europe-Fact-Sheet.pdf.
- 26.Ferrucci L, Corsi A, Lauretani F, et al. The origins of age-related proinflammatory state. Blood. 2005;105(6):2294–2299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Donati MB. The “common soil hypothesis”: evidence from population studies¿ Thromb Res. 2010;125 Suppl 2:S92–95. [DOI] [PubMed] [Google Scholar]
- 28.Bonaccio M, Cerletti C, Iacoviello L, de Gaetano G. Mediterranean diet and low-grade subclinical inflammation: the Moli-sani study. Endocr Metab Immune Disord Drug Targets. 2015;15(1):18–24. [DOI] [PubMed] [Google Scholar]
- 29.Engström G, Hedblad B, Rosvall M, Janzon L, Lindgärde F. Occupation, marital status, and low-grade inflammation: mutual confounding or independent cardiovascular risk factors¿ Arterioscler Thromb Vasc Biol. 2006;26(3):643–648. [DOI] [PubMed] [Google Scholar]
- 30.Ross R. Atherosclerosis-An inflammatory disease. N Engl J Med. 1999; 340(2):115–126. [DOI] [PubMed] [Google Scholar]
- 31.Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352(16):1685–1695. [DOI] [PubMed] [Google Scholar]
- 32.Ridker PM. Closing the loop on inflammation and atherothrombosis: why perform the CIRT and CANTOS trials¿ Trans Am Clin Climatol Assoc. 2013;124:174–190. [PMC free article] [PubMed] [Google Scholar]
- 33.Lawlor DA, Smith GD, Rumley A, Lowe GD, Ebrahim S. Associations of fibrinogen and C-reactive protein with prevalent and incident coronary heart disease are attenuated by adjustment for confounding factors. British Women’s Heart and Health Study. Thromb Haemost. 2005;93(5):955–963. [DOI] [PubMed] [Google Scholar]
- 34.Sanchez PL, Morinigo JL, Pabon P, et al. Prognostic relations between inflammatory markers and mortality in diabetic patients with non-ST elevation acute coronary syndrome. Heart. 2004;90(3):264–269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.de Jager J, Dekker JM, Kooy A, et al. Endothelial Dysfunction and Low-Grade Inflammation Explain Much of the Excess Cardiovascular Mortality in Individuals With Type 2 Diabetes. Arterioscler Thromb Vasc Biol. 2006;26(5):1086–1093. [DOI] [PubMed] [Google Scholar]
- 36.Volpato S, Guralnik JM, Ferrucci L, et al. Cardiovascular disease, interleukin-6, and risk of mortality in older women: the women’s health and aging study. Circulation. 2001;103(7):947–953. [DOI] [PubMed] [Google Scholar]
- 37.Badimon L, Padró T, Vilahur G. Atherosclerosis, platelets and thrombosis in acute ischaemic heart disease. Eur Heart J Acute Cardiovasc Care. 2012;1(1):60–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.van der Wal AC, Becker AE, van der Loos CM, Das PK. Site of intimal rupture or erosion of thrombosed coronary atherosclerotic plaques is characterized by an inflammatory process irrespective of the dominant plaque morphology. Circulation. 1994;89(1):36–44. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.