

In unexplained collapse, the possibility of carbon monoxide poisoning must not be neglected.
CASE HISTORY
A man of 40 was admitted having collapsed. His only medical history was treatment for depression. Examination was unremarkable except for complete short-term memory loss to such an extent that he was unable to recall his address. Blood tests and electrocardiography were normal. CT and MRI (Figures 1 and 2) revealed symmetrical lesions in the globus pallidus and posterior putamen. There were also ill-defined lesions in the posterior periventricular white matter. The following day the patient's neighbour reported finding a hosepipe attached to his car's exhaust pipe.
Figure 1.

CT of brain
Figure 2.
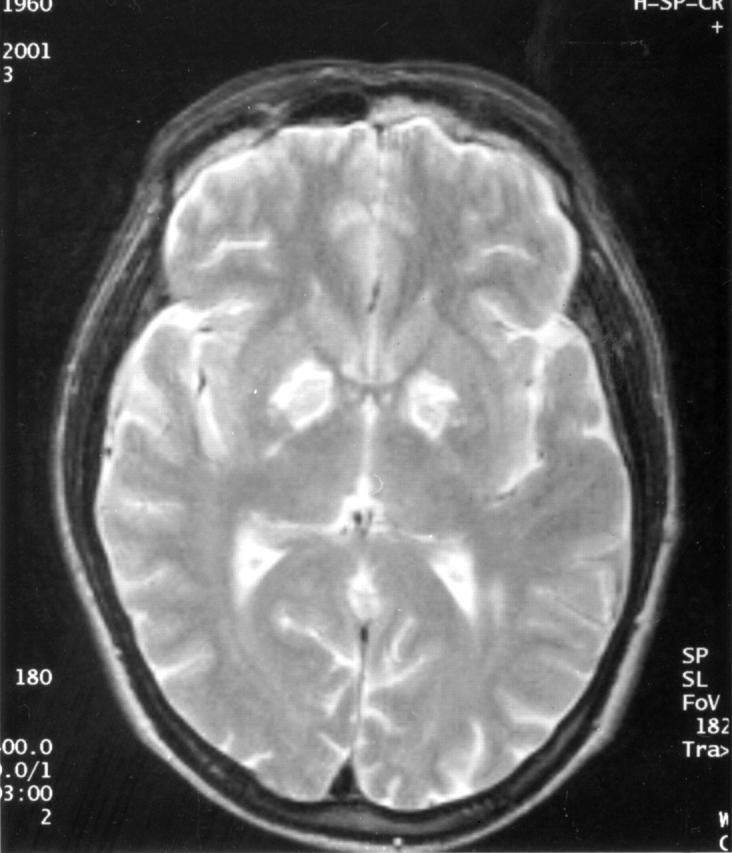
MRI of brain
The radiological findings are characteristic of carbon monoxide poisoning. The patient was referred for hyperbaric oxygen therapy. The results of psychometric testing improved but he was left with defects that limited his everyday function.
Box 1 Differential diagnosis of the CT and MRI appearances in carbon monoxide poisoning
Vascular
Lacunar infarcts
Late-stage hypertensive haemorrhage
Hypoxic injury
Toxic
Carbon monoxide poisoning
Methanol poisoning
Cyanide poisoning
Manganese poisoning
Metabolic
Mitochondrial cytopathies
Wilson's disease
Hallervorden–Spatz disease
Neurodegenerative
Acquired hepatocerebral degeneration
Physiological
Giant perivascular spaces
Age-related iron deposition
Infective
Acute disseminated encephalomyelitis
Acute bilateral striatal necrosis
Congenital
Neurocutaneous syndrome: neurofibromatosis type 1.
COMMENT
Carbon monoxide poisoning is responsible for about 50 deaths and up to 200 severe injuries a year in England.1 Most cases are accidental. Signs and symptoms of poisoning depend upon exposure, and range from those of a non-specific viral illness to arrhythmias, coma and death.2 The classic cherry-red lips, cyanosis and retinal haemorrhages rarely occur. Diagnosis is by measurement of carboxyhaemoglobin, although there is poor correlation between severity of symptoms and concentration of carboxyhaemoglobin. Patients may present for imaging studies with unexplained loss of consciousness or neurological abnormalities where carbon monoxide is not initially suspected. The differential diagnosis of the CT and MRI appearances is summarized in Box 1.
Treatment requires oxygen to shorten the half-life of carboxyhaemoglobin. A recent double-blind randomized trial demonstrated a reduced incidence of cognitive sequelae at six weeks in patients treated with hyperbaric oxygen,3 though the optimum number of sessions and the maximum time to therapy were not established.
References
- 1.Walker E, Hay A. Carbon monoxide poisoning is still an under recognised problem. BMJ 1999;319: 1082-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ernst A, Zibrak JD. Carbon monoxide poisoning. N Engl J Med 1998;339: 1603-8 [DOI] [PubMed] [Google Scholar]
- 3.Weaver LK, Hopkins RO, Chan KJ, et al. Hyperbaric oxygen for acute carbon monoxide poisoning. N Engl J Med 2002;347: 1057-67 [DOI] [PubMed] [Google Scholar]