

Abstract
AIM
To analyse ground reaction forces at higher speeds using another method to be more sensitive in assessing significant gait abnormalities.
METHODS
A total of 44 subjects, consisting of 24 knee osteoarthritis (OA) patients and 20 healthy controls were analysed. The knee OA patients were recruited from an orthopaedic clinic that were awaiting knee replacement. All subjects had their gait patterns during stance phase at top walking speed assessed on a validated treadmill instrumented with tandem force plates. Temporal measurements and ground reaction forces (GRFs) along with a novel impulse technique were collected for both limbs and a symmetry ratio was applied to all variables to assess inter-limb asymmetry. All continuous variables for each group were compared using a student t-test and χ2 analysis for categorical variables with significance set at α = 0.05. Receiver operator characteristics curves were utilised to determine best discriminating ability.
RESULTS
The knee OA patients were older (66 ± 7 years vs 53 ± 9 years, P = 0.01) and heavier (body mass index: 31 ± 6 vs 23 ± 7, P < 0.001) but had a similar gender ratio when compared to the control group. Knee OA patients were predictably slower at top walking speed (1.37 ± 0.23 m/s vs 2.00 ± 0.20 m/s, P < 0.0001) with shorter mean step length (79 ± 12 cm vs 99 ± 8 cm, P < 0.0001) and broader gait width (14 ± 5 cm vs 11 ± 3 cm, P = 0.015) than controls without any known lower-limb joint disease. At a matched mean speed (1.37 ± 0.23 vs 1.34 ± 0.07), ground reaction results revealed that push-off forces and impulse were significantly (P < 0.0001) worse (18% and 12% respectively) for the knee OA patients when compared to the controls. Receiver operating characteristic curves analysis demonstrated total impulse to be the best discriminator of asymmetry, with an area under the curve of 0.902, with a cut-off of -3% and a specificity of 95% and sensitivity of 88%.
CONCLUSION
Abnormal GRFs in knee osteoarthritis are clearly evident at higher speeds. Analysing GRFs with another method may explain the general decline in knee OA patient’s gait.
Keywords: Gait, Treadmill, Ground reaction forces, Symmetry, Osteoarthritis, Knee
Core tip: Top walking speed may unmask significant abnormalities which would not be seen at slower walking speeds. The use of impulse rather than solitary peaks in the analysis of ground reaction forces may be more sensitive in detecting significant abnormalities in gait.
INTRODUCTION
Difficulty walking is one of the principal symptoms reported by patients with knee osteoarthritis (OA). Analysis of gait symmetry between right and left legs has been shown useful in identifying lower limb joint disease, particularly osteoarthritis[1]. Such data may be useful as a trigger for clinical intervention, given that significant asymmetry may lead to falls, injury to other joints and declining walking activity[2,3].
Previous studies analysing gait symmetry in OA are arguably limited in value by their use of slow speed gait protocols[4], with more recent studies demonstrating that slower speeds are employed as a protective mechanism by the patient, and can disguise the significant gait abnormalities apparent at higher speeds[5]. Furthermore, analysis at faster walking speeds may provide insight into why self-selected walking speed is reduced in knee OA patients, which is of particular interest given that a slow walking speed has been associated with decreased life expectancy[6].
Biomechanical (obesity, joint instability and malalignment) factors play an important role in the development of OA[7,8], and the vertical ground reaction force (GRF) measured in gait laboratories is a useful non-invasive surrogate of internal joint loading[9]. Although repeatable and well described, GRF results are surprisingly variable in the published literature, which is likely due to the uncontrolled variation in walking speed during assessments[5]. Analysing GRF symmetry offers a potential method of removing the effect introduced by variations in speed, given that the patient’s normal limb acts as a control when compared to the diseased contralateral limb. Moreover, most studies only use single “peak” data points for GRF during the gait cycle[10], which may fail to capture the variation between subjects afforded by a more detailed analysis.
The aim of the study was to: (1) assess the gait patterns and symmetry of patients with knee OA at top walking speed with the aid of an instrumented treadmill; and (2) apply a new method of assessing ground reaction force symmetry. The null hypothesis was that top walking speed and a new method of analysis would show no differences.
MATERIALS AND METHODS
Participants
A total of 44 subjects, consisting of 24 knee OA patients and 20 healthy controls, were included in this study ethically approved by the joint research office (10/H0807/101). Patients with unilateral symptomatic knee OA awaiting knee arthroplasty were recruited from an orthopaedic knee clinic. All subjects had primary knee osteoarthritis and were cardio-vascularly fit, with no further lower limb or joint disease. Standard pre-operative knee radiographs of the OA patient group were used to assess disease severity using Kellgren and Lawrence (KL) grading[11]. In order to aid validity and interpretation of subsequent data, patients with neurological, medical or other lower limb conditions were excluded, as these variables may also have affected walking ability. This study utilised a control group comprising of healthy staff members, who were free from neurological or joint problems. Test subjects were recruited by a single research assistant. Gait analysis was undertaken using a blinded assessor to avoid testing bias.
Gait analysis and data collection
Gait analysis was performed using a validated treadmill instrumented with tandem piezo-electric force plates (Kistler Gaitway®, Kistler Instrument Corporation, Amherst NY). All participants gave informed consent before treadmill testing began. After an acclimatisation period at 4 km/h, speed was increased incrementally until top walking speed (TWS) performance had been attained. TWS was defined as the fastest speed a subject could walk without running. All walking measurements were collected without the aid of any props using a standardised testing protocol[12]. Vertical ground reaction forces, centre of pressure (COP) and temporal measurements were collected for both limbs with a sampling frequency of 100 Hz over 10 s. Gait data was subject to averaging by a custom written MATLAB software script as a 10 s interval normally recorded a minimum of 5 steps for each limb. A validated body weight normalising (BWN) was applied to the force results to correct for mass differences[13].
BWN force = Ground reaction force/(body mass × gravity)
The data was further divided into affected (A)/unaffected (UA) limb for the OA group, and right/left limb for the healthy controls. A previously described and validated symmetry ratio (SR)[14], was applied to all variables.
SR= [(XA/XUA) - 1] x 100%
SR values describe the percentage difference between limbs, with zero indicating complete symmetry. Negative values indicated worsening asymmetry with respect to the affected limb in the OA group and the right limb in the control group.
Impulse values were calculated from the vertical GRF data. Impulse takes into account both the magnitude of loading and duration of stance phase of a limb. The total and each phase peak of impulse was assessed on the “M” pattern force curve, comprising weight acceptance (WA) and push-off (PO) impulse. These peaks were identified using a MATLAB script to segment the data, with the limits of integration defined as 5% of force time either side of the maximum value. Figure 1 illustrates the calculation of weight acceptance impulse during stance phase between right and left legs. The same technique was also used for push-off and total impulse used the entire curve.
Figure 1.
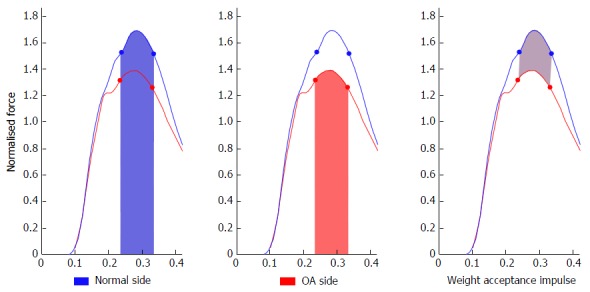
Impulse analysis during weight acceptance: Comparing the knee osteoarthritis limb to the contralateral normal side. OA: Osteoarthritis.
Statistical analysis
Statistical analysis was performed with SPSS (IBM SPSS Statistics, version 20). For continuous variables between the groups an independent t-test was used and for categorical variable (gender), a χ2 test was used. A significance level of α = 0.05 was employed throughout. Shapiro-Wilk test showed the gait variables to be normally distributed. Variable data is presented as means with standard deviations.
Receiver operating characteristics (ROC) curves were utilised to determine which gait symmetry variables had the best discriminating ability. Categorisation of the area under the curve (AUC) was performed, with AUC above 0.7 determined as fair, above 0.8 good and above 0.9 as excellent discriminating ability[15].
OA patients’ top walking speed results were predictably slower than the healthy group, and were hence also compared to the healthy group’s preferred walking speed, which was more comparable.
RESULTS
Patient and control characteristics are provided in Table 1. The most common disease severity grade of OA was 2 using Kellgren and Lawrence system. Nineteen patients had medial tibiofemoral OA with an element of patellofemoral OA. Two patients had lateral tibiofemoral OA and remaining three had primarily patellofemoral OA. None of the patients had significant joint bone deformity and an intermediate grade of knee OA can be concluded.
Table 1.
Subject characteristics
| Subject | Control | Knee OA |
| Sex M:F | 7:13 | 8:16 |
| Age (yr) | 52.5 (8.8) | 65.5 (7.2)1 |
| BMI | 23.2 (6.6) | 31.2 (6.1)1 |
| Leg length (cm) | 89.3 (5.6) | 85.1 (5.9)1 |
| Height (cm) | 168.5 (7.5) | 164.1 (7.9) |
| Total KL score | NA | 2.5 (1.1) |
Significant difference between OA group vs control at PWS (P < 0.05). OA: Osteoarthritis; NA: Not available; PWS: Preferred walking speed; KL: Kellgren and Lawrence; BMI: Body mass index.
Preferred and top walking speed for the knee OA patients was predictably and significantly slower (P < 0.0001) than the controls (1.09 m/s vs 1.34 m/s and 1.37 m/s vs 2.00 m/s respectively). Step length was also reduced at TWS (79 cm vs 99 cm, P < 0.0001), with a broader gait width (14 cm vs 11 cm, P = 0.015) as seen in Table 2. As ground reaction forces are partly speed dependent[16] (Figure 2), analysis comparing the knee OA results to the control group’s preferred walking speed was done given that they were similar (1.34 m/s vs 1.37 m/s P = 0.56). Push-off force and total impulse were significantly (P < 0.0001) less (22% and 12% respectively) than the controls (Table 2 and Figure 3). This was also seen at the knee OA preferred walking speed, but became more pronounced at top walking speed. The knee OA patients were also significantly more asymmetrical than the healthy controls, with the greatest difference between limbs (Table 2) seen during single limb stance time (8%, P = 0.001), push-off impulse (7%, P = 0.050) and total impulse (7%, P < 0.0001). ROC analysis of the gait symmetry variables (Table 3) at TWS demonstrated that total impulse (Figure 4) was the best discriminator of symmetry with an AUC of 0.902, with a cut-off of -3% and a specificity of 95% and sensitivity of 88%.
Table 2.
Temporospatial and normalised ground reaction results
| Variable |
Knee OA PWS |
Symmetry ratio % |
Control PWS |
Symmetry ratio % |
Knee OA TWS |
Symmetry ratio % |
Control TWS |
Symmetry ratio % | ||||
| Affected | Unaffected | Right | Left | Affected | Unaffected | Right | Left | |||||
| (n = 24) | (n = 24) | (n = 20) | (n = 20) | (n = 24) | (n = 24) | (n = 24) | (n = 20) | (n = 20) | ||||
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Speed (m/s) | 1.091 (0.14) | NA | 1.34 (0.07) | NA | 1.372 (0.23) | NA | 2.00 (0.20) | NA | ||||
| Cadence (step/min) | 113 (7) | NA | 114 (10) | NA | 1231,2 (9) | NA | 137 (11) | NA | ||||
| Gait width (cm) | 14.6 (4.2)1 | NA | 11.2 (3.2) | NA | 14.21,2 (4.5) | NA | 11.2 (3.0) | NA | ||||
| Weight acceptance (BWN) | 1.071 (0.08) | 1.121 (0.10) | -4.01 (5.7) | 1.18 (0.08) | 1.18 (0.07) | 0.7 (2.0) | 1.182 (0.14) | 1.261,2 (0.16) | -5.9 (5.7)1,2 | 1.55 (0.12) | 1.52 (0.12) | 2.6 (3.3) |
| Push-off (BWN) | 1.001 (0.06) | 1.021 (0.06) | -2.6 (5.2) | 1.15 (0.09) | 1.16 (0.08) | -1.5 (1.6) | 0.951,2 (0.07) | 1.001,2 (0.07) | -4.2 (6.0)1,2 | 1.16 (0.12) | 1.17 (0.10) | -0.9 (3.5) |
| Total impulse (BWN/s) | 0.53 (0.05) | 0.57 (0.04) | -5.91 (5.6) | 0.55 (0.05) | 0.55 (0.05) | -0.2 (1.8) | 0.491,2 (0.04) | 0.531,2 (0.04) | -7.1 (6.2)1,2 | 0.46 (0.04) | 0.46 (0.04) | -0.1 (1.6) |
| Weight acceptance impulse (BWN/s) | 0.1041 (0.008) | 0.108 (0.010) | -3.41 (6.3) | 0.112 (0.007) | 0.112 (0.007) | 0.9 (3.1) | 0.1132 (0.014) | 0.1202 (0.015) | -5.1 (6.6)1,2 | 0.146 (0.010) | 0.142 (0.011) | 3.5 (4.2) |
| Push off impulse (BWN/s) | 0.0981 (0.008) | 0.0981 (0.011) | 0.6 (13.4) | 0.111 (0.009) | 0.114 (0.008) | -2.9 (2.6) | 0.0911,2 (0.008) | 0.0981,2(0.007) | -6.6 (8.0)1,2 | 0.110 (0.011) | 0.111 (0.009) | -2.9 (4.7) |
| Step length (cm) | 681 (10) | 671 (9) | 2.6 (6.5) | 79 (6) | 78 (5) | 1.7 (2.5) | 79 (12)2 | 78 (11)2 | 2.4 (6.2) | 99 (8) | 98 (8) | 1.0 (1.9) |
| Step time (s) | 0.53 (0.05) | 0.54 (0.04) | -1.2 (7.5) | 0.53 (0.05) | 0.53 (0.04) | 0.3 (3.1) | 0.481,2 (0.03) | 0.502 (0.05) | -4.0 (6.6)1,2 | 0.44 (.04) | 0.44 (0.04) | -0.2 (3.5) |
| Contact time (s) | 0.72 (0.05) | 0.731 (0.05) | -2.41 (3.8) | 0.68 (0.06) | 0.69 (0.06) | -0.3 (1.7) | 0.651,2 (0.05) | 0.672 (0.07) | -3.4 (3.9)1,2 | 0.56 (0.05) | 0.56 (0.05) | -0.3 (1.5) |
| Single limb stance time (s) | 0.331 (0.04) | 0.36 (0.04) | -7.01 (9.3) | 0.38 (0.04) | 0.38 (0.04) | -0.4 (3.5) | 0.321 (0.02) | 0.341 (0.03) | -7.5 (8.5)1,2 | 0.33 (0.04) | 0.33 (0.03) | -0.3 (3.1) |
The values are indicated as means ± standard deviation;
Significant difference between OA group vs control at PWS (P < 0.05);
Significant difference between OA group vs control at TWS (P < 0.05). PWS: Preferred walking speed; NA: Not available; TWS: Top walking speed; BWN: Body weight normalised; OA: Osteoarthritis.
Figure 2.
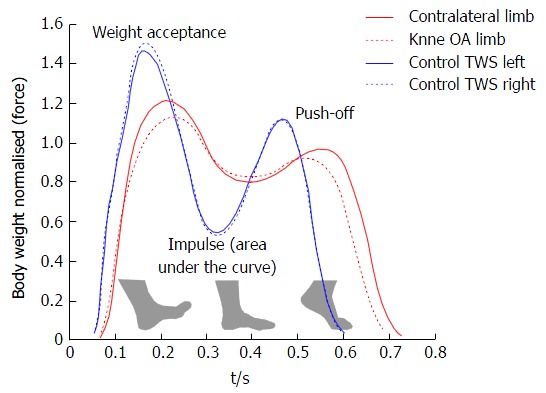
Mean gait patterns during stance phase of controls (blue) and knee osteoarthritis patients (red) at their top walking speed. OA: Osteoarthritis; TWS: Top walking speed.
Figure 3.
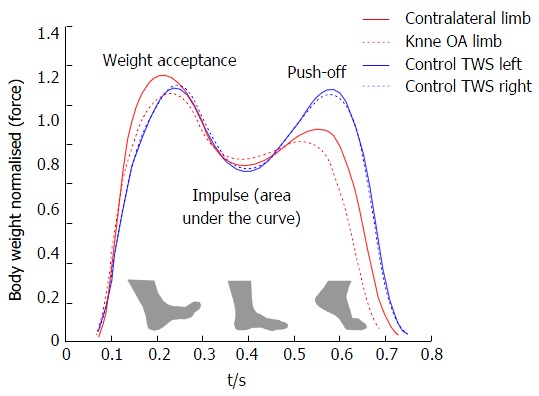
Mean gait patterns during stance phase of controls (blue) and knee osteoarthritis patients (red) at similar speeds. OA: Osteoarthritis; TWS: Top walking speed.
Table 3.
Area under curve results with confidence intervals demonstrating the discriminating ability of different variables
| SR at TWS | AUC | CI | Significance |
| WA | 0.898 | 0.800, 0.996 | < 0.001 |
| PO | 0.683 | 0.521, 0.846 | 0.038 |
| TI | 0.902 | 0.797, 1.000 | < 0.001 |
| WAI | 0.852 | 0.736, 0.968 | < 0.001 |
| POI | 0.654 | 0.491, 0.817 | 0.081 |
| ST | 0.650 | 0.484, 0.816 | 0.090 |
| CT | 0.767 | 0.628, 0.905 | 0.003 |
| SLST | 0.767 | 0.628, 0.906 | 0.003 |
AUC: Area under curve; CI: Confidence intervals; SR: Symmetry ratio; WA: Weight acceptance; PO: Push-off; TI: Total impulse; WAI: Weight acceptance impulse; POI: Push-off impulse; ST: Stance time; CT: Contact time; SLST: Single limb stance time.
Figure 4.
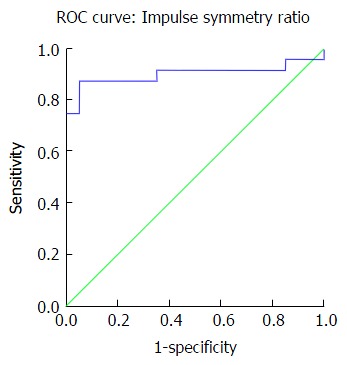
Receiver operating characteristics graph: Displaying the discriminating ability of total impulse symmetry ratio. ROC: Receiver operating characteristics.
DISCUSSION
By analysing gait ground reaction forces and symmetry at top walking speed, this study set-out to determine the changes in gait associated with the general decline in walking speed seen in patients with knee OA. In accordance with previous studies[17,18], compared to healthy controls the OA group walked more slowly and asymmetrically, with a wider based gait, and a shorter step length. Furthermore the study demonstrated that testing at top walking speed elicited differences in gait which would not ordinarily be detected at slower walking speeds.
Of most interest was that the OA patients had a significantly lower, and less symmetrical, push-off force and push-off impulse compared to healthy controls - suggesting a weakness during the terminal stance phase is a factor causing slower walking speeds. This may be secondary to loss of muscle power around the joint, a theory supported by Baert et al[19]’s finding of a 37% decrease in isometric knee extension power in early OA, and a 56% decrease in established OA patients, when compared to a matched control group. This loss may also be due to pain and the progressive attrition of muscle power due to the decreasing activity found in a biomechanically faulty knee. Nevertheless Bytyqi et al[20] demonstrated 11.6 degree loss during knee flexion/extension during comfortable walking in patients with OA when compared to controls which would further explain the importance of power and improved knee kinematics to achieve faster walking speed. This is of clinical value to surgeons and patients alike, given that it reinforces the need for replacement surgery to be combined with physiotherapy aimed at restoring muscle strength and range of motion, and is consistent with the finding that gait and function can improve over time[21].
Another important study finding was the results of weight acceptance and weight acceptance impulse in the knee OA patients. Weight acceptance is the period during early stance phase at which the knee is fully extended and accepting the full weight. Whilst the weight acceptance of the affected limb in knee OA patients was comparable to healthy controls (1.18 vs 1.18 BWN and 0.113 vs 0.112 BWN/s respectively), they were in fact abnormal when compared to the unaffected leg in the same patient (1.18 vs 1.26 BWN and 0.113 vs 0.120 BWN/s). This likely indicates that these patients inherently have loaded their arthritic knee joint beyond than what would be expected at that speed at which now they are limping and trying to reduce load on it. Furthermore considering that the patient’s body mass index (BMI) were 35% higher than the controls, the normalised force results underestimates the true gross force which is traveling through the OA patient’s knee during walking. These findings may partly explain why their knee joints wore out in the first instance. Furthermore they are consistent with a study reporting significantly increased knee joint loads during walking in subjects with knee OA[22]. These observations may be of practical value, as a tool for measuring intervention which aim to retrain gait, avoid high weight acceptance forces and theoretically prevent further joint arthrosis from occurring.
The second main aim of the study was to assess the use of an area (impulse) below ground reaction force peaks, rather than just solitary points on the peak, as a novel method of assessing symmetry. In this regard, after single limb stance time, total impulse and push-off impulse displayed the largest asymmetries in knee OA patients. And ROC analysis identified the total impulse symmetry ratio as the best variable to discriminate between groups, with an AUC of 0.902 which is considered excellent. Weight acceptance impulse also proved to be a good discriminating measure, with an AUC of 0.852. Hodt-Billington recommended a 10% asymmetry criterion for pathological gait from their work comparing hip OA patients with healthy controls[1], whilst our results suggest a symmetry ratio criterion as low as 5% for total impulse. Nevertheless a 10% criterion should generally be recommended for parametric data as recommended by multiple studies[1,23,24]. Our results also demonstrate that healthy gait has a range of asymmetry which is parameter dependent and varies statistically depending on its confidence interval.
The limitation of this study relates to the control group, who were significantly lighter and younger, and walked with a significantly faster top speed. Fortuitously, the control group’s preferred walking speed was similar to the OA group’s top walking speed with identical step length (79 cm vs 79 cm), allowing for a fair and better comparison. Additionally the intended objective was not to determine which group was faster but rather, which factors caused them to be slower. Nevertheless a previous 3-D kinematic gait study looking at knee movements did not observe a difference in fast walking speed in knee OA patients despite them being almost 10 years older than the health controls[25]. And as previously discussed, by looking at asymmetry, in effect patients act as their own controls if they have one healthy, un-affected, knee. In common with many other gait studies, our OA group were significantly heavier than controls, which is unsurprising given that high BMI is a perhaps the greatest known risk factor for OA[5,25]. However, all ground reaction forces were normalised for body weight to minimise the bias introduced by this difference between groups. Lastly this is a cross-sectional study and it would have been interesting to see whether interventions such as physiotherapy, foot orthotics, or knee surgery could restore normal ground reaction forces and symmetry while walking.
In conclusion, this paper reconfirms the gait abnormalities seen with knee OA, but for the first time using ground reaction forces at top walking speed and a novel method of analysis. Reduced push-off and overall loading (impulse) are key factors in limiting the top walking speed of patients with OA. Higher than expected weight acceptance loads are potential causes for patients wearing out their joints. Furthermore OA patients demonstrate significant asymmetry in almost all parameters of gait biomechanics, with ROC analysis identifying total impulse as the variable with the best discriminating ability. Longitudinal studies are required, but these features may be useful in the screening and rehabilitation of patients at risk of developing, or with early knee arthrosis.
COMMENTS
Background
Knee osteoarthritis is an increasingly common condition. Understanding the loading characteristics of patients with knee osteoarthritis may help prevent or delay this condition from occurring.
Research frontiers
The gait assessment of patients with knee osteoarthritis has primarily been completed using slower speed protocols. The use of faster speeds on an instrumented treadmill has allowed us to better understand the loading patterns of patients with knee osteoarthritis.
Innovations and breakthroughs
This study demonstrated that faster speed detected differences which would not be seen at slower speed. Impulse and weight acceptance were the variables with the best discriminating ability.
Applications
Faster walking speed is recommended during gait analysis for patients with knee osteoarthritis.
Terminology
Ground reaction forces are the stance phase loading characteristics of the foot during gait.
Peer-review
This is an interesting paper that aims to evaluate the gait patterns in osteoarthritis patients at top walking speed. This is a well-designed and organized study that uses validated measurements and produces some important findings. The methodology used is appropriate and well presented.
Footnotes
Manuscript source: Invited manuscript
Specialty type: Orthopedics
Country of origin: United Kingdom
Peer-review report classification
Grade A (Excellent): A, A
Grade B (Very good): B
Grade C (Good): 0
Grade D (Fair): D
Grade E (Poor): 0
Institutional review board statement: Ethical approval was sought and gained prior to commencement of the trial through the research ethics committee (10/H0807/101). All investigations were conducted in conformity with ethical principles of research, and informed consent for participation in the study was obtained. This work was performed at, Imperial College London, Charing Cross Campus, United Kingdom.
Conflict-of-interest statement: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Data sharing statement: Extended dataset available from the corresponding author.
Peer-review started: June 17, 2016
First decision: August 16, 2016
Article in press: January 18, 2017
P- Reviewer: Cui Q, Kulshrestha V, Laupattarakasem W, Paschos NK S- Editor: Kong JX L- Editor: A E- Editor: Li D
References
- 1.Hodt-Billington C, Helbostad JL, Vervaat W, Rognsvåg T, Moe-Nilssen R. Criteria of gait asymmetry in patients with hip osteoarthritis. Physiother Theory Pract. 2012;28:134–141. doi: 10.3109/09593985.2011.574783. [DOI] [PubMed] [Google Scholar]
- 2.Patterson KK, Parafianowicz I, Danells CJ, Closson V, Verrier MC, Staines WR, Black SE, McIlroy WE. Gait asymmetry in community-ambulating stroke survivors. Arch Phys Med Rehabil. 2008;89:304–310. doi: 10.1016/j.apmr.2007.08.142. [DOI] [PubMed] [Google Scholar]
- 3.Jørgensen L, Crabtree NJ, Reeve J, Jacobsen BK. Ambulatory level and asymmetrical weight bearing after stroke affects bone loss in the upper and lower part of the femoral neck differently: bone adaptation after decreased mechanical loading. Bone. 2000;27:701–707. doi: 10.1016/s8756-3282(00)00374-4. [DOI] [PubMed] [Google Scholar]
- 4.Bejek Z, Paróczai R, Illyés A, Kiss RM. The influence of walking speed on gait parameters in healthy people and in patients with osteoarthritis. Knee Surg Sports Traumatol Arthrosc. 2006;14:612–622. doi: 10.1007/s00167-005-0005-6. [DOI] [PubMed] [Google Scholar]
- 5.Zeni JA, Higginson JS. Differences in gait parameters between healthy subjects and persons with moderate and severe knee osteoarthritis: a result of altered walking speed? Clin Biomech (Bristol, Avon) 2009;24:372–378. doi: 10.1016/j.clinbiomech.2009.02.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Studenski S, Perera S, Patel K, Rosano C, Faulkner K, Inzitari M, Brach J, Chandler J, Cawthon P, Connor EB, et al. Gait speed and survival in older adults. JAMA. 2011;305:50–58. doi: 10.1001/jama.2010.1923. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tanamas S, Hanna FS, Cicuttini FM, Wluka AE, Berry P, Urquhart DM. Does knee malalignment increase the risk of development and progression of knee osteoarthritis? A systematic review. Arthritis Rheum. 2009;61:459–467. doi: 10.1002/art.24336. [DOI] [PubMed] [Google Scholar]
- 8.Blagojevic M, Jinks C, Jeffery A, Jordan KP. Risk factors for onset of osteoarthritis of the knee in older adults: a systematic review and meta-analysis. Osteoarthritis Cartilage. 2010;18:24–33. doi: 10.1016/j.joca.2009.08.010. [DOI] [PubMed] [Google Scholar]
- 9.Hunt MA, Birmingham TB, Giffin JR, Jenkyn TR. Associations among knee adduction moment, frontal plane ground reaction force, and lever arm during walking in patients with knee osteoarthritis. J Biomech. 2006;39:2213–2220. doi: 10.1016/j.jbiomech.2005.07.002. [DOI] [PubMed] [Google Scholar]
- 10.McCrory JL, White SC, Lifeso RM. Vertical ground reaction forces: objective measures of gait following hip arthroplasty. Gait Posture. 2001;14:104–109. doi: 10.1016/s0966-6362(01)00140-0. [DOI] [PubMed] [Google Scholar]
- 11.KELLGREN JH, LAWRENCE JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. 1957;16:494–502. doi: 10.1136/ard.16.4.494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wiik AV, Manning V, Strachan RK, Amis AA, Cobb JP. Unicompartmental knee arthroplasty enables near normal gait at higher speeds, unlike total knee arthroplasty. J Arthroplasty. 2013;28:176–178. doi: 10.1016/j.arth.2013.07.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hof AL. Scaling gait data to body size. Gait Posture. 1996:222–223. doi: 10.1016/s0966-6362(01)00097-2. [DOI] [PubMed] [Google Scholar]
- 14.Patterson KK, Gage WH, Brooks D, Black SE, McIlroy WE. Evaluation of gait symmetry after stroke: a comparison of current methods and recommendations for standardization. Gait Posture. 2010;31:241–246. doi: 10.1016/j.gaitpost.2009.10.014. [DOI] [PubMed] [Google Scholar]
- 15.Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology. 1982;143:29–36. doi: 10.1148/radiology.143.1.7063747. [DOI] [PubMed] [Google Scholar]
- 16.Astephen Wilson JL. Challenges in dealing with walking speed in knee osteoarthritis gait analyses. Clin Biomech (Bristol, Avon) 2012;27:210–212. doi: 10.1016/j.clinbiomech.2011.09.009. [DOI] [PubMed] [Google Scholar]
- 17.Debi R, Mor A, Segal G, Debbi EM, Cohen MS, Igolnikov I, Bar Ziv Y, Benkovich V, Bernfeld B, Rozen N, et al. Differences in gait pattern parameters between medial and anterior knee pain in patients with osteoarthritis of the knee. Clin Biomech (Bristol, Avon) 2012;27:584–587. doi: 10.1016/j.clinbiomech.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 18.Ornetti P, Maillefert JF, Laroche D, Morisset C, Dougados M, Gossec L. Gait analysis as a quantifiable outcome measure in hip or knee osteoarthritis: a systematic review. Joint Bone Spine. 2010;77:421–425. doi: 10.1016/j.jbspin.2009.12.009. [DOI] [PubMed] [Google Scholar]
- 19.Baert IA, Jonkers I, Staes F, Luyten FP, Truijen S, Verschueren SM. Gait characteristics and lower limb muscle strength in women with early and established knee osteoarthritis. Clin Biomech (Bristol, Avon) 2013;28:40–47. doi: 10.1016/j.clinbiomech.2012.10.007. [DOI] [PubMed] [Google Scholar]
- 20.Bytyqi D, Shabani B, Lustig S, Cheze L, Karahoda Gjurgjeala N, Neyret P. Gait knee kinematic alterations in medial osteoarthritis: three dimensional assessment. Int Orthop. 2014;38:1191–1198. doi: 10.1007/s00264-014-2312-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Taniguchi M, Sawano S, Kugo M, Maegawa S, Kawasaki T, Ichihashi N. Physical Activity Promotes Gait Improvement in Patients With Total Knee Arthroplasty. J Arthroplasty. 2016;31:984–988. doi: 10.1016/j.arth.2015.11.012. [DOI] [PubMed] [Google Scholar]
- 22.Baliunas AJ, Hurwitz DE, Ryals AB, Karrar A, Case JP, Block JA, Andriacchi TP. Increased knee joint loads during walking are present in subjects with knee osteoarthritis. Osteoarthritis Cartilage. 2002;10:573–579. doi: 10.1053/joca.2002.0797. [DOI] [PubMed] [Google Scholar]
- 23.Robinson RO, Herzog W, Nigg BM. Use of force platform variables to quantify the effects of chiropractic manipulation on gait symmetry. J Manipulative Physiol Ther. 1987;10:172–176. [PubMed] [Google Scholar]
- 24.Balasubramanian CK, Bowden MG, Neptune RR, Kautz SA. Relationship between step length asymmetry and walking performance in subjects with chronic hemiparesis. Arch Phys Med Rehabil. 2007;88:43–49. doi: 10.1016/j.apmr.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 25.Landry SC, McKean KA, Hubley-Kozey CL, Stanish WD, Deluzio KJ. Knee biomechanics of moderate OA patients measured during gait at a self-selected and fast walking speed. J Biomech. 2007;40:1754–1761. doi: 10.1016/j.jbiomech.2006.08.010. [DOI] [PubMed] [Google Scholar]