

Abstract
Background
Colistin has been considered as a last-line treatment option in severe infections caused by multidrug-resistant (MDR) gram-negative pathogens. However, the emergence of the mobile colistin resistance gene (mcr-1) has challenged this viewpoint. The aim of this study is to explore the prevalence of mcr-1 in Escherichia coli (E. coli) in a Chinese teaching hospital, and investigate their molecular characteristics.
Methods
A total of 700 E. coli isolates were used to screen mcr-1 by PCR and sequencing in a Chinese university hospital from August 2014 to August 2015. Susceptibility test of mcr-1-producing isolates was determined by Vitek -2 Compact system. 26 virulence factors (VFs), phylogenetic groups, Multi-locus sequence typing (MLST), and DNA Fingerprinting (ERIC-PCR) of strains were investigated by PCR.
Results
Four (0.6%) mcr-1 producing E. coli isolates were found in this study. The results of antibiotic susceptibility test showed that all four isolates were resistant to colistin, ciprofloxacin, levofloxacin, cefazolin, and trimethoprim/sulfamethoxazole, and were susceptible to amikacin, ertapenem and imipenem. In addition, all 4 isolates exhibited high-level resistance to aztreonam, cefotaxime and gentamicin. The numbers of VFs contained in mcr-1 positive isolates were no more than 4 in our study. MLST result demonstrated that these isolates were assigned to two sequence types: ST156 and ST167. The result of phylogenetic analysis showed that four mcr-1-positive isolates belong to two phylogenetic groups: A and B1 group. ERIC-PCR showed that four mcr-1 positive strains were categorized into three different genotypes.
Conclusions
Our study demonstrated a low prevalence of mcr-1 in E. coli clinical isolates in a Chinese teaching hospital, and we have gained insights into the molecular characteristics of these mcr-1-positive strains. Increasing the surveillance of these infections, as well as taking effective infection control measures are urgently needed to take to control the transmission of mcr-1 gene.
Keywords: E. coli, mcr-1, Colistin, Multidrug-resistant
Background
In recent years, colistin has been considered as an effective therapeutic option for the rapid increasing of multidrug-resistant (MDR) gram-negative pathogens [1, 2]. However, the prevalence of the mobile colistin resistance gene (mcr-1) in animals and human beings worldwide has challenged this viewpoint [3, 4]. Resistance to polymyxins is mainly caused by the modification to bacterial outer membrane, which was usually considered as chromosomally mediated resistance [5, 6].
Since it was initially found, plasmid-mediated mcr-1 has been detected widely [3, 7]. Nowadays, mcr-1-producing bacteria have been reported in many regions in China [4, 8]. Mcr-1 was firstly found in Escherichia coli (E. coli), and now it has been spreading to other Enterobacteriaceae [9]. Several reports showed that the mcr-1 gene could coexist with other resistance genes (such as CRE/ESBL) in E. coli and Klebsiella pneumoniae, which probably lead to the emergence pan-drug resistant and increase the difficulty of treatment [8, 10]. Therefore, the emergence and spread of mcr-1 gene among human beings should be given close attention. The aim of this study was to evaluate the prevalence of mcr-1 in E. coli clinical isolates in a Chinese teaching hospital, and to investigate the molecular characteristics of these strains.
Methods
Bacterial strains
A total of 700 E. coli clinical isolates were collected from the clinical laboratory of Fujian Medical University Union Hospital (Fuzhou, Fujian province, China) from August 2014 to August 2015. It is a 2200-bed tertiary care teaching hospital with approximately 95,000 hospital admissions per year, located in southeastern China. All isolates were identified by GNI card of the Vitek system (BioMèrieux, Missouri, France).
Antibiotic susceptibility testing
Antimicrobial susceptibility testing was performed using the AST-GN16 of Vitek-2 Compact system (Bio Mérieux, France). The antimicrobial agents tested included: tigecycline (glycycline); ertapenem and imipenem (carbapenems); cefazolin; cefoxitin; cefepime, and cefotaxime (cephalosporins); aztreonam (monobactam); amikacin and gentamicin (aminoglycosides); ciprofloxacin and levofloxacin (quinolone); piperacillin/tazobactam; trimethoprim/sulfamethoxazole. The results were interpreted by the Clinical and Laboratory Standards Institute (CLSI) [11]. The MIC of colistin was determined using agar dilution method, and the result was interpreted according to European Committee On Antimicrobial Susceptibility Testing (EUCAST) guidelines [12]. E. coli ATCC 25922 was used as a quality control.
DNA extraction
Several colonies were suspended in 50 µl of sterile distilled water for preparing genomic DNA of the isolates, and then the bacterial suspension was heated at 100 °C for 10 min as described previously [13].
MCR-1 detection
mcr-1 gene was screened in E. coli clinical isolates by PCR using primers as previously described [4]. All of the PCR products were sequenced and then compared with known sequences listed in the GenBank (http://www.ncbi.nlm.nih.gov/blast/).
Detection of virulence factor genes
Twenty six virulence factors (VFs) genes associated with extraintestinal virulence [14, 15] were detected using a multiplex PCR method as previously described [15]. These genes were as follows: adhesions (papAH, papEF, papC, papG allele I, papG II/III, papG allele II, sfa/focDE, afa/draBC, fimH, gafD, sfaS, focG and nfaE), toxins (hlyA, cnf1 and cdtB), siderophores (fyuA and iutA), protections and invasions (kpsMTII, kpsMTIII, traT, cvaC, kpsMT and K1/K5), miscellaneous (rfc and PAI). The PCR products were sequenced and then compared with known sequences listed in the GenBank (http://www.ncbi.nlm.nih.gov/blast/).
Phylogenetic analysis
The phylogenetic groups (A, B1, B2, and D) of mcr-1 producing E. coli isolates were identified by a triplex PCR as previously described [16].
Multi-locus sequence typing (MLST)
Mcr-1 positive strains were analyzed by multilocus sequence typing (MLST), which was based on 7 standard housekeeping genes (adk, fumC, gyrB, icd, mdh, purA, recA) (http://mlst.ucc.ie/mlst/mlst/dbs/Ecoli) [17].
DNA fingerprinting
Enterobacterial Repetitive Intergenic Consensus Sequences PCR (ERIC-PCR) was applied to typing mcr-1 producing E. coli isolates with the primers ERIC-1 and ERIC-2 [18]. DNA fingerprints were compared by visual inspection, ERIC profiles were regarded as different if there were different bands on visual inspection [19].
Results and discussion
In this study, four isolates (0.6%) were confirmed to carry mcr-1 gene, which is lower than previous study [4]. The age of the patients ranged between 38 and 80 years. These mcr-1 producing strains were isolated from two different wards (Table 1). Two strains were isolated from the same patient. The clinical data of patients with mcr-1 positive E. coli infection were shown in Table 2.
Table 1.
Main characteristics of the mcr-1 E. coli
| Isolates | Data | Ward | Specimen | Phylogenetic groups | MLST | ERIC pattern | VFs | Antibiotic resistance |
|---|---|---|---|---|---|---|---|---|
| E321 | 2014.8 | Colorectal surgery | Drainage-fluid | B1 | ST156 | 1 | traT, iutA | COL, CFZ, FOX, CIP, LVX, SXT, TGC |
| E684 | 2015.1 | Colorectal surgery | Secretion | B1 | ST156 | 2 | fimH, traT, iutA | COL, CFZ, CTX, FEP, ATM, GEN, CIP, LVX, SXT |
| E921 | 2015.4 | Hepatobiliary surgery | Secretion | A | ST167 | 3 | fyuA, traT, iutA | COL, CFZ, CTX, ATM, GEN, CIP, LVX, SXT |
| E1005 | 2015.5 | Hepatobiliary surgery | Drainage-fluid | A | ST167 | 3 | fyuA, cvaC, traT, iutA | COL, CFZ, CTX, ATM, GEN, CIP, LVX, SXT |
CFZ cefazolin, FOX cefoxitin, CTX cefotaxime, FEP cefepime, TZP piperacillin/tazobactam, ATM aztreonam, IPM imipenem, ETP ertapenem, AMK amikacin, GEN gentamicin, CIP ciprofloxacin, LVX levofloxacin, SXT trimethoprim/sulfamethoxazole, TIG tigecycline, COL colistin, MLST multi-locus sequence typing, ERIC enterobacterial repetitive intergenic consensus, VFs virulence factor genes
Table 2.
Clinical data of patients with mcr-1 positive E. coli infection
| Isolates | Patients | Gender | Age (years) | Underlying diseases | Length of hospital stay (days) | Treatments used | Outcomes |
|---|---|---|---|---|---|---|---|
| E321 | Patient 1 | Female | 80 | Malignancy, hypertension, pulmonary tuberculosis | 51 | TZP | Survived |
| E684 | Patient 2 | Female | 57 | Perineal infection, hypertension | 37 | TZP | Survived |
| E921 | Patient 3 | Male | 38 | Hypertension, pancreatitis, diabetes | 26 | MEM | Survived |
| E1005 | Patient 3 | Male | 38 | Hypertension, pancreatitis, diabetes | 26 | MEM | Survived |
TZP piperacillin/tazobactam, MEM meropenem
Mcr-1 was usually found to be co-localized with other resistance genes on plasmids, such as ESBL genes and carbapenemase genes [20], which might increase the emergence of pan-drug resistance. In our study, the results of antimicrobial susceptibility test showed a high drug resistance in the mcr-1-producing isolates. All of the mcr-1 positive isolates were resistance to at least 3 different kinds of antibiotics (Table 1).
All four mcr-1 positive strains detected in our study were resistant to colistin and the MICs ranged from 4 to 16 μg/ml. It will be worrisome once mcr-1 coexists with other resistant genes, especially carbapenemase genes because of limited therapeutic options [20]. Previous studies revealed that mcr-1 co-produced with carbapenem-resistant genes in E. coli [8, 21]. Fortunately, all of them were susceptible to carbapenems (IPM and ETP), which probably indicated that no carbapenem-resistant genes coexisted with mcr-1. Result of ERIC-PCR (Fig. 1) showed that four mcr-1 positive strains were categorized into three different genotypes, one of which contained 2 strains (from the same patient). These isolates which have different patterns suggest that they were non-clonal transmission. In a previous study, two mcr-1 positive E. coli isolates from a single fowl were belonging to phylogenetic B1 and D group [22]. The mcr-1-producing isolates in this study were belonged to phylogenetic groups A and B1, which were mainly distributed among human commensal E. coli isolates [23]. The mcr-1 producing isolates were assigned by MLST to two different sequence types: ST156 and ST167 (Table 1), which was similar to previous reports in other studies from China [8, 22]. E. coli ST156 has been found that it has connection with different ESBL genes [24, 25]. ST167 was belonged to ST10 complex and regarded as prevalent ST among ESBL-producing E. coli from human and animal sources [26]. In addition, E. coli ST167 was reported to be closely related to bla NDM, which needed closely concern of spreading [27]. The similar molecular characterizations illustrated that mcr-1 positive isolates detected from the same department in our study were clonally related.
Fig. 1.
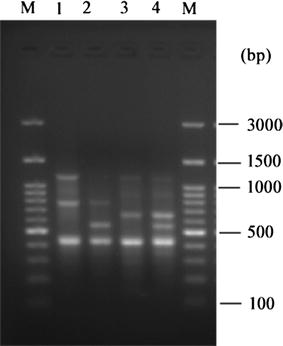
ERIC-PCR products from four mcr-1 positive isolates. M mark, lane 1 E321, lane 2 E684, lane 3 E921, lane 4 E1005
VFs in E. coli were associated with colonization, bacterial fitness and virulence [28]. VFs include five main groups: (1) adhesions; (2) toxins; (3) siderophores; (4) capsule production and (5) protections and invasions. Clinical E. coli strains often carry multiple VFs, and isolates belonging to groups A and B1 often have less VFs than those belonging to phylogroups B2 and D [28]. To the best of our knowledge, there is no study concerning about VFs in mcr-1 producing E. coli. In our study, mcr-1 producing isolates contained less than 4 different VFs (Table 1). Only five different kinds of VFs had been detected in our mcr-1 positive isolates, which included fimH, fyuA, traT, iutA and cvaC. fimH is one of the most commonly VFs present in E. coli, which encodes the adhesion subunit of type 1 fimbriae and related to colonization [15]. Lee et al. reported that fyuA, traT, and iutA were found to be independent predictors for pathogenicity. Meanwhile, traT and iutA were thought to be closely related to ESBL genes [29]. Pitout et al. found that cvaC was only present in non-CTX-M-producing isolates [30]. Previous reports suggested that antibiotic resistance has negative association with virulence factors [31], which could be interpreted by the loss of VFs associated with mutation to resistance [32].
It is noteworthy that two mcr-1 positive E. coli strains were isolated from the same patient but at different time (Table 1). Results of MLST and ERIC-PCR revealed that these isolates had identical genetic background. Result of antimicrobial susceptibility test showed that they had similar antibiograms. We speculate that the two isolates probably originated from a same source.
In conclusion, we have revealed a low prevalence of mcr-1 in E. coli clinical isolates in a Chinese teaching hospital, and presented detailed molecular characteristics of these isolates. The presence of mcr-1 in E. coli clinical isolates suggests that it will pose a threat to public healthcare. Effective infection control measures are urgently needed to take to control the transmission of mcr-1 gene.
Authors’ contributions
QH, XX, FL, ZZ and YC conducted laboratory assays. ZW collected clinical data. QH wrote the paper. BL designed the study and reviewed the manuscript. All authors read and approved the final manuscript.
Acknowledgements
We thank Prof. Jianhua Liu and Yiyun Liu of South China Agricultural University, Guangzhou, China for kindly providing us the mcr-1 positive control. We also thank Prof. Min Chen and Department of Laboratory Medicine, Medical Technology and Engineering College, Fujian Medical University for their kindly help.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
There is no additional data and materials, except those in the sections of “Methods” and “Results and discussion”.
Funding
This study was supported by the National Natural Science Foundation of China (Grant No. 81201328), the Fujian Provincial Funds for Distinguished Young Scientists in Colleges and Universities, China (Grant No. JA13134), and the Medical Elite Cultivation Program of Fujian, China (Grant No. 2015-ZQN-ZD-15).
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- MCR-1
mobile colistin resistance gene
- MDR
multi-drug resistant
- PCR
polymerase chain reaction
- CLSI
Clinical and Laboratory Standards Institute
- MLST
multi-locus sequence typing
- CRE
carbapenem-resistant Enterobacteriaceae
- ESBL
extended-spectrum β-lactamase
- ERIC-PCR
Enterobacterial Repetitive Intergenic Consensus Sequences PCR
- VFs
virulence factors
Contributor Information
Qing-wen He, Email: heqingwen66@126.com.
Xiao-hong Xu, Email: vancy1988@163.com.
Fang-jun Lan, Email: lanfangjun3519@hotmail.com.
Zhi-chang Zhao, Email: 13950342709@126.com.
Zhi-yun Wu, Email: yangziyun37110@163.com.
Ying-ping Cao, Email: caoyingping@aliyun.com.
Bin Li, Phone: +86-591-53357896-8408, Email: leonlee307@hotmail.com.
References
- 1.Nation RL, Li J, Cars O, Couet W, Dudley MN, Kaye KS, Mouton JW, Paterson DL, Tam VH, Theuretzbacher U, et al. Framework for optimisation of the clinical use of colistin and polymyxin B: the Prato polymyxin consensus. Lancet Infect Dis. 2015;15(2):225–234. doi: 10.1016/S1473-3099(14)70850-3. [DOI] [PubMed] [Google Scholar]
- 2.Doi Y, Paterson DL. Carbapenemase-producing Enterobacteriaceae. Semin Respir Crit Care Med. 2015;36(1):74–84. doi: 10.1055/s-0035-1544208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Skov RL, Monnet DL. Plasmid-mediated colistin resistance (mcr-1 gene): 3 months later, the story unfolds. Euro Surveill. 2016;21:9. doi: 10.2807/1560-7917.ES.2016.21.9.30155. [DOI] [PubMed] [Google Scholar]
- 4.Liu YY, Wang Y, Walsh TR, Yi L, Zhang R, Spencer J, Doi Y, Tian G, Dong B, Huang X, et al. Emergence of plasmid-mediated colistin resistance mechanism MCR-1 in animals and human beings in China: a microbiological and molecular biological study. Lancet Infect Dis. 2016;16(2):161–168. doi: 10.1016/S1473-3099(15)00424-7. [DOI] [PubMed] [Google Scholar]
- 5.Giani T, Arena F, Vaggelli G, Conte V, Chiarelli A, Henrici De Angelis L, Fornaini R, Grazzini M, Niccolini F, Pecile P, et al. Large nosocomial outbreak of colistin-resistant, carbapenemase-producing Klebsiella pneumoniae traced to clonal expansion of an mgrB deletion mutant. J Clin Microbiol. 2015;53(10):3341–3344. doi: 10.1128/JCM.01017-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Olaitan AO, Morand S, Rolain JM. Mechanisms of polymyxin resistance: acquired and intrinsic resistance in bacteria. Front Microbiol. 2014;5:643. doi: 10.3389/fmicb.2014.00643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Du H, Chen L, Tang Y, Kreiswirth BN. Emergence of the mcr-1 colistin resistance gene in carbapenem-resistant Enterobacteriaceae. Lancet Infect Dis. 2016;16(3):287–288. doi: 10.1016/S1473-3099(16)00056-6. [DOI] [PubMed] [Google Scholar]
- 8.Yu H, Qu F, Shan B, Huang B, Jia W, Chen C, Li A, Miao M, Zhang X, Bao C, et al. Detection of mcr-1 colistin resistance gene in carbapenem-resistant Enterobacteriaceae from different hospitals in China. Antimicrob Agents Chemother. 2016;60(8):5033–5035. doi: 10.1128/AAC.00440-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Schwarz S, Johnson AP. Transferable resistance to colistin: a new but old threat. J Antimicrob Chemother. 2016;71(8):2066–2070. doi: 10.1093/jac/dkw274. [DOI] [PubMed] [Google Scholar]
- 10.Haenni M, Poirel L, Kieffer N, Chatre P, Saras E, Metayer V, Dumoulin R, Nordmann P, Madec JY. Co-occurrence of extended spectrum beta lactamase and MCR-1 encoding genes on plasmids. Lancet Infect Dis. 2016;16(3):281–282. doi: 10.1016/S1473-3099(16)00007-4. [DOI] [PubMed] [Google Scholar]
- 11.CLSI. Methods for dilution antimicrobial susceptibility tests for bacteria that grow aerobically; approved standard, 10th ed. CLSI document M07-A10. Wayne: Clinical and Laboratory Standards Institute; 2015.
- 12.EUCAST. Breakpoints tables for interpretation of MICs and zone diameters, version 6.0; 2016.
- 13.He Q, Chen W, Huang L, Lin Q, Zhang J, Liu R, Li B. Performance evaluation of three automated identification systems in detecting carbapenem-resistant Enterobacteriaceae. Ann Clin Microbiol Antimicrob. 2016;15(1):40. doi: 10.1186/s12941-016-0154-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Johnson JR, Russo TA. Molecular epidemiology of extraintestinal pathogenic (uropathogenic) Escherichia coli. Int J Med Microbiol. 2005;295(6–7):383–404. doi: 10.1016/j.ijmm.2005.07.005. [DOI] [PubMed] [Google Scholar]
- 15.Johnson JR, Stell AL. Extended virulence genotypes of Escherichia coli strains from patients with urosepsis in relation to phylogeny and host compromise. J Infect Dis. 2000;181(1):261–272. doi: 10.1086/315217. [DOI] [PubMed] [Google Scholar]
- 16.Clermont O, Bonacorsi S, Bingen E. Rapid and simple determination of the Escherichia coli phylogenetic group. Appl Environ Microbiol. 2000;66(10):4555–4558. doi: 10.1128/AEM.66.10.4555-4558.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Johnson JR, Clermont O, Johnston B, Clabots C, Tchesnokova V, Sokurenko E, Junka AF, Maczynska B, Denamur E. Rapid and specific detection, molecular epidemiology, and experimental virulence of the O16 subgroup within Escherichia coli sequence type 131. J Clin Microbiol. 2014;52(5):1358–1365. doi: 10.1128/JCM.03502-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Smith JL, Drum DJ, Dai Y, Kim JM, Sanchez S, Maurer JJ, Hofacre CL, Lee MD. Impact of antimicrobial usage on antimicrobial resistance in commensal Escherichia coli strains colonizing broiler chickens. Appl Environ Microbiol. 2007;73(5):1404–1414. doi: 10.1128/AEM.01193-06. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Manges AR, Johnson JR, Foxman B, O’Bryan TT, Fullerton KE, Riley LW. Widespread distribution of urinary tract infections caused by a multidrug-resistant Escherichia coli clonal group. N Engl J Med. 2001;345(14):1007–1013. doi: 10.1056/NEJMoa011265. [DOI] [PubMed] [Google Scholar]
- 20.Schwarz S, Johnson AP. Transferable resistance to colistin: a new but old threat. J Antimicrob Chemother. 2016;71:2066–2070. doi: 10.1093/jac/dkw274. [DOI] [PubMed] [Google Scholar]
- 21.Li A, Yang Y, Miao M, Chavda KD, Mediavilla JR, Xie X, Tang YW. Complete sequences of mcr-1-harboring plasmids from extended-spectrum-beta-lactamase- and carbapenemase-producing Enterobacteriaceae. Antimicrob Agents Chemother. 2016;60(7):4351–4354. doi: 10.1128/AAC.00550-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yang RS, Feng Y, Lv XY, Duan JH, Chen J, Fang LX, Xia J, Liao XP, Sun J, Liu YH. Emergence of NDM-5 and MCR-1-producing Escherichia coli clone ST648 and ST156 from a single muscovy duck (Cairina moschata) Antimicrob Agents Chemother. 2016;60:6899–6902. doi: 10.1128/AAC.01365-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Pitout JD. Extraintestinal pathogenic Escherichia coli: an update on antimicrobial resistance, laboratory diagnosis and treatment. Exp Rev Anti Infect Ther. 2012;10(10):1165–1176. doi: 10.1586/eri.12.110. [DOI] [PubMed] [Google Scholar]
- 24.Cortes-Cortes G, Lozano-Zarain P, Torres C, Castaneda M, Moreno Sanchez G, Alonso CA, Lopez-Pliego L, Gutierrez Mayen MG, Martinez-Laguna Y, Rocha-Gracia RD. Detection and molecular characterization of Escherichia coli strains producers of extended-spectrum and CMY-2 type beta-lactamases, isolated from turtles in Mexico. Vector Borne Zoonotic Dis. 2016;16:595–603. doi: 10.1089/vbz.2014.1725. [DOI] [PubMed] [Google Scholar]
- 25.Pan YS, Liu JH, Hu H, Zhao JF, Yuan L, Wu H, Wang LF, Hu GZ. Novel arrangement of the blaCTX-M-55 gene in an Escherichia coli isolate coproducing 16S rRNA methylase. J Basic Microbiol. 2013;53(11):928–933. doi: 10.1002/jobm.201200318. [DOI] [PubMed] [Google Scholar]
- 26.Schink AK, Kadlec K, Kaspar H, Mankertz J, Schwarz S. Analysis of extended-spectrum-beta-lactamase-producing Escherichia coli isolates collected in the GERM-Vet monitoring programme. J Antimicrob Chemother. 2013;68(8):1741–1749. doi: 10.1093/jac/dkt123. [DOI] [PubMed] [Google Scholar]
- 27.Huang Y, Yu X, Xie M, Wang X, Liao K, Xue W, Chan EW, Zhang R, Chen S. Widespread dissemination of carbapenem-resistant Escherichia coli sequence type 167 strains harboring blaNDM-5 in clinical settings in China. Antimicrob Agents Chemother. 2016;60(7):4364–4368. doi: 10.1128/AAC.00859-16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Smith JL, Fratamico PM, Gunther NW. Extraintestinal pathogenic Escherichia coli. Foodborne Pathog Dis. 2007;4(2):134–163. doi: 10.1089/fpd.2007.0087. [DOI] [PubMed] [Google Scholar]
- 29.Lee S, Yu JK, Park K, Oh EJ, Kim SY, Park YJ. Phylogenetic groups and virulence factors in pathogenic and commensal strains of Escherichia coli and their association with blaCTX-M. Ann Clin Lab Sci. 2010;40(4):361–367. [PubMed] [Google Scholar]
- 30.Pitout JD, Laupland KB, Church DL, Menard ML, Johnson JR. Virulence factors of Escherichia coli isolates that produce CTX-M-type extended-spectrum beta-lactamases. Antimicrob Agents Chemother. 2005;49(11):4667–4670. doi: 10.1128/AAC.49.11.4667-4670.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Skjot Rasmussen L, Ejrnaes K, Lundgren B, Hammerum AM, Frimodt Moller N. Virulence factors and phylogenetic grouping of Escherichia coli isolates from patients with bacteraemia of urinary tract origin relate to sex and hospital- vs. community-acquired origin. Int J Med Microbiol. 2012;302(3):129–134. doi: 10.1016/j.ijmm.2012.03.002. [DOI] [PubMed] [Google Scholar]
- 32.Vila J, Simon K, Ruiz J, Horcajada JP, Velasco M, Barranco M, et al. Are quinolone-resistant uropathogenic Escherichia coli less virulent? J Infect Dis. 2002;186(7):1039–1042. doi: 10.1086/342955. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
There is no additional data and materials, except those in the sections of “Methods” and “Results and discussion”.