

Abstract
Menthol is a vasoactive compound that is widely used in topical analgesic agents. Menthol induces cutaneous vasodilation, however the underlying mechanisms are unknown. Determining the rates of appearance and clearance of menthol in the skin is important for optimizing topical treatment formulation and dosing. The purpose of this study was to determine the mechanisms contributing to menthol-mediated cutaneous vasodilation and to establish a time course for menthol appearance/clearance in the skin. Ten young (23±1 years, 5 males 5 females) subjects participated in two protocols. In study 1, four intradermal microdialysis fibers were perfused with increasing doses of menthol (0.1-500mM) and inhibitors for nitric oxide (NO), endothelium derived hyperpolarizing factors (EDHFs), and sensory nerves. Skin blood flow was measured with laser Doppler flowmetry and normalized to %CVCmax. In study 2, two intradermal microdialysis fibers were perfused with lactated Ringer's solution. 0.017mL•cm-2 of a 4% menthol gel was placed over each fiber. 5μL samples of dialysate from the microdialysis fibers were collected every 30 minutes and analyzed for the presence of menthol with high performance gas chromatography/mass spectrometry. Skin blood flow (laser speckle contrast imaging) and subjective ratings of menthol sensation were simultaneously obtained with dialysate samples. In study 1, menthol induced cutaneous vasodilation at all doses ≥100mM (all p<0.05). However, inhibition of either NO, EDHFs, or sensory nerves fully inhibited menthol-mediated vasodilation (all p>0.05). In study 2, significant menthol was detected in dialysate 30 minutes post menthol application (0.89ng, p=0.0002). Relative to baseline, cutaneous vasodilation was elevated from minutes 15-45 and ratings of menthol sensation were elevated from minute 5-60 post menthol application (all p<0.05). Menthol induces cutaneous vasodilation in the skin through multiple vasodilator pathways, including NO, EDHF, and sensory nerves. Topical menthol is detectable in the skin within 30 minutes and is cleared by 60 minutes. Skin blood flow and perceptual measures follow a similar time course as menthol appearance/clearance.
Keywords: Menthol, TRPM8, microdialysis, cutaneous, microvasculature, gas chromatography
Introduction
Menthol is the active ingredient in many topical analgesic agents that elicits a cold sensation by acting on transient receptor potential melastatin 8 (TRPM8) channels (Peier et al., 2002). Because of its wide ranging use in topical products, it is important to understand how menthol is penetrating the skin and affecting blood flow and sensation. Utilizing laser speckle contrast imaging, we recently demonstrated the topically applied menthol gel induces vasodilation of the cutaneous microvasculature (Craighead and Alexander, 2016).
TRPM8 channels are expressed in vascular endothelium (Johnson et al., 2009) and smooth muscle (Yang et al., 2006). The literature on the vasoactive effects of menthol is varied, with most (Cheang et al., 2013; Craighead and Alexander, 2016; Johnson et al., 2009; Sun et al., 2014) but not all (Olive et al., 2010; Topp et al., 2013; Topp et al., 2011) studies finding that menthol possess vasorelaxent properties. However, there is not a consensus on the mechanism(s) through which menthol mediates vasodilation. There is evidence that menthol acts through nitric oxide (NO)(Johnson et al., 2009), RhoA/Rho kinase (Sun et al., 2014), and by altering smooth muscle calcium concentration (Cheang et al., 2013; Ito et al., 2008). The disparate findings may be due to the use of different animal models and vascular beds. Because of menthol's presence in many topical agents, the human cutaneous circulation is a clinically relevant vascular bed in which to examine the vasoactive effects of menthol.
Utilizing reactive hyperemia and local heating to assess endothelium derived hyperpolarizing factor (EDHF)/sensory nerve and NO-dependent vasodilation respectively, we recently found that menthol likely caused vasodilation through EDHFs and sensory nerves (Craighead and Alexander, 2016). However, a ceiling effect of cutaneous vasodilation with local heating may have masked any contribution from NO to menthol-mediated vasodilation. Furthermore, while reactive hyperemia and local heating in the skin are in large part pathway specific, there is a certain degree of cross talk from multiple vasodilator pathways (Brunt and Minson, 2012; Engelke et al., 1996; Medow et al., 2007). Consequently, the mechanism(s) contributing to menthol-mediated vasodilation need to be more fully elucidated.
From a therapeutic standpoint, topical menthol containing products are used in clinical populations (i.e. arthritis, muscle strain, back pain) for their effects of sensation and pain relief. Along with elucidating menthol's mechanism(s) of action, determining the amount of menthol delivered to the cutaneous tissue and the rate of menthol appearance/clearance is important for optimizing formulation of topical menthol containing products for improving its analgesic effects.
The goals of this study were to use intradermal microdialysis, to (1) pharmacodissect the mechanism(s) through which menthol induces cutaneous vasodilation, and (2) determine a time course for menthol appearance and clearance in the cutaneous tissue following topical menthol application. We hypothesized that NO, EDHFs, and sensory nerves would all contribute to menthol-mediated vasodilation. We also hypothesized that menthol would be detectable in dialysate samples from the cutaneous tissue within 30 minutes on topical exposure and remain present throughout the duration of our protocol.
Methods
Experimental protocols were approved by the institutional review board of The Pennsylvania State University and conformed to the Declaration of Helsinki. Voluntary verbal and written consent were obtained from all subjects prior to participation in the study. Protocols were carried out in a group of 10 young, healthy, participants who did not smoke, were not pregnant or breastfeeding, and were free from any apparent cardiovascular disease. Women not taking birth control were tested during the early follicular phase, while women on oral birth control were tested during the placebo phase of their medication. Participants were free of any other medications that are known to alter vascular function.
Study 1: Menthol dose-response
All experiments took place in a thermoneutral laboratory with subjects in a semi-supine position. Subjects did not exercise, or consume caffeine or alcohol, for 12 hours before the experiment. Four intradermal microdialysis fibers (CMA Microdialysis; 55 kDa cutoff) were placed in the skin of the ventral forearm as previously described (Smith et al., 2011; Stanhewicz et al., 2012). After placement of microdialysis fibers, 60-90 minutes was given for full resolution of hyperemia due to insertion trauma.
After resolution of fiber placement hyperemia, each microdialysis site was randomly assigned either 1) control (lactated Ringer's solution), 2) 20mM NG-Nitro-L-arginine methyl ester (L-NAME), a non-selective NO synthase (NOS) antagonist to assess NO-dependent vasodilation, 3) 50mM tetraethylammonium (TEA), a potassium channel blocker to determine the contribution of EDHFs or 4) Lidocaine (4% LMX4 cream applied for 60 min) over a microdialysis site perfused with lactated Ringer's to inhibit sensory nerves. L-NAME and TEA were mixed with lactated Ringer's right before use and filtered through a syringe microfilter (Acrodisc; 0.2μm filter). Drugs were perfused with microperfusion pumps (BASi Bee Hive controller and Baby Bee syringe drive) set at a rate of 2μL•min-1. Sensory nerve blockade was confirmed through lack of sensation to a needle prick (Minson et al., 2001; Wong, 2013).
After full abatement of insertion trauma, local heating units were placed over each microdialysis site and set to 33°C to maintain thermoneutral skin temperature. Laser Doppler flowmeter probes (Moor Instruments) were placed over each local heating unit to continually measure red cell flux. Measurement of skin blood flow with laser Doppler flowmetry is highly reproducible when the data are expressed as a percentage of maximum vasodilation (Tew et al., 2011). Data were sampled at 40Hz with WinDaq data acquisition software (DATAQ Instruments). Blood pressure was measured every five minutes via brachial auscultation (CardioCap5, General Electric). Baseline laser Doppler flux was measured for approximately 15 minutes, after which the menthol dose-response commenced. Seven increasing doses of menthol (99% Menthol, Sigma-Aldrich) (0.1, 1, 10, 50, 100, 250, and 500mM) were perfused through each microdialysis fiber in 5 minute increments. Menthol was mixed with lactated Ringer's and the matching pharmacological inhibitor when appropriate. 500mM menthol was chosen as the maximum dose as it represented the most menthol that could dissolve in lactated Ringer's when utilizing a hot plate and a stir bar. Menthol's solubility could have been increased with the addition of ethanol to the solution, however we elected not include ethanol because of its inhibitory effect on TRPM8 channels (Benedikt et al., 2007).
Following completion of the menthol dose response, 28mM sodium nitroprusside (SNP), was perfused through the fibers at a rate of 4μL•min-1 and the temperature of the local heaters was raised to 43°C to elicit maximum vasodilation (Holowatz et al., 2005; Smith et al., 2011).
Data were stored offline for later analysis. Red cell flux was normalized to cutaneous vascular conductance (CVC: flux•mean arterial pressure-1) and expressed as a percentage of site specific maximum obtained from SNP/43°C heat (%CVCmax). All data were analyzed with GraphPad Prism 6 software. A 2-way ANOVA was run to detect menthol dose-site interactions. Tukey's multiple comparisons tests were conducted where appropriate. Significance was set a priori at α=0.05. An a priori power analysis revealed that 10 subjects was sufficient to detect a meaningful physiological difference of 10% between microdialysis treatment sites with a standard deviation of the difference of 10%, with a desired power of 0.8. Effect size (Cohen's d) was calculated for main effects of treatment in study 1. The interpretation of effect size follows the convention of Cohen: 0.2, 0.5, 0.8 correspond to “small,” “medium,” and “large” effect sizes respectively (Cohen, 1988).
Study 2: Menthol dialysate recovery
All experiments took place under the same conditions as in study 1. Two microdialysis fibers were placed in the skin of the ventral forearm. Thirty minutes after placement of fibers and resolution of the insertion hyperemia, a 60cm2 (15cm•4cm) area on the ventral forearm was marked. This marked area included the intradermal portions of the microdialysis fibers. Skin blood flow over this area was measured for 5 minutes with a sample rate of 0.25 Hz utilizing a laser speckle contrast imager (Full-field Laser Perfusion Imager, Moor Instruments). Laser speckle contrast imaging measures provides a relative measure of skin blood flow that is reproducible and possesses good spatial and temporal resolution (Roustit and Cracowski, 2012; Roustit et al., 2010). Dialysate samples from outflow end of the microdialysis fibers were simultaneously collected in 300 μL glass vials with Teflon coated caps. Microperfusion pumps were set at a rate of 1 μL•min-1 to collect 5μL of dialysate. After collection of baseline skin blood flowand dialysate samples was completed, the microperfusion pumps were turned off and skin blood flow measurements were paused. One mL of 4% menthol gel (Biofreeze®) was applied evenly over the 60cm2 area by a researcher with a gloved hand. A clear plastic covering was placed over the menthol to prevent evaporation and measurement of skin blood flow was resumed.
Topical menthol was left in place for 30 minutes. Subjective rating of menthol sensation was obtained from the subjects 5, 10, 15, and 30 minutes after menthol had been applied. The sensation scale was a 0 to 10 visual analog scale with 0 representing no sensation of menthol and 10 a “very intense” sensation.
After 30 minutes, the plastic covering was removed and excess menthol containing gel was wiped away using a sterile piece of gauze. Dialysate samples and menthol sensation were collected as during baseline and were repeated every 30 minutes for 240 more minutes (270 total experiment time). Laser speckle contrast perfusion imaging was measured continuously throughout the protocol. After completion of the protocol dialysate samples were stored at -80°C for later analysis.
To prepare the dialysate samples for menthol detection by gas chromatograph, menthol was extracted from the Ringer's solution by liquid-liquid extraction into dichloromethane. 2-nonanol was used as in internal standard to control for extraction efficiency by adding 20μL of aqueous 250pg•μL-1 2-nonanol to each dialysate. Undecane was used as a second internal standard to control for variation in sample concentration caused by in-vial solvent evaporation. 50μL of dichloromethane containing 2ng•μL-1 undecane was added to each dialysate and vials were vortexed vigorously for 30 seconds. Partitioning was facilitated by centrifuging vials for 5 minutes at 600×g and organic phase was carefully transferred to a gas chromatograph vial.
All samples were analyzed with a gas chromatograph-flame ionization detector (GC-FID) using an Agilent 6890 chromatograph (Agilent Technologies, Santa Clara, CA) equipped with a SPB-35 bonded phase capillary column (0.25 mm × 0.25 μm × 30 m; Supelco, Bellefonte, PA, USA). Injections of 1uL were performed in splitless mode with a split delay of 0.75 min and helium carrier gas flow of 0.8 mL•min-1. The oven was kept at an initial temperature of 40°C for one minute then increased to 200°C at a rate of 15°C•min-1. Inlet and FID temperatures were 220°C and 250°C respectively. Confirmation of menthol recovery was confirmed using an authentic standard as well as by analysis of selected samples by gas chromatography-mass spectrometry (GC-MS) using an Agilent 6890 GC interfaced with an Agilent 5973 mass selective detector operated in electron impact (EI) mode. Parameters were identical to those of the GC-FID and standard EI settings (ion source: 230°C, quadrupole: 150°C, and fragmentation at 70eV) were used to generate spectra matching the NIST 08 reference spectra. Concentrations of menthol, 2-nonanol, and undecane were calculated from their respective FID peak areas in conjunction with external calibration curves and were used to determine total menthol recovery in nanograms.
Skin blood flow data were stored offline for later analysis. Red cell flux was normalized to CVC. All data were analyzed with GraphPad Prism 6 software. One-way ANOVAs were run to detect CVC-time, sensation-time, and menthol recovery-time interactions. Tukey's multiple comparisons tests were conducted where appropriate. Significance was set a priori at α=0.05.
Results
Subject characteristics are presented in table 1. All 10 young, healthy participants completed both study 1 and 2.
Table 1. Subject characteristics.
All subjects were young, apparently healthy, and did not present with any chronic diseases.
| Sex (M,F) | Age (y) | Height (m) | Weight (kg) | BMI (kg•m-2) | SBP (mmHg) | DBP (mmHg) | Total Chol. (mg•dL-1) |
|---|---|---|---|---|---|---|---|
| 5,5 | 23 ± 1 | 1.72 ± 0.02 | 71.3 ± 3.4 | 24.2 ± 1.3 | 116 ± 4 | 69 ± 4 | 158 ± 8 |
Data from the menthol dose response are displayed in figure 1. In the control site, menthol induced significant vasodilation compared to baseline at all concentrations ≥100mM menthol (all p<0.05). In all three treatment sites, CVC was attenuated compared to the control site. Specifically, vasodilation at the L-NAME and lidocaine sites was attenuated compared to control at all menthol doses ≥100mM (all p<0.05). Vasodilation at the TEA site was attenuated compared to control at all menthol doses ≥50mM (all p<0.05). Each inhibitor (L-NAME, TEA, lidocaine) fully blocked menthol-mediated vasodilation. At no dose of menthol was vasodilation with any inhibitor significantly increased compared to baseline (all p>0.05). There were no differences between the three inhibitors. The effect size between our control site and our treatment sites was large (effect size=1).
Figure 1. Menthol dose response.
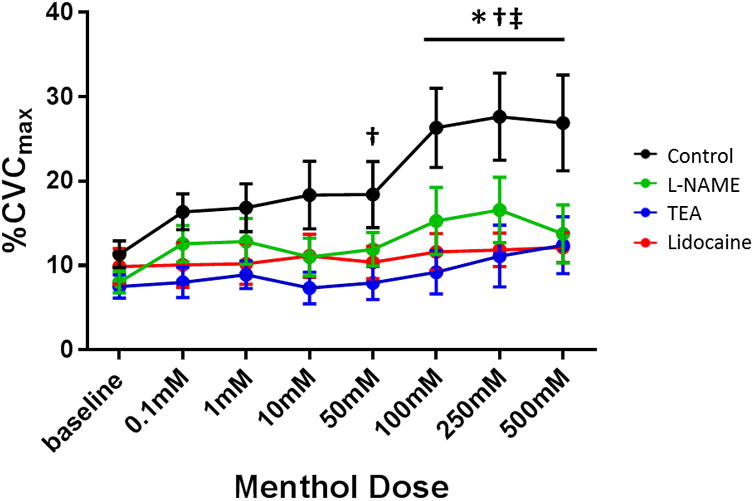
Menthol elicited increased vasodilation at all concentrations ≥100 mM. Antagonism with any of L-NAME, TEA, or lidocaine prevented vasodilation. The control site exhibited significantly more vasodilation than the TEA site at all menthol doses ≥50mM and more than the L-NAME and lidocaine sites at all menthol doses ≥100mM. * p<0.05 between control and L-NAME, † p<0.05 between control and TEA, ‡ p<0.05 between control and lidocaine.
Self-reported sensation of menthol over time is shown in figure 2A. There was a significant report of menthol sensation from minute 5 to minute 60-post menthol application (all p<0.05), after which the reported menthol sensation was different compared to baseline. Figure 2B. illustrates absolute CVC over time during the topical menthol experiment. Compared to baseline, menthol application induced cutaneous vasodilation measured at minute 15 and remained elevated through minute 45 (all p<0.05), however by minute 60 CVC returned to baseline (p=0.08). The concentration of menthol recovered from dialysate is depicted in figure 2C. Compared to menthol-free baseline samples, menthol was detected at the 30 minute time point (0.89 ng, p=0.0002). Trace amounts of menthol were detected at each subsequent measurement, however none of these measures reached statistical significance (all p>0.05).
Figure 2. Perceptual and physiological responses to topical menthol.
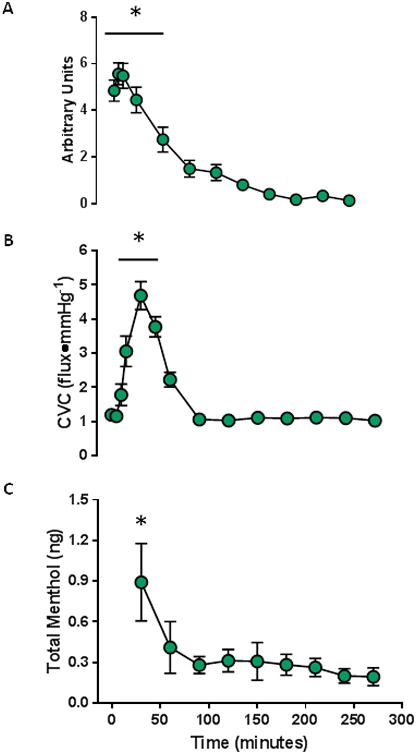
(A) Self-reported sensation from topical menthol was significant at every time point between minute 5 and minute 60 post menthol application. (B) Topical menthol significantly increased vasodilation by 15 minutes post-application. Vasodilation remained elevated relative to baseline through minute 45 post-application. (C) Menthol collected from dialysate (ng). Significant menthol was detected at 30 minutes post menthol application. Menthol detection was statistically insignificant at every following time point. * p<0.05 compared to baseline.
Discussion
The main findings from this study were that (1) menthol increases cutaneous microvascular blood flow in a dose-dependent manner, (2) full expression of menthol mediated-vasodilation is dependent on NO, EDHFs, and sensory nerves, and (3) menthol from the application of a topical analgesic is detectable in dialysate from intradermal microdialysis fibers 30 minutes post-menthol application.
We have recently reported that menthol induces cutaneous vasodilation through EDHF and sensory nerve pathways. In that study we used the physiological stimuli reactive hyperemia and local heating to induce NO- and EDHF/sensory nerve-dependent vasodilation, respectively (Craighead and Alexander, 2016). We concluded that EDHFs and sensory nerves contribute to menthol-mediated vasodilation, but our findings in regard to NO were inconclusive.
In the present study we utilized specific pharmacological inhibitors of NOS, vascular smooth muscle potassium channels, and sensory nerves. We found that NO, EDHFs, and sensory nerves all play a role in menthol-mediated vasodilation as inhibition of any individual pathway attenuated menthol-induced cutaneous vasodilation.
Our finding that menthol-mediated dilation through multiple mechanisms is not surprising given the physiology of TRPM8 channels. When activated, TRPM8 channels allow the non-selective flow of cations, including calcium, into the cell. Entrance of calcium into endothelial cells through vascular TRPM8 channels has the potential to upregulate both NO and EDHFs. Increased calcium in the endothelium increases NO production by binding to calmodulin and subsequently activating NOS which then catalyzes the formation of NO from the substrate L-arginine (Cohen and Vanhoutte, 1995; Forstermann et al., 1991; Kuchan and Frangos, 1994). In our study, we utilized L-NAME to competitively inhibit NOS, and thus NO synthesis, and found that menthol-mediated vasodilation was significantly attenuated.
Calcium entry into the endothelium can also induce downstream activation of intermediate and small conductance calcium activated potassium channels. Activation of these potassium channels induces hyperpolarization that is propagated to the vascular smooth muscle cells via myoendothelial gap junctions. The resulting hyperpolarization relaxes the vascular smooth muscle and leads to vasodilation (Feletou and Vanhoutte, 2009; Ungvari et al., 2002). That TEA inhibited menthol-mediated vasodilation suggests that opening of calcium-activated potassium channels is requisite for menthol-induced vasodilation.
That inhibition of either NO- or EDHF-mediated vasodilation fully attenuated menthol-induced cutaneous vasodilation suggests that there is cross-talk between these two pathways. Cross-talk between these two pathways has been shown to occur in the cutaneous microvasculature, albeit in response to reflex vasodilation (Brunt et al., 2013) and sodium sulfide (Kutz et al., 2015). The mechanism that would like NO and EDHF-dependent vasodilation with regards to menthol is not readily apparent and will require further elucidation.
Topical lidocaine mayabolish menthol-mediated vasodilation by preventing the opening of TRPM8 channels (Leffler et al., 2011), or lidocaine-mediated inhibition of sodium channels may shift the cation flux across TRPM8 to a higher sodium, lower calcium balance, reducing the stimulus for NO and EDHF-mediated vasodilation.
Due to the cold sensation it elicits, menthol is commonly used in place of ice cryotherapy with the belief that it induces vasoconstriction. The data in this study add to a large body of literature that implicates menthol as a vasodilator. These counterintuitive findings are most likely due to the expression of TRPM8 receptors in sensory nerves (Dhaka et al., 2008) and the vasculature (Johnson et al., 2009; Yang et al., 2006). It is likely that activation of TRPM8 channels on sensory nerves elicits cool sensations, while vascular TRPM8 receptors mediate vasodilation.
The second aim of this study was to simultaneously measure the perception of the coolness sensation induced by menthol, vasodilation, and appearance/clearance over time. Our results demonstrate that all three of these factors operate along a similar time course. Elevated concentrations of menthol were measured in the dialysate only 30 minutes after application, whereas vasodilation and sensation persisted for 45 and 60 minutes, respectively. Based on these results, it seems likely that the effects of menthol cease soon after it is cleared from the tissue. Menthol was detected (but not statistically different from baseline) in every sample from timepoints 60 to 270 minutes. At these later time points menthol was detected in very low concentrations and is more likely due to trace contaminants or noise and was of little physiological consequence, as evidenced by the return of perception and vascular tone to basal values. It is likely that most of menthol was cleared during this time and that any remaining menthol was below the threshold of TRPM8 channel activation. For all practical purposes, menthol was cleared from the skin after the 30 minute measurement and all other measurements of menthol in dialysate represent full clearance.
These data help to further characterize the effects of menthol on skin blood flow by utilizing pharmacological techniques to elucidating the vasoactive mechanisms of action and determining a time course for various characteristics of topical menthol treatment. Menthol based topical analgesics in the form of creams and gels are applied directly to the skin. Thus, investigating vasoactive and sensory mechanisms of menthol in the skin are important for improving their therapeutic uses. In addition to the mechanistic characterization of the vasoactive properties of menthol we also measured menthol from dialysate samples after topical application of a commonly used menthol based gel. It is technically very challenging to collect and analyze such small volumes and low concentration of menthol. This is a surrogate and most direct measure to date of the menthol concentration within cutaneous tissue. Future work utilizing this analytical technique could be used to examine relative delivery and clearance of different compounds in the skin (i.e. agents with different menthol concentrations or release mechanisms).
Limitations
One limitation of this study was that we were limited in concentration of menthol we could perfuse through microdialysis fibers due to menthol's limited solubility in aqueous solution. While solubility of menthol could have been improved by dissolving it in a 10% ethanol solution, ethanol has been shown to inhibit TRPM8 (Benedikt et al., 2007), which would have altered the results. Therefore, we chose not to utilize ethanol in our experimental approach. DMSO may be a more appropriate solvent for use with menthol, though we did not utilize it in this study. Consequently, we observed relatively small changes in vasodilation when delivering menthol through intradermal microdialysis fibers compared to what we observed from topical menthol application. Despite these differences, our findings were very consistent with our previous findings (Craighead and Alexander, 2016).
A second limitation is that we did not measure TRPM8 activation. Though menthol is considered a TRPM8 specific agonist, it does have cross talk with TRPV3 channels, especially at higher concentrations (Macpherson et al., 2006). TRPV3 channels are capable of inducing vasodilation (Murphy et al., 2016; Pires et al., 2015). Therefore, our skin blood flow findings, especially at higher menthol concentrations, may be due in part to TRPV3 receptor co-activation. Uncovering the contribution of different TRP channels to menthol-mediated vasodilation require further investigation.
Importantly, the population for this study consisted of young, healthy participants free of any chronic disease. These findings may not apply to aged men and women or populations with cardiovascular disease risk factors (i.e. hypertension, hypercholesterolemia) that express decrements in cutaneous microvascular function (Carberry et al., 1992; Holowatz et al., 2011; Holowatz et al., 2010)
Finally, our measurement of menthol in dialysate possesses a lot of inherent variability. Topical menthol is first diluted in the cutaneous tissue, and then passively diffuses into the lactated Ringer's solution perfusing the intradermal microdialysis fibers. Technical issues such as the depth of microdialysis fiber insertion or volume of dialysate collected likely contributed to this variability. Furthermore, the small amounts of menthol measured from minute 60-270 could be due to (1) incomplete clearance of menthol from the microdialysis fiber between measurements and not necessarily from menthol diffusing from the cutaneous tissue at these time points, or (2) trace contaminants or noise from the detection method. None the less, we were able to demonstrate that menthol is detectable shortly after topical menthol application and that the pattern of menthol appearance and disappearance in the skin follows a similar patter as menthol's effect on skin blood flow.
Conclusion
By using specific pharmacological inhibitors, we confirmed our previous finding that menthol induces vasodilation through EDHFs and sensory nerves. We also found that menthol induces NO-dependent vasodilation at thermoneutral skin temperatures. Additionally, we characterized the time course of perception, vasodilation, and appearance/clearance for topical menthol. Menthol peaks in the skin after 30 minutes, the vasoactive effects are apparent after 15 minutes and disappear after 45 minutes, while the sensation of menthol begins rapidly and persists for an hour post application.
Acknowledgments
The authors would like to acknowledge all the research subjects for their time and effort donated towards this study. We would also like to thank Sean Shank, Tom Heinbockel, Ashlee Snyder, and Megan Clarke for their assistance with data collection.
Abbreviations
- CVC
cutaneous vascular conductance
- %CVCmax
percentage of maximum cutaneous vascular conductance
- EDHF
endothelium derived hyperpolarizing factor
- L-NAME
NG-Nitro-L-arginine methyl ester
- NO
nitric oxide
- SNP
sodium nitroprusside
- TRPV3
transient receptor potential vanilloid 3
- TRPM8
transient receptor potential melastatin 8
- TEA
tetraethylammonium
References
- Benedikt J, et al. Ethanol inhibits cold-menthol receptor TRPM8 by modulating its interaction with membrane phosphatidylinositol 4,5-bisphosphate. J Neurochem. 2007;100:211–24. doi: 10.1111/j.1471-4159.2006.04192.x. [DOI] [PubMed] [Google Scholar]
- Brunt VE, et al. No independent, but an interactive, role of calcium-activated potassium channels in human cutaneous active vasodilation. J Appl Physiol (1985) 2013;115:1290–6. doi: 10.1152/japplphysiol.00358.2013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brunt VE, Minson CT. KCa channels and epoxyeicosatrienoic acids: major contributors to thermal hyperaemia in human skin. J Physiol. 2012;590:3523–34. doi: 10.1113/jphysiol.2012.236398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carberry PA, et al. Resting and maximal forearm skin blood flows are reduced in hypertension. Hypertension. 1992;20:349–55. doi: 10.1161/01.hyp.20.3.349. [DOI] [PubMed] [Google Scholar]
- Cheang WS, et al. Menthol relaxes rat aortae, mesenteric and coronary arteries by inhibiting calcium influx. Eur J Pharmacol. 2013;702:79–84. doi: 10.1016/j.ejphar.2013.01.028. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. L. Erlbaum Associates; Hillsdale, N.J: 1988. [Google Scholar]
- Cohen RA, Vanhoutte PM. Endothelium-dependent hyperpolarization. Beyond nitric oxide and cyclic GMP. Circulation. 1995;92:3337–49. doi: 10.1161/01.cir.92.11.3337. [DOI] [PubMed] [Google Scholar]
- Craighead DH, Alexander LM. Topical menthol increases cutaneous blood flow. Microvasc Res. 2016;107:39–45. doi: 10.1016/j.mvr.2016.04.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dhaka A, et al. Visualizing cold spots: TRPM8-expressing sensory neurons and their projections. J Neurosci. 2008;28:566–75. doi: 10.1523/JNEUROSCI.3976-07.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engelke KA, et al. Contribution of nitric oxide and prostaglandins to reactive hyperemia in human forearm. J Appl Physiol (1985) 1996;81:1807–14. doi: 10.1152/jappl.1996.81.4.1807. [DOI] [PubMed] [Google Scholar]
- Feletou M, Vanhoutte PM. EDHF: an update. Clin Sci (Lond) 2009;117:139–55. doi: 10.1042/CS20090096. [DOI] [PubMed] [Google Scholar]
- Forstermann U, et al. Calmodulin-dependent endothelium-derived relaxing factor/nitric oxide synthase activity is present in the particulate and cytosolic fractions of bovine aortic endothelial cells. Proc Natl Acad Sci U S A. 1991;88:1788–92. doi: 10.1073/pnas.88.5.1788. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holowatz LA, et al. Oral atorvastatin therapy restores cutaneous microvascular function by decreasing arginase activity in hypercholesterolaemic humans. J Physiol. 2011;589:2093–103. doi: 10.1113/jphysiol.2010.203935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holowatz LA, et al. Aging and the control of human skin blood flow. Front Biosci (Landmark Ed) 2010;15:718–39. doi: 10.2741/3642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holowatz LA, et al. Mechanisms of acetylcholine-mediated vasodilatation in young and aged human skin. J Physiol. 2005;563:965–73. doi: 10.1113/jphysiol.2004.080952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ito S, et al. Inhibition by the cold receptor agonists menthol and icilin of airway smooth muscle contraction. Pulm Pharmacol Ther. 2008;21:812–7. doi: 10.1016/j.pupt.2008.07.001. [DOI] [PubMed] [Google Scholar]
- Johnson CD, et al. Transient receptor potential melastatin 8 channel involvement in the regulation of vascular tone. Am J Physiol Heart Circ Physiol. 2009;296:H1868–77. doi: 10.1152/ajpheart.01112.2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson JM, et al. Effect of local warming on forearm reactive hyperaemia. Clin Physiol. 1986;6:337–46. doi: 10.1111/j.1475-097x.1986.tb00239.x. [DOI] [PubMed] [Google Scholar]
- Kuchan MJ, Frangos JA. Role of calcium and calmodulin in flow-induced nitric oxide production in endothelial cells. Am J Physiol. 1994;266:C628–36. doi: 10.1152/ajpcell.1994.266.3.C628. [DOI] [PubMed] [Google Scholar]
- Kutz JL, et al. Evidence for a functional vasodilatatory role for hydrogen sulphide in the human cutaneous microvasculature. J Physiol. 2015;593:2121–9. doi: 10.1113/JP270054. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leffler A, et al. Activation of TRPA1 by membrane permeable local anesthetics. Mol Pain. 2011;7:62. doi: 10.1186/1744-8069-7-62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macpherson LJ, et al. More than cool: promiscuous relationships of menthol and other sensory compounds. Mol Cell Neurosci. 2006;32:335–43. doi: 10.1016/j.mcn.2006.05.005. [DOI] [PubMed] [Google Scholar]
- Medow MS, et al. Cyclooxygenase and nitric oxide synthase dependence of cutaneous reactive hyperemia in humans. Am J Physiol Heart Circ Physiol. 2007;293:H425–32. doi: 10.1152/ajpheart.01217.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Minson CT, et al. Nitric oxide and neurally mediated regulation of skin blood flow during local heating. J Appl Physiol (1985) 2001;91:1619–26. doi: 10.1152/jappl.2001.91.4.1619. [DOI] [PubMed] [Google Scholar]
- Murphy TV, et al. TRPV3 expression and vasodilator function in isolated uterine radial arteries from non-pregnant and pregnant rats. Vascul Pharmacol. 2016;83:66–77. doi: 10.1016/j.vph.2016.04.004. [DOI] [PubMed] [Google Scholar]
- Olive JL, et al. Vascular conductance is reduced after menthol or cold application. Clin J Sport Med. 2010;20:372–6. doi: 10.1227/NEU.0b013e3181e57bca. [DOI] [PubMed] [Google Scholar]
- Peier AM, et al. A TRP channel that senses cold stimuli and menthol. Cell. 2002;108:705–15. doi: 10.1016/s0092-8674(02)00652-9. [DOI] [PubMed] [Google Scholar]
- Pires PW, et al. Unitary TRPV3 channel Ca2+ influx events elicit endothelium-dependent dilation of cerebral parenchymal arterioles. Am J Physiol Heart Circ Physiol. 2015;309:H2031–41. doi: 10.1152/ajpheart.00140.2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roustit M, Cracowski JL. Non-invasive assessment of skin microvascular function in humans: an insight into methods. Microcirculation. 2012;19:47–64. doi: 10.1111/j.1549-8719.2011.00129.x. [DOI] [PubMed] [Google Scholar]
- Roustit M, et al. Excellent reproducibility of laser speckle contrast imaging to assess skin microvascular reactivity. Microvasc Res. 2010;80:505–11. doi: 10.1016/j.mvr.2010.05.012. [DOI] [PubMed] [Google Scholar]
- Smith CJ, et al. Upregulation of inducible nitric oxide synthase contributes to attenuated cutaneous vasodilation in essential hypertensive humans. Hypertension. 2011;58:935–42. doi: 10.1161/HYPERTENSIONAHA.111.178129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stanhewicz AE, et al. Local tetrahydrobiopterin administration augments reflex cutaneous vasodilation through nitric oxide-dependent mechanisms in aged human skin. J Appl Physiol (1985) 2012;112:791–7. doi: 10.1152/japplphysiol.01257.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sun J, et al. Activation of cold-sensing transient receptor potential melastatin subtype 8 antagonizes vasoconstriction and hypertension through attenuating RhoA/Rho kinase pathway. Hypertension. 2014;63:1354–63. doi: 10.1161/HYPERTENSIONAHA.113.02573. [DOI] [PubMed] [Google Scholar]
- Tew GA, et al. Reproducibility of cutaneous thermal hyperaemia assessed by laser Doppler flowmetry in young and older adults. Microvasc Res. 2011;81:177–82. doi: 10.1016/j.mvr.2010.12.001. [DOI] [PubMed] [Google Scholar]
- Topp R, et al. Topical menthol, ice, peripheral blood flow, and perceived discomfort. J Athl Train. 2013;48:220–5. doi: 10.4085/1062-6050-48.1.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Topp R, et al. Effect of topical menthol on ipsilateral and contralateral superficial blood flow following a bout of maximum voluntary muscle contraction. Int J Sports Phys Ther. 2011;6:83–91. [PMC free article] [PubMed] [Google Scholar]
- Ungvari Z, et al. Increases in endothelial Ca(2+) activate K(Ca) channels and elicit EDHF-type arteriolar dilation via gap junctions. Am J Physiol Heart Circ Physiol. 2002;282:H1760–7. doi: 10.1152/ajpheart.00676.2001. [DOI] [PubMed] [Google Scholar]
- Wong BJ. Sensory nerves and nitric oxide contribute to reflex cutaneous vasodilation in humans. Am J Physiol Regul Integr Comp Physiol. 2013;304:R651–6. doi: 10.1152/ajpregu.00464.2012. [DOI] [PubMed] [Google Scholar]
- Yang XR, et al. Functional expression of transient receptor potential melastatin- and vanilloid-related channels in pulmonary arterial and aortic smooth muscle. Am J Physiol Lung Cell Mol Physiol. 2006;290:L1267–76. doi: 10.1152/ajplung.00515.2005. [DOI] [PubMed] [Google Scholar]