

Abstract
Impaired cognition has a significant impact on a person’s ability to manage their medicines. The aim of this paper is to provide a narrative review of contemporary literature on medicines management by people with dementia or cognitive impairment living in the community, methods for assessing their capacity to safely manage medicines, and strategies for supporting independent medicines management. Studies and reviews addressing medicines management by people with dementia or cognitive impairment published between 2003 and 2013 were identified via searches of Medline and other databases. The literature indicates that as cognitive impairment progresses, the ability to plan, organise, and execute medicine management tasks is impaired, leading to increased risk of unintentional non-adherence, medication errors, preventable medication-related hospital admissions and dependence on family carers or community nursing services to assist with medicines management. Impaired functional capacity may not be detected by health professionals in routine clinical encounters. Assessment of patients’ (or carers’) ability to safely manage medicines is not undertaken routinely, and when it is there is variability in the methods used. Self-report and informant report may be helpful, but can be unreliable or prone to bias. Measures of cognitive function are useful, but may lack sensitivity and specificity. Direct observation, using a structured, standardised performance-based tool, may help to determine whether a person is able to manage their medicines and identify barriers to adherence such as inability to open medicine packaging. A range of strategies have been used to support independent medicines management in people with cognitive impairment, but there is little high-quality research underpinning these strategies. Further studies are needed to develop and evaluate approaches to facilitate safe medicines management by older people with cognitive impairment and their carers.
Keywords: Cognitive impairment, dementia, functional ability, medicines management, self-care
Introduction
Managing one’s own medicines is a skill that is necessary for successful independent living [1]. Impaired cognition can have a significant impact on a person’s ability to manage medicines safely, leading to increased risk of unintentional non-adherence and medication errors [2-4], preventable medication related hospital admissions [5], and dependence on family carers or community nursing services to assist with medicines management [6]. Older people with cognitive impairment may also experience reduced psychomotor and physical abilities [7] further increasing the risk of medicines management problems and non-adherence [3].
It is estimated that 12 million people worldwide have a diagnosis of dementia, and this is expected to increase to 25 million by 2040 [8]. Increasing numbers of older people with cognitive impairment or dementia are requiring support with managing medicines at home (e.g. from family carers or community nursing services), as a result of increasing intensity of medical therapy for chronic diseases (leading to increasing polypharmacy), and a shift towards home-based care in place of residential care. This increased reliance on health and aged care services due to cognitive and functional decline has led to a pressing need for strategic and cost-effective measures to manage the impact on those affected and the community [9]. In order to develop strategies to reduce the associated burden with dementia, in 2012, the Australian Federal Government declared dementia a national health priority [10].
The World Health Organisation (WHO) report ‘Dementia: a public health priority’ recommended the promotion of dementia friendly societies and investing in health systems to improve care and services for people with dementia and their carers [11]. There are a number of problems with current systems and models for assessing and supporting safe medicines management by older people in the community [2], particularly where cognitive decline or dementia is a factor. Therefore, the aim of this paper is to provide a narrative review of contemporary literature on medicines management by people with dementia or cognitive impairment, methods for assessing their capacity to safely manage medicines, and strategies for supporting independent medicines management.
Search strategy
To identify literature about medicines management in people with dementia or cognitive impairment, searches of EMBASE, MEDLINE and CINAHL were undertaken (see Table 1). The search included only articles in English and to ensure relevance to current practice only articles published between 2003 and 2013. Articles were examined for relevance, and articles reporting on medicines for treatment of dementia or cognitive impairment rather than management of the medicines of people with dementia/ cognitive impairment were excluded, as were articles focussing on older people residing in institutional care. Articles that did not focus on medicines management but other activities of daily living were also excluded.
Table 1.
EMBASE, Medline, Cinahl search strategy*.
| EMBASE/MEDLINE | CINAHL |
|---|---|
| MESH terms ‘mental competency’ ’prescription drugs’ ‘self medication’ ‘self administration’ ’patient participation’ ‘decision making’ ’medication adherence’ ’medication errors ”medication therapy management’ ’non prescription drugs’ ‘pharmaceutical preparations’ ‘medications’ ‘cognitive disorders’ ‘memory disorders’ ‘dementia’ ‘Alzheimers Disease’ (219 articles retrieved) Key word search ‘cognitive impairment’ and ‘medicines management’ (67 articles retrieved) |
MESH terms ‘dementia’ ‘cognition disorders’ ’Alzheimer’s disease’ ’medications’ ‘drugs’ ‘self administration’ ’medication errors’ (20 additional articles were retrieved) |
| After duplicates were removed a total of 306 articles on medicines management on people with dementia were retrieved and examined for relevance. | |
*The search strategy was devised by a librarian with substantial experience in the MESH terms and Keywords appropriate to each particular Database.
To identify tools for assessing older persons’ cognitive and physical capacity to manage medicines, we used reviews conducted by one of the authors [12, 13], and updated the literature search (to December 2013) using the same search strategy and inclusion criteria described in the 2009 systematic review [12].
Impact of cognitive impairment on medicines management
As people age most experience some impairment in dexterity, mobility, hearing and vision. The presence of cognitive impairment compounds these changes, often with significant impact on functional status [2] including safe self-administration of medicines. For example, in a large cross-sectional study of older people (mean age 87 years) it was reported that 14% were unable to open a screw capbottle, 32% a bottle with a snap lid, and 10% a blister pack [7]. Dementia diagnosis and lower mini-mental state examination (MMSE) scores were strongly associated with reduced ability to open medicine containers. People with dementia were at least three times more likely to be unable to remove medicines from packaging, even after adjusting for other factors such as age, impaired vision and arthritis.
As dementia progresses, affecting memory and other aspects of cognition, the ability to plan, organise, and execute tasks required in the medicines management process is impaired. Problems associated with non-adherence to medicines regimens in those with dementia include poor therapeutic outcomes or therapeutic failure, escalating diagnostic and therapeutic measures, increased risk of adverse events and hospitalisation or repeat hospitalizations [2]. In a 2008 review by Arlt et al., it was reported that there is increasing knowledge and insight about the factors that influence adherence behavior in older age and its relationship to cognitive capacity, memory and executive function, but that awareness of non-adherence as a result of cognitive impairment is relatively low [2].
There is little quantitative data on the prevalence of medication errors, non-adherence and adverse medication events in people with dementia or cognitive impairment, because few studies have focussed exclusively on these types of patients [4]. In one study of people with dementia living at home, injury resulting from medication self-administration that required emergency attendance was reported to be the fifth most common source of harm, with the leading sources being failure to eat and drink, and failure to report a medical condition [14]. In a Dutch study the strongest risk-factor for preventable medication-related hospital admissions was impaired cognition (oddsratio, 11.9; 95% confidence interval, 3.9-36.3) [5].
Kaasalainen et al., 2011, used a grounded theory approach to ascertain the challenges that older adults with dementia living in the community face with medicines management. Analysis of 57 interviews revealed that severity of dementia in older people was associated with changes in medicines management behaviours, and a number of corresponding facilitators and barriers to safe medicines management. Facilitators included interdisciplinary collaboration, geriatrician assessment, caregiver respite and support, trust between caregiver and patient and patient, caregiver and health professional, morning medicines and an established routine for managing medicines. Barriers were living alone, limited caregiver availability or forgetful caregiver, forgetfulness and confusion, lack of insight, introduction of new medicines or learning a new medication system and the number and frequency of medicines [15].
Other findings reported by Kaasalainen et al., were that:
Medicines self-administration in early stage dementia is characterised by the persons’ desire to maintain their independence, their denial of disease related issues and anger, sometimes resulting in refusal to take medicines [15].
In late stage dementia, older adults may refuse medicines as an outcome of delusional or suspicious thinking, resulting in caregivers assuming responsibility for medicines management [15].
While et al., interviewed 34 people with dementia or their carers, and reported that other factors affecting self-management capability included: low health literacy impacting on ability to follow instructions, and complexity of the medicine regimen (including managing more than one medicine and taking medicines more than once a day) [6]. Family carers recognised that medical practitioners are in a difficult position trying to identify medicine management problems and assist people with dementia to manage medicines, as they are reliant on carers for feedback, and at times they struggle to be inclusive of both the person with dementia and their family carer [6].
Identifying impaired capacity to manage medicines
Impaired functional ability may not be detected by health professionals in routine clinical encounters [16], and may not be reported by patients. In one study, only 27% of people who were unable to open one or more containers were receiving help with their medicines [7]. In another study, lack of assistance in those needing medication support was associated with higher risk of hospitalisation and institutionalisation [17].
Assessment of patients’ (or their carers’) ability to safely manage medicines is not undertaken routinely by health professionals, and when it is undertaken there is variability in the methods used [6, 13]. How to assess a person’s capacity to manage their medicines depends to a large extent on the severity of their cognitive impairment and their willingness and ability to cooperate [2]. Availability of an informant, usually a family member or carer with first-hand knowledge about the person’s recent medicines management performance, is also an important consideration. The goal should be to recognise people who are having difficulties with medicines management before significant errors or non-adherence occur [2].
It is important to note that adherence to a medicines regimen may be influenced by many factors, not just the person’s capacity to manage medicines. The person’s attitudes and beliefs about medicines and health, ability to pay for medicines and access to a pharmacy are all contributing factors [18]. Methods for identifying medication non-adherence and factors that contribute to non-adherence have been extensively reviewed [2, 18, 19], and are not discussed further here. This section focuses on methods for assessing a person’s cognitive and physical capacity to safely and accurately manage their medicines. Factors to consider when assessing a person’s ability to manage their medicine regimen are summarised in Fig. 1.
Fig. (1).
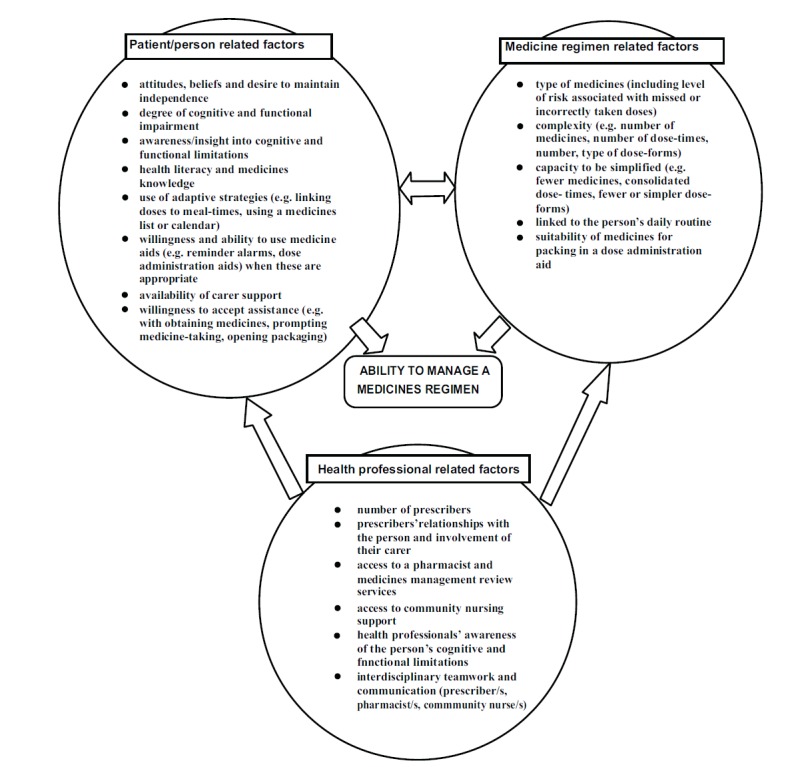
Factors that influence a person’s ability to manage their medicines.
Self-report and Informant Report
Patient self-report or informant report is a reasonable starting point for identifying problems with medicines management, but a limitation is that these can be prone to bias [16]. Some older people, especially with cognitive impairment, have difficulty evaluating their own competence or are reluctant to admit their inability to cope, potentially leading to over-estimation of performance [6, 20-22].
Family members or caregivers may under- or over-estimate performance, depending on their familiarity with the person’s medicines needs and behaviours and the degree of caregiver burden experienced, or they may be unable to make a determination because of a lack of opportunity to observe the person [17, 21, 23].
Cognitive Screening Tools
Since ability to manage medicines is known to be associated with cognitive functioning [13, 24, 25], measures of cognition such as the MMSE are sometimes used to identify people who may be at risk of medicine management problems. Often the focus of assessment is the person’s ability to remember to take their medicines, but in those with cognitive impairment non-adherence may also be due to improper use of medicines or medicine administration devices, such as inhalers. Higher MMSE scores are associated with better performance on multi-dose inhaler devices [26] and use of a simple drawing test (Intersecting Pentagons) identified people that were unlikely to be able to learn to use a Turbuhaler dry powder device [27]. In 2009, Board & Allen reported that in clinical practice most persons with an MMSE <24 or inability to copy Intersecting Pentagons (IP) will not be able to learn to use a multi-dose inhaler effectively. IP had the best overall predictive value [28].
Although many studies have reported associations between cognitive function screening or cognitive assessment tools and patients’ ability to manage medicines, a limitation is that these measures may lack sensitivity and specificity in discriminating competent from incompetent individuals, and it is unclear what scores on cognitive screening tools indicate inability to manage medicines [1, 29-31]. Furthermore, MMSE may be unreliable in people with poor literacy or numeracy skills. Measures of cognitive function may serve as a useful initial screen, but should not be used alone to determine whether a person with mild to moderate cognitive impairment can safely manage their own medicines.
Functional Assessment Tools
Commonly used functional assessment tools (e.g. the Lawton IADL scale) include items relating to medicines management [32]. Generally these rely on self-report or informant report, and they often include only a single item to assess medicines management ability despite this being a complex multi-faceted task. These tools also lack clear definitions for the skills required and provide little information as to the cause of identified incapacity. When compared with direct observation, they may over-estimate performance [33].
Direct Observation
Sometimes health professionals judge a person’s ability to manage medicines based on informal, unstructured observation. This has the advantage of enabling the person’s actual performance to be assessed, and therefore may be a more effective approach than relying on self-report or cognitive screening tests, but it is of unproven reliability [34].
A number of structured, standardised performance-based tools designed to assess a person’s ability to manage medicines have been developed [12, 13], although few have found their way into routine clinical practice [2, 13]. A 2009 literature review identified 14 tools designed to assess cognitive and physical ability to manage medicines [12]. Our update of the literature search (to December 2013) identified additional tools [31, 35-39], of which three met the inclusion criteria of the 2009 review [35, 38]. Published tools fell into two broad categories: those that used the person’s own medicines as the basis for assessment (n=3) [40-42], and those that used a simulated medicine regimen (n=14) [7] [35, 38, 39, 43-52]. In contrast, most unpublished, unvalidated tools used in clinical practice use a person’s own medicines [13].
There is considerable variation in the methods used to assess medicines management and the range of skills assessed by published and unpublished tools [12, 13]. No identified instrument included a structured or standardised method for assessing ability to use non-oral dose-forms such as inhalers, despite the fact that there are examples of such protocols in the literature [53]. Several tools assessed ability to fill a dose administration aid, but only one included an assessment of ability to use a pre-filled dose administration aid [12, 13, 39], even though these devices are commonly used by people with cognitive impairment and it has been reported that some people have difficulty using them [6, 54].
Most instruments took between 5 and 15 minutes to administer. Instruments that included an assessment of medication knowledge in addition to the medication-taking task required more time (15-30 minutes). Administration time may be longer in people with cognitive impairment [12]. Most instruments have undergone limited evaluation of reliability, and although most published tools have demonstrated an association with at least one related construct (e.g. cognitive function, performance of other IADLs) there is limited evidence of their ability to predict successful independent medication management [12]. Validation studies usually had methodological shortcomings, and therefore further studies are required to determine the tools’ predictive validity [12].
Two structured medicines management assessment tools that have been widely studied and appear to have reasonable reliability and validity are the Drug Regimen Unassisted Grading Scale (DRUGS) and the Medication Management Ability Assessment (MMAA) (see Table 2) [12, 50].
Table 2.
Examples of structured, standardised performance-based tools medicine management assessment tools [12].
| Drugs [ 40 ] | MMAA [ 50 ] | |
|---|---|---|
| Medicine regimen used for assessment | The person’s own medicines | A simulated medication regimen |
| Method | The person is asked to perform the following four tasks with each medicine: 1) identify the medicine, 2) open the container, 3) select the correct dose, and 4) report the appropriate timing of doses using a grid marked with specific times of the day as a role-play of their typical day. |
Four plastic pill bottles with dried beans are labelled with directions. The interviewer describes the medication regimen to the subject, then 45-60 minutes later the subject is asked to walk through their day, saying when they would wake up, eat meals, and take each medication. They are required to dispense the pills for each dose and hand them to the interviewer. |
| Scoring | Out of 100. Each drug is scored out of 4, with 1 for each correct response/action. This is then converted to a percentage score. The composite score is the overall average score. | Several scoring methods have been reported, for example: A) Total MMAA score (out of 25): One point deducted for each deviation from prescribed regimen (i.e. too many or too few pills or incorrect timing in relation to food). B) Total number of pills correct (out of 21) (see reference [12] for more details) |
| Reliability | Evidence of good inter-rater and test-retest reliability. | Evidence of good test-retest reliability but inter-rater reliability unknown. |
| Validity | Construct validity has been demonstrated through associations between DRUGS scores and cognitive function, health literacy, independent medication management and MMAA performance. DRUGS scores have also been shown to be responsive to change. | Construct validity has been demonstrated through associations between MMAA scores and cognitive function, observed IADL performance, and DRUGS scores. |
| Typical administration time* | Approximately 15 minutes. | Approximately 15 minutes, plus a 45 minute delay between explaining the regimen to the person and task completion. |
| Application | May be best suited to assessments conducted in patients’ homes, with access to their own medicines, or assessment as part of a ‘brown bag medicine review’ where the person brings their medicines to the clinic or pharmacy. | May be suited to situations where a person’s ability to manage a new medicines regimen needs to be assessed, and/or where the person’s own medicines are not available, such as in hospital. |
DRUGS = Drug Regimen Unassisted Grading Scale; IADL = instrumental activities of daily living; MMAA = Medication Management Ability Assessment
*Administration times may be longer in people with cognitive impairment
Self-Administration of Medicines Programs
Another approach to assessing a person’s capacity to manage their medicines accurately and safely is through a self-administration of medicines program (SAMP) [55]. These programs are offered in some hospitals, and enable a person to self-administer their medicines under supervision prior to discharge. They enable hospital clinicians to determine whether a person is likely to be able to manage their medicines after discharge and identify barriers to safe self-administration. For example, a study of SAMP participants at an Australian hospital reported that almost 20% of patients who intended to manage their own medicines at home were not safe to do so, and a further 11% had barriers to safe medicines management identified that needed to be addressed (e.g. difficulty opening containers, inability to remember to take their medicines) [56]. Inpatient SAMPs have also been reported to increase patients’ understanding of their medicines regimens and improve their ability to manage their medicines after discharge [55, 57].
Application of Medicines Management Assessment Tools
It has been suggested that supplementing self-reported information with objective functional assessment might improve detection of older adults who are experiencing functional decline, thus permitting timely and targeted interventions to reduce the risk of adverse outcomes [55]. Structured, performance-based medicines management assessment instruments may therefore be useful in clinical practice to identify barriers to self-management and assist health professionals to identify patients’ in need of education, regimen simplification, medication assistance or medication aids [12]. They could also serve an additional function as cognitive screening tools, since they have all demonstrated associations with performance on cognitive screening tests such as the MMSE [12]. In fact some medicines management assessment tools were initially developed as cognitive screening tools [38, 47].
Whilst performance-based measures provide an objective assessment of functional performance, it is important to note that they assess what a person is able to do (i.e. capacity), which may not reflect what they actually do [16, 58]. Additionally, they do not assess what the person wants to do. Performance based-measures need to be used as part of a comprehensive assessment of the person’s medicines management processes, routines and supports, their medication-related beliefs, goals and preferences, and other factors that might impact on medicine use and adherence (e.g. financial status, adverse drug reactions). Informant information, if available, should also be considered. Taking a strengths-based, person centred approach is more appropriate than focussing on the person’s deficits or making assumptions based on a dementia diagnosis or results of global cognitive function tests [6].
Strategies to improve medicines management by people with cognitive impairment
The ability to manage medicines is a continuum, ranging from independent self-management through to total dependence on others. A person with dementia may adapt to their changing cognitive and functional abilities as their disease progresses, by using internal and external strategies to assist with medicines management (e.g. linking dose-times to meal-times, using reminder cards or dosing aids) and assigning some medicines management tasks to family members (e.g. obtaining prescriptions, opening packaging, prompting medicine-taking) [6].
Understanding the motivation, beliefs and attitudes of a person with dementia are important considerations when trying to influence medicine-taking behaviours [6, 59]. Adherence to a medicines regimen is more likely when the person believes that their medicines are important to maintaining well-being, independence and life [6]. An awareness of the outcomes of specific medicines and the appearance and names of tablets also support adherence to prescribed medicines in older people with dementia [6]. Health professionals may not always demonstrate insight into the information needs of the client in relation to their medicines, however, and perceived passivity of the person with dementia may influence the amount of information provided about medicines resulting in insufficient information to optimise the person’s treatment and outcomes [6]. When providing medicines information to a person with cognitive impairment, the amount and format of the information is important, taking into consideration level of cognitive impairment and the education level and language of the consumer and or their carer [6, 59].
Strategies that simplify medicines regimens are important for assisting a person with cognitive impairment (or their carer) to manage their medicines [2]. Examples include reducing the number of prescribed medicines or reducing the number of dose-times [60]. This requires an accurate medication history, inspection of all medicines used (including non-prescribed and complementary medicines) and review of the medicines regimen [2].
Many older people with dementia maintain safe and effective medicines self-administration by incorporating a range of behavioural strategies into their daily life, relying on routines and visual and auditory cues. Dose administration aids and reminder alarms are added when specific or additional cues are required to maintain behaviours [6, 59].
Although dose administration aids are commonly used there has been little high quality research on their effectiveness and safety [61]. Most studies have had methodological flaws (for example no control group or inadequate randomisation, short duration, high loss to follow-up, and confounding due to application of multiple concurrent adherence strategies), and few have focussed on people with cognitive impairment. Most trials have focused on a single health problem, for example hypertension, limiting generalisability to typical users of dose administration aids (people with multiple comorbidities). A recent Cochrane review pooled data from several studies (none focussed on older people or people with cognitive impairment) and found that dose administration aids modestly increased the percentage of pills taken (mean difference of 11%, 95% confidence interval 6–17%) [62]. Despite a lack of evidence that they improve the percentage of pills taken, qualitative studies suggest that in appropriately selected people there may be benefits such as fewer medicines needing to be stored at home (if the device is packed by a pharmacy), fewer duplicated doses (as a result of not remembering that a dose was already taken), fewer missed or incorrect doses, and less stress for the individual or their carer to remember which medicine to take when [6, 61]. There is evidence that many older people, especially those with cognitive impairment, have difficulties managing dose administration aids, and that introducing them too early can lead to disempowerment and de-skilling of the individual, so these devices need to be used judiciously [61].
A systematic review by Campbell et al., published in 2012, identified only three published studies evaluating interventions to improve medicine adherence in older adults with cognitive impairment. The interventions focussed on providing reminders and cueing systems, with mixed success [63]. The first was a nurse-led intervention in which reminder cues and dose administration aids were provided. This intervention did not significantly improve medicine adherence. In a small controlled study, use of telephone or televideo prompting was reported to increase medicine adherence. The third study reported that use of refill reminder postcards and an illustrated medication schedule did not improve adherence [63]. A further small, uncontrolled study by Kamimura et al., (2012) demonstrated that a medicines reminder device (a dose-administration aid that omitted an audible alarm when doses were due to be taken) may assist older people with mild cognitive impairment to maintain independence with medicine-taking and improve adherence [64].
These findings highlight the challenges associated with improving medicines management and adherence in older people with cognitive impairment, and the fact that there has been limited research focussing on this high-risk group of people. Prompting and reminding to take medicines as prescribed may be more effective when delivered by another person than by automated devices or other methods, however, further research is needed to confirm these findings [6, 63].
Health service provision for older people with cognitive impairment
In their review of the literature on medicines management for individuals who live in the community and have both chronic illness and mild to moderate dementia Kralik et al., discussed the importance of person-centred care co-ordination and consumer partnerships in medicines management. Specifically, the authors reported the necessity for coordinated, tailored and flexible care processes [64]. While acknowledging that in the Australian setting a range of services and programs aim to support people living in the community (e.g. Home and Community Care Services (HACC) and Home Medicines Review - a government-funded medication review conducted by a pharmacist in the person’s home, on referral from their medical practitioner), they identified a lack of care coordination, with services limited by a lack of collaboration between service providers [65].
Acute hospital admission is often a trigger for changes to older persons’ medicines regimens. Current hospital admission and discharge processes in relation to provision of information about medicines and support for returning to self-administration and self-management of medicines, has been identified as inadequate [66, 67] and may compromise the safety of people who have dementia.
Discussion
This review highlights the impact of cognitive impairment and dementia on older peoples’ ability to manage medicines, methods for assessing people’s ability to manage medicines, and the need for older people living with cognitive decline or dementia and taking prescribed medicines to have access to services providing comprehensive medicines management assessment. Comprehensive assessment, conducted by a competent health professional, would assist in determining the person’s capacity for medicines self-administration and contribute to processes supporting the older person to maintain the level of independence that they desire and are capable of. Assessment should include carers involved in the person’s medicines management and aim to develop an understanding of their goals of treatment, attitudes and beliefs about medicines use. Greater understanding of and respect for older peoples’ attitudes and beliefs about acceptable levels of safety versus autonomy in medicines taking may also influence medicines management behaviours’.
Assessment of cognitive ability, using instruments such as the MMSE, may form part of a medicines assessment but is not an adequate substitute for a comprehensive medicines assessment and history. Assessments based upon the person’s strengths and abilities may assist in facilitating and maintain greater levels of independence in medicines management. Existing medicines assessment tools limit functional assessment of medicines self-administration to oral preparations; evidence is presented here indicating that this should be extended to any and all forms of medicine that an individual uses or that their carer administers, such as inhalers, eye drops, patches and other devices. Specific assessment of the suitability of dose administration aides including pre-packaged systems for older people could also assist in supporting independence for people with dementia and their carers.
Despite the development of validated clinical tools to assist in the process of medicines assessment, health service providers’ time and economic constraints are barriers to the usage of medicines assessment tools in the community setting and limit their wider use. Healthcare funders need to ensure that health professionals are adequately resourced to assess peoples’ medicine management skills, because without comprehensive assessment there is insufficient knowledge and data gathered to plan appropriate care, support and enablement for older adults with cognitive impairment and their carers, potentially leading to increased economic and health care burden.
Conclusion
Impaired cognition affects peoples’ ability to manage medicine regimens, and increases the risk of errors and adverse events. Impaired ability to manage medicines may not be detected in routine clinical practice, and although validated tools for assessing a person’s ability to manage medicines exist, they are rarely used. When cognitive impairment is identified or suspected, increased focus on assessing the person’s ability to safely manage their medicines is needed, using reliable and valid methods. As there has been limited research evaluating strategies to improve medicine-taking in people with cognitive impairment, further studies in this area are urgently needed.
ACKNOWLEDGEMENTS
The authors wish to acknowledge the contribution of Ms. Fleur Duane and Dr. Cik Yin Lee in the preparation of this manuscript and Ms. Jane Edwards for her assistance with the development of the literature search strategy.
CONFLICT OF INTEREST
The authors confirm that they have no conflicts of interest.
References
- 1.Barbas N.R., Wilde E.A. Competency issues in dementia: medical decision making driving and independent living. J. Geriatr. Psychiatry Neurol. 2001;14:199–212. doi: 10.1177/089198870101400405. [DOI] [PubMed] [Google Scholar]
- 2.Arlt S., Lindner R., Rusler A., Von Renteln-Kruse W. Adherence to medication in patients with dementia. Predictors and strategies for improvement. Drugs Aging. 2008;25:1033–1047. doi: 10.2165/0002512-200825120-00005. [DOI] [PubMed] [Google Scholar]
- 3.Field T.S., Mazor K.M., Briesacher B., DeBellis K.R., Gurwitz J.H. Adverse drug events resulting from patient errors in older adults. J. Am. Geriatr. Soc. 2007;55:271–276. doi: 10.1111/j.1532-5415.2007.01047.x. [DOI] [PubMed] [Google Scholar]
- 4.Douglas A., Letts L., Richardson J. A systematic review of accidental injury from fire wandering and medication self administration errors for older adults with and without dementia. Arch. Gerontol. Geriatr. 2011;52:e1–e10. doi: 10.1016/j.archger.2010.02.014. [DOI] [PubMed] [Google Scholar]
- 5.Leendertse A.J., van Dijk E.A., De Smet P.A., et al. Contribution of renal impairment to potentially preventable medication related hospital admissions. Ann. Pharmacother. 2012;46(5):625–633. doi: 10.1345/aph.1Q633. [DOI] [PubMed] [Google Scholar]
- 6.While C., Duane F., Beanland C., Koch S. Medication management The perspectives of people with dementia and family carers. Dementia: Int J Soc Res Pract. 2013;12:734–750. doi: 10.1177/1471301212444056. [DOI] [PubMed] [Google Scholar]
- 7.Beckman A.G., Parker M.G., Thorslund M. Can elderly people take their medicine? Patient Educ. Couns. 2005;59(2):186–191. doi: 10.1016/j.pec.2004.11.005. [DOI] [PubMed] [Google Scholar]
- 8.Burns A., Illiffe S. Dementia. BMJ. 2009;338:405–409. doi: 10.1136/bmj.b75. [DOI] [PubMed] [Google Scholar]
- 9.Australian Medicines Industry Retrieved from http://www.fightdementia.org.au/common/files/NAT/121112_MR_Dementia_Threat_Haunting_Australia.pdf. (accessed March 2014) 2012.
- 10.Australian Institute of Health and Welfare National Health Priority areas. Retrieved from http://www.aihw.gov.au/nationalhealth-priority-areas/ (accessed March 2014) 2013.
- 11.World Health Organisation and Alzheimer’s Disease International Dementia: A Public Health Priority. Geneva:WHO2012. http://www.who.int/mental_health/publications/dementia_report_2012/en/ (accessed March 2014)
- 12.Elliott RA, Marriott J. Standardised assessment of patients' capacity to manage medications a systematic review of published instruments. . BMC Geriatrics . 2009. [DOI] [PMC free article] [PubMed]
- 13.Elliott R.A., Marriott J. Review of instruments used in clinical practice to assess patients’ ability to manage medications. J Pharm Pract Res. 2010;40:36–41. [Google Scholar]
- 14.Tierney M., Charles J., Naglie G., Jaglal S., Kiss A., Fisher R. Risk factors for harm in cognitively impaired seniors who live alone: a prospective study. J. Am. Geriatr. Soc. 2004;52:1435–1441. doi: 10.1111/j.0002-8614.2004.52404.x. [DOI] [PubMed] [Google Scholar]
- 15.Kaasalainen S., Dolovich L., Papaioannou A., et al. The process of medication management for older adults with dementia. J. Nurs. Healthc. Chronic Illn. 2011:10. [Google Scholar]
- 16.Applegate W.B., Blass J.P., Williams T.F. Instruments for functional assessment of older patients. N. Engl. J. Med. 1990;322:1207–1214. doi: 10.1056/NEJM199004263221707. [DOI] [PubMed] [Google Scholar]
- 17.Kuzuya M., Hirakawa Y., Suzuki Y., et al. Association between unmet needs for medication support and all cause hospitalization in community dwelling disabled elderly people. J. Am. Geriatr. Soc. 2008;56:881–886. doi: 10.1111/j.1532-5415.2008.01676.x. [DOI] [PubMed] [Google Scholar]
- 18.Nguyen T., Caze A., Cottrell N. What are validated self report adherence scales really measuring? a systematic review. Br. J. Clin. Pharmacol. 2014;77:427–445. doi: 10.1111/bcp.12194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lavsa S.M., Holzworth A., Ansani N.T. Selection of a validated scale for measuring medication adherence. J. Am. Pharm. Assoc. 2011;51:90–94. doi: 10.1331/JAPhA.2011.09154. [DOI] [PubMed] [Google Scholar]
- 20.Karagiozis H., SarahSacco J, Martha Kawas C. The Direct Assessment of Functional Abilities (DAFA) A Comparison to an Indirect Measure of Instrumental Activities of Daily Living. Gerontologist. 1998;38:113–121. doi: 10.1093/geront/38.1.113. [DOI] [PubMed] [Google Scholar]
- 21.Allaire J., Gamaldo C., Ayotte B.J., Sims R., Whitfield K. Mild cognitive impairment and objective instrumental everyday functioning the everyday cognition battery memory test. J. Am. Geriatr. Soc. 2009;57:12–125. doi: 10.1111/j.1532-5415.2008.02054.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Maidment I.D., Fox C., Boustani M., Katona C. Medication management the missing link in dementia interventions. Int. J. Geriatr. Psychiatry. 2012;27:439–442. doi: 10.1002/gps.2745. [DOI] [PubMed] [Google Scholar]
- 23.Mangone C.A., Sanguinetti R.M., Baumann P.D., et al. Influence of Feelings of Burden on the Caregiver's Perception of the Patient's Functional Status. Dement Geriatr Cogn. 1993;4:287–293. doi: 10.1159/000107335. [DOI] [PubMed] [Google Scholar]
- 24.Yeh Y.C., Lin K.N., Chen W.T., Lin C.Y., Chen T.B., Wang P.N. Functional disability profiles in amnestic mild cognitive impairment. Dement Geriatr Cogn. 2011;31:225–232. doi: 10.1159/000326910. [DOI] [PubMed] [Google Scholar]
- 25.Alosco M.L., Spitznagel M.B., van Dulmen M., et al. Cognitive function and treatment adherence in older adults with heart failure. Psychosom. Med. 2012;74:965–973. doi: 10.1097/PSY.0b013e318272ef2a. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Fraser M., Patel M., Norkus E., Whittington C. The role of cognitive impairment in the use of diskus inhaler. JAMDA. 2012;13:390–393. doi: 10.1016/j.jamda.2011.04.004. [DOI] [PubMed] [Google Scholar]
- 27.Board M., Allen S. A simple drawing test to identify patients who are unlikely to be able to learn to use an inhaler. Int. J. Clin. Pract. 2006;60:510–513. doi: 10.1111/j.1368-5031.2006.00933.x. [DOI] [PubMed] [Google Scholar]
- 28.Allen S., Warwick Sanders M., Baxter M. A comparison of four tests of cognition as predictors of inability to learn to use a metered dose inhaler in old age. Int. J. Clin. Pract. 2009;63:1150–1153. doi: 10.1111/j.1742-1241.2009.02060.x. [DOI] [PubMed] [Google Scholar]
- 29.Royall D.R., Chiodo L.K., Polk M.J. Correlates of disability among elderly retirees with “subclinical” cognitive impairment. . J Gerontol A Bio. Sci Med. 2000;55:M541–M546. doi: 10.1093/gerona/55.9.m541. [DOI] [PubMed] [Google Scholar]
- 30.Cromwell D.A., Poulos K, Roslyn G. The performance of instrumental activities of daily living scale in screening for cognitive impairment in elderly community residents. J. Clin. Epidemiol. 2003;56:131–137. doi: 10.1016/s0895-4356(02)00599-1. [DOI] [PubMed] [Google Scholar]
- 31.Anderson K., Jue S.G., Madaras Kelly K.J. Identifying patients at risk for medication mismanagement: using cognitive screens to predict a patient's accuracy in filling a pillbox. Consult Pharm. 2008;23:459–462. doi: 10.4140/tcp.n.2008.459. [DOI] [PubMed] [Google Scholar]
- 32.Graf C. The Lawton Instrumental Activities of Daily Living (IADL) Scale. Ann. Longterm Care. 2007;15(7) [Google Scholar]
- 33.Edwards M.M. The Reliability and Validity of Self-Report Activities of Daily Living Scales. Can. J. Occup. Ther. 1990;57:273–278. [Google Scholar]
- 34.Fulmer T., Gurland B. Evaluating the caregiver’s intervention in the elder’s task performance capacity versus actual behaviour. Int. J. Geriatr. Psychiatry. 1997;12:920–925. doi: 10.1002/(sici)1099-1166(199709)12:9<920::aid-gps664>3.0.co;2-i. [DOI] [PubMed] [Google Scholar]
- 35.McDougall G.J., Becker H., Vaughan P.W., Acee T.W., Delville C.L. The revised direct assessment of functional status for independent older adults. Gerontologist. 2010;50:363–370. doi: 10.1093/geront/gnp139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sino C.G., Sietzema M., Egberts T.C., Schuurmans M.J. Medication management capacity in relation to cognition and self management skills in older people on polypharmacy. J. Nutr. Health Aging. 2014;18:44–49. doi: 10.1007/s12603-013-0359-2. [DOI] [PubMed] [Google Scholar]
- 37.Kim J.S., Kim J.M., Kim H.J., Yun J.Y., Jeon B.S. Use of the Pill Questionnaire to detect cognitive deficits and assess their impact on daily life in patients with Parkinson's disease. Neurol. Asia. 2013;18:369–375. [Google Scholar]
- 38.Zartman A.L., Hilsabeck R.C., Guamaccia C.A., Houtz A. The Pillbox Test: an ecological measure of executive functioning and estimate of medication management abilities. Arch. Clin. Neuropsychol. 2013;28:307–319. doi: 10.1093/arclin/act014. [DOI] [PubMed] [Google Scholar]
- 39.Irvine Meek J, Gould O. Psychometric evaluation of a self-medication assessment tool in an elderly population. CJHP. 2011;64:16–24. doi: 10.4212/cjhp.v64i1.982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Edelberg H.K., Shallenberger E., Wei J.Y. Medication management capacity in highly functioning community living older adults detection of early deficits. J. Am. Geriatr. Soc. 1999;47(5):592–596. doi: 10.1111/j.1532-5415.1999.tb02574.x. [DOI] [PubMed] [Google Scholar]
- 41.Raehl C.L., Bond C.A., Woods T., Patry R.A., Sleeper R.B. Individualized drug use assessment in the elderly. Pharmacotherapy. 2002;22(10):1239–1248. doi: 10.1592/phco.22.15.1239.33473. [DOI] [PubMed] [Google Scholar]
- 42.Orwig D., Brandt N., Gruber Baldini A.L. Medication management assessment for older adults in the community. Gerontologist. 2006;46(5):661–668. doi: 10.1093/geront/46.5.661. [DOI] [PubMed] [Google Scholar]
- 43.Murray M.D., Darnell J., Weinberger M., Martz B.L. Factors contributing to medication noncompliance in elderly public housing tenants. Drug Intell. Clin. Pharm. 1986;20:146–152. doi: 10.1177/106002808602000210. [DOI] [PubMed] [Google Scholar]
- 44.Meyer M.E., Schuna A.A. Assessment of geriatric patients' functional ability to take medication. DICP. 1989;23(2):171–174. doi: 10.1177/106002808902300214. [DOI] [PubMed] [Google Scholar]
- 45.Romonko L., Pereles L. An evaluation of pharmacy assessment for geriatric patients. Can Hosp Pharm. 1992;45(1):15–20. [PubMed] [Google Scholar]
- 46.Isaac L.M., Tamblyn R.M. Compliance and cognitive function a methodological approach to measuring unintentional errors in medication compliance in the elderly. McGill Calgary Drug Research Team. Gerontologist. 1993;33(6):772–781. doi: 10.1093/geront/33.6.772. [DOI] [PubMed] [Google Scholar]
- 47.Gurland B.J., Cross P., Chen J., et al. A new performance test of adaptive cognitive functioning the Medication Management Test. Int. J. Geriatr. Psychiatry. 1994;9:875–885. [Google Scholar]
- 48.Albert S.M., Weber C.M., Todak G., et al. An observed performance test of medication management ability in HIV relation to neuropsychological status and medication adherence outcomes. AIDS Behav. 1999;3(2):121–128. [Google Scholar]
- 49.Heaton R.K., Marcotte T.D., Mindt M.R., et al. The impact of HIV associated neuropsychological impairment on everyday functioning. J. Int. Neuropsychol. Soc. 2004;10:317–331. doi: 10.1017/S1355617704102130. [DOI] [PubMed] [Google Scholar]
- 50.Patterson T.L., Lacro J., McKibbin C.L., Moscona S., Hughs T., Jeste D.V. Medication management ability assessment results from a performance based measure in older outpatients with schizophrenia. J. Clin. Psychopharmacol. 2002;22(1):11–19. doi: 10.1097/00004714-200202000-00003. [DOI] [PubMed] [Google Scholar]
- 51.Carlson M.C., Fried L.P., Xue Q., Tekwe C., Brandt J. Validation of the Hopkins Medication Schedule to identify difficulties in taking medications. J. Gerontol. A Biol. Sci. Med. Sci. 2005;60(2):217–223. doi: 10.1093/gerona/60.2.217. [DOI] [PubMed] [Google Scholar]
- 52.Schmidt K.S., Lieto J.M. Validity of the Medication Administration Test among older adults with and without dementia. Am. J. Geriatr. Pharmacother. 2005;3(4):255–261. doi: 10.1016/j.amjopharm.2005.12.003. [DOI] [PubMed] [Google Scholar]
- 53.Gray S.L., Williams D.M., Pulliam C.C., Sirgo M.A., Bishop A.L., Donohue J.F. Characteristics predicting incorrect metered dose inhaler technique in older subjects. Arch. Intern. Med. 1996;156:984–988. [PubMed] [Google Scholar]
- 54.Nunney J., Raynor K., Knapp P., Closs S. How do the attitudes and beliefs of older people and healthcare professionals impact on the use of multi compartment compliance aids? a qualitative study using grounded theory. Drugs Aging. 2011;28:403–414. doi: 10.2165/11587180-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 55.Wright J., Emerson A., Stephens M., Lennan E. Hospital inpatient self administration of medicine programmes a critical literature review. Pharm. World Sci. 2006;28:140–151. doi: 10.1007/s11096-006-9014-x. [DOI] [PubMed] [Google Scholar]
- 56.Tran T., Elliott R.A., Taylor S.E., Woodward M.C. A self administration of medications program to identify and address potential barriers to adherence in elderly patients. Ann. Pharmacother. 2011;45:201–206. doi: 10.1345/aph.1P473. [DOI] [PubMed] [Google Scholar]
- 57.Lam P., Elliott R.A., George J. Impact of a self administration of medications program on elderly inpatients competence to manage medications. J. Clin. Pharm. Ther. 2011;36:80–86. doi: 10.1111/j.1365-2710.2009.01157.x. [DOI] [PubMed] [Google Scholar]
- 58.Moore D.J., Palmer B.W., Patterson T.L., Jeste D.V. A review of performance based measures of functional living skills. J. Psychiatr. Res. 2007;41:97–118. doi: 10.1016/j.jpsychires.2005.10.008. [DOI] [PubMed] [Google Scholar]
- 59.Duane F., Goeman D., Beanland C., Koch S. The role of a clinical nurse consultant dementia specialist a qualitative evaluation. Dementia. 2013 doi: 10.11771/1471301213498759. [DOI] [PubMed] [Google Scholar]
- 60.Schlenk E.A., Dunbar Jacob J., Enberg S. Meciation non-adherence among older adults: a review of strategies and interventions for improvement. J. Gerontol. Nurs. 2004;30:33–43. doi: 10.3928/0098-9134-20040701-08. [DOI] [PubMed] [Google Scholar]
- 61.Elliott R.A. Appropriate use of dose administration aids. Aust. Prescr. 2014;37:46–50. [Google Scholar]
- 62.Mahtani K.R., Heneghan C.J., Glasziou P.P., Perera R. Reminder packaging for improving adherence to self administered long term medications. Cochrane Database Syst. Rev. 2011;(9):CD005025. doi: 10.1002/14651858.CD005025.pub3. [DOI] [PubMed] [Google Scholar]
- 63.Campbell N., Boustani M., Skopelja E., Gao S., Unverzagt F., Murray M. Am J Geriatr Pharm. 2012;10:165–177. doi: 10.1016/j.amjopharm.2012.04.004. [DOI] [PubMed] [Google Scholar]
- 64.Kamimura T., Ishiwata R., Inoue T. Medication reminder device for the elderly patients with mild cognitive impairment. Am. J. Alzheimers Dis. (Columbia) 2012;27:238–242. doi: 10.1177/1533317512450066. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Kralik D., Visentin K., March G., et al. Medication Management for Community dwelling Older People with Dementia and Chronic Illness. Aust. J. Prim. Health. 2008;14:25–35. [Google Scholar]
- 66.Hain D., Tappen R., Diaz S., Oustander J. Cognitive impairment and medication self management errors in older adults discharged home from a community hospital. Home Healthc. Nurse. 2012;30:246–254. doi: 10.1097/NHH.0b013e31824c28bd. [DOI] [PubMed] [Google Scholar]
- 67.Cooper G., Deeks L. Dementia medication and care transitions the current Australian experience. Int. J. Pharm. Pract. 2012;20(2):9–10. [Google Scholar]