

Abstract
Hanging is violent asphyxial death. The objective of this study is to assess the data of hanging cases. A descriptive-retrospective study was conducted. We studied 244 hanging cases autopsied in Forensic Division, Department of Pathology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, between January 2001 and December 2013. The study included 197 men (80.7%) and 47 women (19.2%). Their age ranged from 14 to 93 years. Most of these cases were incomplete hanging (83.6%). Features of hanging victims, such as tongue protrusion; congestion of face; petechial hemorrhage of face, conjunctiva, and internal organs; and neck injuries, significantly correlated with complete hanging. The predominant occupation of hanging victims was in the service industry (63.1%). Suicides usually occurred in private homes or apartments (84.8%). A suicide note was found in 6.1% of cases. The most common ligature material used was nylon rope, found in 61.1% of cases. The most underlying diseases of the victims in hanging cases were tuberculosis and human immunodeficiency virus infection, 9 cases each. Blood ethanol levels of 29 cases (11.8%) were detected to be higher than 150 mg%. Methamphetamine and benzodiazepine were detected in 5.3% and 3.3% of cases, respectively. This study provides comprehensive baseline data of hanging cases in central Bangkok.
Keywords: Hanging, forensic pathology, forensic autopsy, cause of death, asphyxia, suicide
Introduction
Hanging is violent asphyxial death caused by suspension of the body by a ligature which encircles the neck, the constricting force being the weight of the body.1 The mode of death in hanging cases is almost always suicide or accident, rarely homicide.2 Hanging is the most common method of committing suicide, followed by fall from height, firearm (in men), and toxic substance (in women).3–5 Hanging usually produces painless and rapid death and can occur even with partial suspension.4 When the body is found completely suspended from above, it is called complete hanging; if some part of the body touches the ground, it is called incomplete or partial hanging.6 There are a number of mechanisms by which hanging produces death. These include stretching of the carotid complex, causing a reflex of cardiac inhibition, venous, and arterial occlusion; airway obstruction; disruption of the spinal cord; and so on.7 This descriptive-retrospective study was done with the objective of assessing data on hanging cases and documenting the characteristics of death cases resulting from hanging.
Materials and Methods
The study design was a descriptive-retrospective one based on autopsy records of the Forensic Division, Department of Pathology, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand, between January 2001 and December 2013. Ramathibodi Hospital is a major medical center where about 80% of the total medicolegal autopsies across the district of Ratchathewi, Phaya Thai, Din Daeng, Huai Khwang, and Dusit (total population of 453 736 spread in an area of 50.7 km2) are performed. The police department of Thailand is legally bound to arrange crime scene investigations and autopsies in all medicolegal deaths with doctors or forensic pathologist. Medicolegal deaths are deaths that are unnatural (including suicide, homicide, and accident), suspicious, or of unknown circumstances. The police papers provide much of the information regarding age, sex, residence, marital status, date of death, reasons and manner of death, and all other relevant information about the case, but we did not include the police information in this study. A total of 6539 medicolegal deaths were reported in this medical center over a period of 13 years. Hanging was noted in 245 (3.7%) cases, with a range of 14 to 23 cases per year with hanging mortality rate of 4.6 per 100 000 population per year. We reviewed the autopsy reports and digital photographs of 244 of 245 cases included; one case with incomplete information was excluded. The data evaluated sex, age group, circumstance of death, ligature material used by the victim, postmortem findings, internal organ injuries, underlying disease, toxicology findings, microscopic findings, and manner of death. In the cases of psychotic disorders which were diagnosed and treated in Ramathibodi Hospital, we reviewed the medical record and noted this information in the autopsy reports.
Data were analyzed using descriptive statistics and χ2 test using SPSS for Windows Version 18.0. Statistical significance was considered to be P ⩽ .05.
Results
Demographic data
In this study, a total of 244 cases were included: 197 men (80.7%) and 47 women (19.2%), ranging in age from 14 to 93 years (Figure 1). The mean age was 37.2 years. The incidence of hanging was more commonly found in the second decade of life (20-29 years, 30.3%) followed by the third decade (30-39 years, 28.3%).
Figure 1.
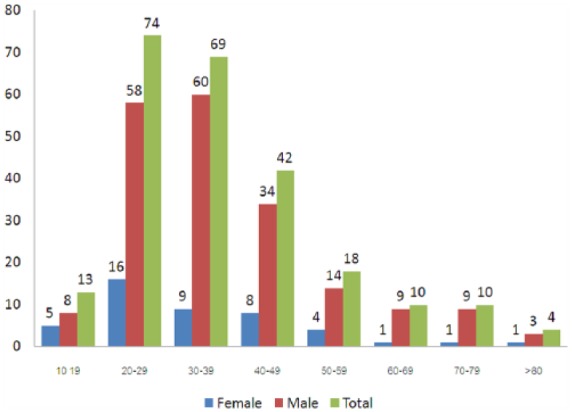
Age and sex distribution of hanging cases.
Body weights of victims ranged from 38 to 87 kg with peak incidence at 60 to 69 kg (36.5%) followed by 50 to 59 kg (26.6%). The average weight was 59 kg. The peak incidence in men was at 60 to 69 kg and in women at 40 to 49 kg.
In hanging deaths, 242 cases were suicidal, and 2 cases were indeterminate because of the atypical characteristics with multiple neck injuries, in which the forensic doctor was not able to rule out homicide.
The conditions of the body in hanging cases are shown in Table 1. If the victims had significant discoloration, marbling, purging of putrefactive fluids, insect activity, skin slippage, foul smelling, or bloating, or a combination of these conditions, they were recorded as decomposed. Overall, only 12.3% of cases were decomposed and 87.7% were fresh. The victim was unidentified in 1.6% of cases.
Table 1.
Condition of body, identity, nationality, and hometown.
| Condition of body | Male, No. (%) | Female, No. (%) | Total, No. (%) |
|---|---|---|---|
| Decomposition | 25 (10.2) | 5 (2.0) | 30 (12.2) |
| Nondecomposition | 172 (70.5) | 42 (17.2) | 214 (87.7) |
| Total | 197 (80.7) | 47 (19.3) | 244 (100) |
| Identified | 194 (79.5) | 46 (18.8) | 240 (98.4) |
| Unidentified | 3 (1.2) | 1 (0.4) | 4 (1.6) |
| Total | 197 (80.7) | 47 (19.3) | 244 (100) |
| Nationality: Thai | 179 (73.4) | 40 (16.4) | 219 (89.8) |
| Nationality: non-Thai | 18 (7.4) | 7 (2.9) | 25 (10.2) |
| Total | 197 (80.7) | 47 (19.3) | 244 (10.2) |
| Hometown: Bangkok | 88 (36.1) | 22 (9) | 110 (45.1) |
| Hometown: other provinces | 91 (37.3) | 18 (7.4) | 109 (44.7) |
| Total | 179 (73.4) | 40 (16.4) | 219 (89.8) |
Percentages are calculated based on the total.
Most of the hanging cases were of Thai nationality (219, 89.8%). The remaining 21 cases (8.6%) were from other countries, including Myanmar (6 cases), Japan (4 cases), China (3 cases), and 1 case each from Laos, Korea, the Netherlands, Africa, Bhutan, Iran, Denmark, and France. Approximately half of Thai victims (110) were from Bangkok and half (109) were from other provinces. However, a slight majority of cases were from outside Bangkok, whereas 9% of female cases were from Bangkok.
Occupation of the victims
Of the 244 victims of hanging cases, most (63.1%) were in the service industry, followed by merchants/managers (12%) and government service (5%) (Table 2). The lowest number of cases was farmers (1 case). In all, 1 female and 9 male victims of hanging were jobless.
Table 2.
Occupation of the victims.
| Occupation | Male, No. (%) | Female, No. (%) | Total, No. (%) |
|---|---|---|---|
| Service | 132 (54.1) | 22 (9) | 154 (63.1) |
| Merchant/manager | 21 (8.6) | 8 (3.3) | 29 (11.9) |
| Government official | 10 (4.1) | 2 (0.8) | 12 (4.9) |
| Servant | 6 (2.4) | 3 (1.2) | 9 (3.7) |
| Student | 4 (1.6) | 4 (1.6) | 8 (3.3) |
| Monk | 2 (0.8) | 0 (0) | 2 (0.8) |
| Farmer | 1 (0.4) | 0 (0) | 1 (0.4) |
| Jobless | 9 (3.7) | 1 (0.4) | 10 (4.1) |
| Not known | 12 (4.9) | 7 (2.9) | 19 (7.8) |
| Total | 197 (80.7) | 47 (19.3) | 244 (100) |
Percentages are calculated based on the total.
Place of hanging
Most (85%) victims hung themselves in their private home or apartment, followed by hostels (3.7%), offices (3.3%), and police stations (2.9%). In total, 164 (67.2%) cases and 43 (17.6%) cases of men and women, respectively, hung themselves in private home or apartment. None of the female victims were found outdoor, and only 1 female victim was found in police station and office. These percentages did not differ significantly between men and women.
Seasonal variation
There was no massive variation in the incidences of hanging cases (Table 3), but suicides of both men and women occurred in all months, except December for women. Most of the men hung themselves in April and July and women in October.
Table 3.
Distribution of month in hanging cases.
| Month | Male, No. (%) | Female, No. (%) | Total, No. (%) |
|---|---|---|---|
| February | 13 (5.3) | 5 (2) | 18 (7.4) |
| March | 12 (4.9) | 3 (1.2) | 15 (6.1) |
| April | 21 (8.6) | 3 (1.2) | 24 (9.8) |
| May | 17 (7) | 4 (1.6) | 21 (8.6) |
| June | 19 (7.8) | 2 (0.8) | 21 (8.6) |
| July | 21 (8.6) | 2 (0.8) | 23 (9.4) |
| August | 9 (3.7) | 5 (2) | 14 (5.7) |
| September | 19 (7.8) | 5 (2) | 24 (9.8) |
| October | 13 (5.3) | 8 (3.3) | 21 (8.6) |
| November | 20 (8.2) | 6 (2.4) | 26 (10.7) |
| December | 20 (8.2) | 0 (0) | 20 (8.2) |
| January | 13 (5.3) | 4 (1.6) | 17 (7) |
Percentages are calculated based on the total. Summer: February to May; Rainy: June to October; Winter: November to January.
Time of death
Time of death in most cases was during daytime between 06.00 am and 06.00 pm (144 cases, 59%), followed by nighttime between 06.00 pm and 06.00 am (100 cases, 41%).
Types of hanging
Complete hanging was seen in 40 cases (16.4%)—30 men and 10 women—and partial (incomplete) hanging in 204 cases (83.6%)—167 men and 37 women.
Ligature material
Types of ligature material used for hanging are shown in Table 4. The most common type of ligature material was rope which was seen in 61% of hanging deaths, followed by fabric material such as cloth (shirt, loincloth, bed sheet) in 19.26% and cable (electric wire) in 7.8%. Both men and women used rope most often, but women used other materials slightly more than men.
Table 4.
Distribution of ligature material.
| Ligature material | Male, No. (%) | Female, No. (%) | Total, No. (%) |
|---|---|---|---|
| Rope | 124 (50.8) | 25 (10.2) | 149 (61.1) |
| Vine | 1 (0.4) | 0 (0) | 1 (0.4) |
| Fabric | 37 (15.2) | 10 (4.1) | 47 (19.3) |
| Hanger | 1 (0.4) | 0 (0) | 1 (0.4) |
| Belt | 5 (2) | 2 (0.8) | 7 (2.9) |
| Spring | 1 (0.4) | 0 (0) | 1 (0.4) |
| Cable | 13 (5.3) | 6 (2.4) | 19 (7.8) |
| Necktie | 2 (0.8) | 0 (0) | 2 (0.8) |
| Strand of blanket | 3 (1.2) | 0 (0) | 3 (1.2) |
| Bag | 3 (1.2) | 1 (0.4) | 4 (1.6) |
| Not known | 7 (2.9) | 3 (1.2) | 10 (4.1) |
| Total | 197 (80.7) | 47 (19.3) | 244 (100) |
Percentages are calculated based on the total.
Position of victims
Most victims (167 [68.4%]) of hanging were found in the standing position, followed by sitting (53 [21.7%]), kneeling (10 [4%]), and lying (4 [1.6%]). In both men and women, the position most found was standing in 133 and 34 cases, respectively, followed by sitting in 44 and 9 cases, respectively. Position in men and women did not differ massively.
Distribution of underlying disease for hanging
Of the 244 cases of hanging, 204 cases (83.6%) showed no evidence of underlying disease (Table 5). In 31 cases (12.7%), single chronic disease was found, followed by multiple chronic disease in 9 cases (3.7%).The most common underlying diseases of victims were tuberculosis and human immunodeficiency virus (HIV) infections (9 cases each), followed by diabetes mellitus and psychotic disorder (major depressive disorder and schizophrenia) (4 cases each). All victims who had tuberculosis were men. HIV victims included 6 men and 3 women. Female victims had a slightly lower disease rate than male victims.
Table 5.
Distribution of underlying disease in hanging victims.
| Underlying disease | Male, No. (%) | Female, No. (%) | Total, No. (%) |
|---|---|---|---|
| Single disease | 27 (11.7) | 4 (1.6) | 31 (12.7) |
| Multiple diseases | 7 (2.9) | 2 (0.8) | 9 (3.7) |
| No underlying disease | 163 (66.8) | 41 (16.8) | 204 (83.6) |
| Total | 197 (80.7) | 47 (19.3) | 244 (100) |
| Tuberculosis | 9 (3.7) | 0 (0) | 9 (3.7) |
| HIV | 6 (2.4) | 3 (1.2) | 9 (3.7) |
| Psychotic disease | 4 (1.6) | 0 (0) | 4 (1.6) |
| Malignancy | 2 (0.8) | 1 (0.4) | 3 (1.2) |
| Cirrhosis | 2 (0.8) | 0 (0) | 2 (0.8) |
| Emphysema | 2 (0.8) | 0 (0) | 2 (0.8) |
| Hepatitis | 1 (0.4) | 0 (0) | 1 (0.4) |
| Parkinson disease | 1 (0.4) | 0 (0) | 1 (0.4) |
| Poliomyelitis | 1 (0.4) | 0 (0) | 1 (0.4) |
Abbreviation: HIV, human immunodeficiency virus.
Percentages are calculated based on the total.
Features of injuries and pathology in hanging cases
Features of injuries, including injuries caused by the ligature and those caused indirectly to internal organs, are shown in Table 6. Tongue protrusion was found in 45% of cases. Face congestion occurred in 23.8% and petechial hemorrhage of face or conjunctiva in 28.7% of hanging deaths. The neck injuries included neck muscle hemorrhage in 8.6% of cases, thyroid hemorrhage in 2% of cases, intimal tear of carotid artery in 0.8% of cases, hyoid/thyroid bone fracture in 1 case, and vertebral fracture in 1 case. Congestion of internal organs occurred in 57.4% of cases, with similar percentages in men and women. Petechial hemorrhage of internal organs (including pleura, epicardium, pericardium, liver, and spleen) was present in 20.5% of cases. Pulmonary edema was present in 20.5% of cases and brain edema was found in 8.6% of cases, both with higher percentages in women. Hesitation was present in 7% of cases, 12 cases being men and 5 cases being women. Suicide notes were found in 6.1% of cases.
Table 6.
Features of injuries in hanging cases.
| Features of hanging | Male, No. (%) | Female, No. (%) | Total, No. (%) |
|---|---|---|---|
| Tongue protrusion | 90 (36.9) | 22 (9) | 112 (45.9) |
| Congestion of face | 48 (19.7) | 10 (4.1) | 58 (23.8) |
| Petechial hemorrhage of face or conjunctiva | 56 (2.3) | 14 (5.7) | 70 (28.7) |
| Neck muscle hemorrhage | 18 (7.4) | 3 (1.2) | 21 (8.6) |
| Thyroid hemorrhage | 5 (2) | 0 (0) | 5 (2) |
| Intimal tear of carotid artery | 2 (0.8) | 0 (0) | 2 (0.8) |
| Hyoid/thyroid bone fracture | 1 (0.4) | 1 (0.4) | 2 (0.8) |
| Vertebral fracture | 1 (0.4) | 0 (0) | 1 (0.4) |
| Congestion of internal organs | 113 (46.3) | 27 (11.1) | 140 (57.4) |
| Petechial hemorrhage of internal organs | 41 (16.8) | 9 (3.7) | 50 (20.5) |
| Pulmonary edema | 35 (13.5) | 15 (6.1) | 50 (20.5) |
| Brain edema | 15 (6.1) | 6 (2.4) | 21 (8.6) |
| Hesitation | 12 (4.9) | 5 (2) | 17 (7) |
| Suicide note | 11 (4.5) | 4 (1.6) | 15 (6.1) |
Features of hanging marks in relation to ligature material
The hanging mark around the neck was usually situated above the level of thyroid cartilage for all types of ligature material (Table 7). The direction of the ligature mark was known from the position of the knot. The knot was commonly placed over the back of the neck at the occipital protuberance in 25.5% of cases, but was placed on 1 side in 11.3% of cases and in front in 2 cases. In cases who used fabric, however, the knot was placed on the side of the rope in 7 cases and in the back in 6 cases. It is difficult to compare placement of the knot in relation to ligature material because in 60% of all cases, the site of the knot mark was not found. In cases who used cable, however, marks were not found in 21%, and in 79% of cases where marks were found, it was in the back of the neck in 36.8% of cases and on the side in 3 cases.
Table 7.
Distribution of features of hanging mark in relation to ligature material.
| Features of hanging mark | Rope, No. (%) | Fabric, No. (%) | Belt, No. (%) | Cable, No. (%) | Necktie, No. (%) | Blanket, No. (%) | Bag, No. (%) |
|---|---|---|---|---|---|---|---|
| Level of compression mark | |||||||
| Above thyroid | 146 (98) | 46 (98) | 7 (100) | 18 (95) | 2 (100) | 3 (100) | 4 (100) |
| At level of thyroid | 3 (1.6) | 1 (2.1) | 0 (0) | 1 (5.3) | 0 (0) | 0 (0) | 0 (0) |
| Site of knot mark | |||||||
| Anterior | 2 (1.1) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Back of neck/occiput | 44 (23.7) | 6 (12.8) | 1 (14.3) | 7 (36.8) | 0 (0) | 1 (33) | 0 (0) |
| Right side of neck | 7 (3.8) | 5 (10.6) | 0 (0) | 1 (5.3) | 0 (0) | 1 (33) | 0 (0) |
| Left side of neck | 6 (3.2) | 2 (4.3) | 2 (28.6) | 2 (10.5) | 0 (0) | 0 (0) | 0 (0) |
| Not found | 90 (60.4) | 34 (72.3) | 4 (57.1) | 9 (47.4) | 2 (100) | 1 (33) | 4 (100) |
| Pattern of compression mark | |||||||
| Inverted V shape | 32 (17.2) | 8 (17) | 1 (14.3) | 4 (21.1) | 0 (0) | 1 (33) | 0 (0) |
| Horizontal with minimal upright | 117 (78.5) | 39 (83) | 6 (85.7) | 15 (78) | 2 (100) | 2 (66) | 4 (100) |
| Width of compression mark, cm | |||||||
| <0.5 | 9 (4.8) | 2 (4.3) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| 0.5-0.9 | 35 (18.8) | 2 (4.3) | 1 (14.3) | 6 (31.6) | 0 (0) | 0 (0) | 0 (0) |
| 1-1.9 | 72 (48.3) | 10 (21.3) | 0 (0) | 12 (63.2) | 0 (0) | 0 (0) | 0 (0) |
| 2-2.9 | 28 (15.1) | 15 (31.9) | 1 (14.3) | 1 (5.3) | 2 (100) | 0 (0) | 1 (25) |
| >3 | 5 (2.6) | 18 (38.3) | 5 (71.4) | 0 (0) | 0 (0) | 3 (100) | 3 (75) |
The pattern of the neck compression mark was found to be horizontal with minimal upright for all types of ligature material (78.5% of cases of all rope use, 83% of cases of all fabric use) followed by inverted V-shaped pattern (17.2% of cases of rope use, 17% of cases of fabric use).
The width of compression mark was commonly found to be 1 to 1.9 cm in cases of rope and cable use (48% and 63% of cases, respectively) but greater than 2 cm in cases of fabric use (70% of cases). The mark was found to be greater than 3 cm in the relatively few cases of belt, blanket, and bag use.
Correlation between features of hanging with multiple factors
In 40 cases, the body was suspended with complete hanging, and in 204 cases, there was incomplete or partial hanging (Table 8). Tongue protrusion was found in 83 of 204 cases of partial hanging and in 29 of 40 cases of complete hanging with significant correlation (χ2: 13.63, P < .01). The other external features (congestion of face, petechial hemorrhage of face, or conjunctiva) were also significantly correlated with complete hanging. In addition, the internal features of hanging (neck injuries, petechial hemorrhage of internal organs) were also significantly correlated with complete hanging, except congestion of internal organs and pulmonary and brain edema (Tables 8 and 9).
Table 8.
Correlation between features of hanging with type of hanging.
| Features of hanging | Partial hanging (n = 204) | Complete hanging (n = 40) | P value |
|---|---|---|---|
| Tongue protrusion | 83 | 29 | <.001* |
| Congestion of face | 40 | 18 | <.001* |
| Petechial hemorrhage of face or conjunctiva | 48 | 22 | <.001* |
| Congestion of internal organs | 91 | 13 | .157 |
| Petechial hemorrhage of internal organs | 34 | 16 | <.001* |
| Pulmonary edema | 37 | 11 | .173 |
| Brain edema | 15 | 6 | .115 |
Mean statistical significance P<0.05.
Table 9.
Correlation between neck injury and other factors.
| Factor | Neck injury | No neck injury | Total, No. (%) | P value |
|---|---|---|---|---|
| Type of hanging | ||||
| Complete | 13 | 27 | 40 (16.4) | <.001* |
| Partial | 12 | 192 | 204 (83.6) | |
| Width of compression mark, cm | ||||
| ⩽1 | 12 | 106 | 118 (48.3) | .96 |
| >1 | 13 | 113 | 126 (51.6) | |
| Body weight, kg | ||||
| ⩽60 | 17 | 115 | 132 (54) | .791 |
| >60 | 11 | 83 | 94 (38.5) | |
| Ligature material | ||||
| Rope | 18 | 131 | 149 (61.1) | .654 |
| Not rope | 12 | 73 | 85 (34.8) | |
| Pattern of compression mark | ||||
| Inverted V | 5 | 43 | 48 (19.7) | .873 |
| Horizontal minimal upright | 22 | 174 | 196 (80.3) | |
| Sex | ||||
| Male | 23 | 174 | 197 (71.3) | .534 |
| Female | 4 | 43 | 47 (19.2) | |
Mean statistical significance P<0.05.
Neck injuries found included neck muscle hemorrhage, thyroid hemorrhage, and fracture of neck organs (hyoid/thyroid/vertebra) (Table 9).There was no significant relationship between width of compression mark and presence of neck injury. In addition, other factors, including body weight, ligature material, pattern of compression mark, and sex, also had no significant correlation with neck injury.
Toxicologic and microscopic analysis
Toxicologic analysis was evaluated in 221 (92.1%) of cases of hanging, including 10 decomposed cases. The toxicologic analysis cannot detect intoxicants in 153 (62.7%) decomposed cases. Ethanol was detected in 68 cases (27.9%). Ethanol level ranged between 12 and 416 mg%, with concentration of 151 to 300 mg% in 29 cases (11.9%) of men and more than 300 mg% in 5 (2%) cases of men.
Toxic substance and illegal drugs, such as amphetamine, methamphetamine, pseudoephridrine, and mitragynine, were detected in 35 cases (14.3%) (Table 10). The most common substances were amphetamine/methamphetamine in 13 (5.3%) cases, predominantly men (12 cases), followed by benzodiazepines in 8 cases (3.3%), mostly men (6 cases).
Table 10.
Substance found in specimens according to sex.
| Ethanol level, mg% | Male, No. (%) | Female, No. (%) | Total, No. (%) |
|---|---|---|---|
| 10-50 | 9 (3.7) | 2 (0.8) | 11 (4.5) |
| 51-150 | 17 (7) | 6 (2.5) | 23 (9.4) |
| 151-300 | 25 (10.2) | 4 (1.6) | 29 (11.9) |
| >300 | 5 (2) | 0 (0) | 5 (2) |
| Total | 56 (23) | 12 (4.9) | 68 (27.9) |
| Amphetamine/methamphetamine | 12 (4.9) | 1 (0.4) | 13 (5.3) |
| Benzodiazepine | 6 (2.4) | 2 (0.8) | 8 (3.3) |
| Pseudoephridrine | 3 (1.2) | 0 (0) | 3 (1.2) |
| Methadone | 3 (1.2) | 0 (0) | 3 (1.2) |
| Acetaminophen | 3 (1.2) | 0 (0) | 3 (1.2) |
| Tramadol | 2 (0.8) | 0 (0) | 2 (0.8) |
| Sertraline | 1 (0.4) | 0 (0) | 1 (0.4) |
| Methanol | 1 (0.4) | 0 (0) | 1 (0.4) |
| Mitragynine | 1 (0.4) | 0 (0) | 1 (0.4) |
| Total | 32 (13.1) | 3 (1.2) | 35 (14.3) |
| Negative finding | 122 (50) | 31 (12.7) | 153 (63) |
Percentages are calculated based on the total.
Ethanol was found predominantly in the 20- to 29-year age group (24 of 68 cases), followed by the 30- to 39-year age group and 40- to 49-year age group (20 and 16 cases, respectively). In addition, illegal drugs such as amphetamine, methamphetamine, pseudoephridrine, and mitragynine were detected in all age groups, predominantly in the age group of 20 to 29. Amphetamine/methamphetamine was also found mostly in the 20- to 29-year age group (6 of 13 cases) but was not detected in victims older than 50 years.
Microscopic examination was performed in all cases of hanging deaths. The samples were preserved mostly to confirm the pathologic findings and not for the cause of death.
Discussion
Suicide is one of the leading causes of death in the world. Asia accounts for about 60% of world suicides, with China, India, and Japan accounting for about 40% of world suicides. Bangladesh, China, Hong Kong, Japan, South Korea, Sri Lanka, and Taiwan had relatively higher suicide rates (>13.0/100 000), with Bangladesh having the highest (39.6/100 000). Due to stigmatization and legal sanctions against suicide, underreporting of suicide rates in Muslim countries (such as Iran, Pakistan, Saudi Arabia, and Turkey) may partly contribute to extremely low rate (<6.5/100 000). Thailand had higher suicide rates (7.8/100 000 population) than Muslim countries.8
Suicide methods differ prominently in Western and Asian countries. For example, the use of firearms is the favored suicide method in many Western countries, but not in Asia.6 In contrast, pesticide ingestion, charcoal burning, and self-immolation are all unique leading suicide methods in Asia. Overall, hanging and pesticide poisoning were dominant methods of suicide in Asia and Thailand.3,4,8-10 Certain methods rarely reported in the West were, however, very common in some countries, such as Turkey,11 England and Wales,12 Germany,13 Japan,14 Saudi Arabia,15 and Hungary.16 Hanging constituted 65.6% of all suicides in this study and 58.3% of all suicides in the whole population of Thailand (2001-2005).8,17
In Turkey and Kuala Lumpur, Malaysia, the ranking of common suicide methods had been stable over 1990-2011. In South Korea, the ranking of the leading suicide methods had been consistent, although the proportions of hanging and poisoning increased over the years (1995-2006). The prevalence of suicide varies by region in Thailand and over time has increased during crisis that the country faces. Suicide is most prevalent in Northern Thailand and least prevalent in Southern Thailand. Since the late 1990s, the rate of female suicide by hanging became higher than by self-poisoning. In the period 2001-2005, ingestion of agricultural chemicals took the place of other substance intoxication and became the second leading suicide method. Except for a mild upward fluctuation of suicide rate in 1998-2000 after the Asian financial crisis, suicide rate in Thailand has been relatively stable in 1977-2003. Suicide has historically increased during periods of crisis, such as the 2007 Asian Economic Crisis and during the years when the AIDS epidemic was cutting short many young lives in Thailand. In Singapore and Thailand, even though the composition of suicide methods changed over time, suicide rate remained stable, indicating that patterns of suicide in a country are shaped by multiple factors.9,17,18
Overall, most of the Asian countries had lower male-to-female suicide gender ratios (<2.0) compared with their Western counterparts. These countries included Bahrain, China, Hong Kong, India, South Korea, Philippines, Singapore, and Turkey. China has the lowest suicide gender ratio (0.88 in 1999), whereas Iran (3.0 in 1991), Pakistan (2.9-4.0 in the period 1991-2006), and Thailand (3.2 in 2002) had higher gender ratios compared with Western figures. Japan (2.7 in 2009) and Taiwan (2.1 in 2010) were in the middle range. Suicidal hanging victims in this study were predominantly men (4.1:1). Similarly, in a study in Shanghai,5 the male-to-female ratio of hanging victims was 2.08:1, but contrasts with relatively high incidence of hanging in woman (40% of cases) reported in Denmark by Simondsen19 and those in London, Northern Ireland.20,21 The excess of male cases in suicidal hanging is a common feature in other studies, such as those in Kuwait and Cardiff. In general, men constituted approximately 73% and 60% of these cases, respectively.22,23
We present the data of the hanging victims in the central area of Bangkok, which is representative of urban societies where people experience the high pressures of competition, especially in working ages. Most of the victims were found to be in the 20- to 29-year age group. Victims of hanging tend to be of young working age consistent with the results of Abd-Elwahab Hassan et al22 and Üzün et al.11 As reported by previous studies in Thailand, hanging has been the most common means of suicide for both genders with a higher percentage of men than women. Suicide by hanging was also the most common method across all age groups.9 Violent death is more commonly associated with men.24 In addition, more men suffer from chronic stress, whereas more women experience acute precipitating events. Younger subjects tend to have more acute precipitating events before death, whereas older subjects have reported more chronic stress.25
Nearly all cases in this study (90%) were of Thai nationality, with about half of the cases reported in Bangkok, but they are not necessarily urban residents. In fact, only 36% of victims were Bangkok residents. This is can be explained by the fact that many people from other provinces in Thailand and foreigners from some Asian countries, such as Myanmar, Japan, China, and Laos, migrate to work in Bangkok, and so most of the victims are Bangkok residents, but not much different from countrymen. The common occupations of the hanging victims in this study are employees of service industries and merchants or mangers. These results are similar to a study conducted in Bahrain, an Islamic country in the Gulf, in which the mean suicide rate was higher in Indian migrants.26
The private home or apartment is the most common place for committing suicide by hanging (207 cases, 84.8%).This is probably due to the private environment and easy availability of different ligature materials at home. As reported by an Indian study,27 more than 95% of victims preferred their home for committing suicide by hanging.
As reported by an Indian study,28 incidences of suicide happened most in April and May, and similarly in a Lithuanian study,29 but in our study, about equal numbers of victims were found in winter followed by summer and rainy seasons, but these seasonal differences are minor. The peak incidence was in November. In men, most number of cases was found during the rainy season. However, human behavior could be affected by seasonal variations. This may be due to the fact that the rainy season (June to October) is the longest season according to Thailand climate and bad weather might lead people to miserable and violent behaviors.30 The most common period for hanging was daytime. This may be because hanging victims were usually found during daytime and because the time of death was sometimes recorded as the time the body was found.
Factors increasing the risk of suicide are complex. These include psychiatric, biological, social, and environmental factors, as well as those related to an individual’s life history. Such factors include psychiatric illnesses, alcohol abuse, interpersonal conflicts or broken or disturbed relationships, legal- or work-related problems, and economic hardship.31 In our study, we found a single chronic disease in 12.7% and multiple chronic disease in 3.68%, with peak incidence in tuberculosis and HIV infection, followed by chronic illnesses and psychotic disorders (major depressive disorder and schizophrenia). Tantipiwatanaskul and Visrutratana conducted a study in Chiang Mai, a province with highest reported suicide rates in Thailand, and found that the 5 most common precipitating factors were HIV infection (20%), alcohol-related problems (18.7%), marital discord (17.8%), chronic illnesses (17.8%), and financial problems (15.8%).9 However, more details about the social victim will be beneficial, but this study had the limitation of information about education, police profiles, and prison records of the hanging cases.
One of the strongest risk factors for suicidal behavior is alcohol and illicit substance dependency and abuse.32–34 In Thailand, the upper legal limit of blood alcohol level for driving is 50 mg% because this level can impair decision-making ability. In this study, alcohol was the most common substance present in the hanging victims (68 cases, 27.9%). Eleven cases showed ethanol within the legal limit and 57 cases above the legal limit. Only 18 cases showed positive results for illegal substances in blood and urine samples. Amphetamine and methamphetamines were common drugs, and only 1 case showed mitragynine in the toxicologic reports. Similar to a study in Australia by Darke et al,35 alcohol was the most common substance present in toxicology laboratory findings of suicide hanging cases. In an Iranian36 report, a different result was obtained; morphine was the most common substance found in corpses, whereas ethanol and codeine were in the next rank.36 In accordance with substance found in specimen against age group, it was found that the presence of ethanol and other substance was higher in younger cases, similar to the study by Ranjbar et al.36
In this series, the bodies were decomposed in 12.3% of cases and were unidentified in 1.6% of cases; similar to the study by Ambade et al,37 most of the bodies were undecomposed and identified. The bodies were decomposed in 8.7% of cases and were unidentified in 4.7% of cases.
The ligature material most commonly used in hanging was rope followed by fabric material and cable. Rope and the fabric material, such as clothing, are usually the most easily available ligature material in a household. In an Indian study,37 nylon rope was the most common type of ligature material used for hanging. However, another Indian study by Patel et al38 reported that soft material such as cloth followed by firm material such as rope were the preferred choices.
In this study, incomplete hanging cases predominated complete hanging, in contrast to an Egyptian study by Saisudheer and Nagaraja,39 but in an Indian study, Sharma et al40 found 46% complete and 54% partial hanging cases.
The hanging mark was typically present above the thyroid cartilage, as in the study of Ambade et al.37 In all ligature materials, the knot mark was commonly over the back of the neck or occiput (25.5%), and typical hanging mark (inverted V pattern) was found in 20% of cases. The knot was on one side (right side) of the neck in 11%. These findings are consistent with those reported in India by Sharma et al,40 Ambade et al,37 and another study from Thailand by Worawat et al.41 The width of compression mark was commonly found to be 1 to 1.9 cm with rope use, but more than 3 cm in cases of fabric and belt use, and the compression mark was commonly found to be 0.6 to 3.5 cm.
Regarding external pathologic findings, which include unspecific signs of asphyxia as reported by Ambade et al,37 facial congestion was present in about 40% of cases and petechiae in 26% of hanging deaths. The Spanish study by Suarez-Penaranda et al42 found congestion of face in 42.9% and petechial hemorrhage in 23.4% of cases. This is generally consistent with our study, and these findings are significantly associated with complete hanging compared with incomplete hanging, in contrast to some authors who have found such signs more frequent in partial hanging.43,44 Studies in Canada and United States by Clement et al45 and Luke et al,46 respectively, noted a significantly higher incidence of petechial hemorrhage in partial suspension compared with complete hanging. However, in the Spanish study, Suarez-Penaranda et al42 did not find any correlation between facial congestion and petechial hemorrhage with the type of suspension.
Hanging produces asphyxia due to constriction of the neck by the ligature. It happens as a result of suspension in such a manner that the weight of the body, or a part of it, pulls upon the ligature.47 Weight ranges for hanging of men in different body positions are presented: in the standing posture, the ligature is stretched by more than 65% of the body weight; in kneeling position by 64% to 74%; in sitting by 17% to 32%; and in recumbent posture by less than 18% of the body weight.48 In our study, most victims were hanging in standing position, and body weight ranged from 38 to 87 kg with peak incidence at 60 to 69 kg, followed by 50 to 59 kg, consistent with Worawat et al.41
Regarding neck injuries, the percentage of neck muscle injuries ranged from 20% to 34% and was not related to the location of the ligature knot or the type of hanging. The ligature pressure on the muscle is contralateral in relation to the knot, whereas the traction of muscle is ipsilateral in relation to the knot. The analysis showed that the frequency of the neck muscle injuries was related to the width of the ligature, which could be explained by the ligature pressure on the muscle. The ligature pressure is inversely proportional to the width of the ligature mark.49
Tension force is also a factor in neck injuries. As explained by the Newton law, tension is the reaction force applied by a stretched ligature material which acts upward against the downward gravitational force on the object. In other words, the tension force is directly proportional to the weight of the body. In contrast, this study found a result similar to that of Worawat et al,41 in which neck muscle injuries are not significantly associated with the weight of victims and the width of the ligature mark. Our study also found there was no significant association with the type of ligature material and pattern of neck compression. There was a significant association between neck injury and complete hanging due to the greater tension force and pressure on the neck in complete hanging victims, but the width of the ligature mark or body weight is not a major factor in producing neck injuries. This is consistent with the findings of Abd-Elwahab Hassan et al, who found more neck injuries (fracture in the neck) in complete hanging victims than in partial hanging cases.
Tongue protrusion was detected in partial hanging in 83 of 204 cases and in complete hanging in 29 of 40 cases, with a significant association with complete hanging, in contrast to another study from Thailand.41
Neck injuries were more common in men, probably due to greater body weight, but not significantly so, as in the case of the Spanish study.42 Neck injuries in this study include neck muscle hemorrhage in 8.6% of cases, similar to the Egyptian study by Saisudheer and Nagaraja39 and a study in the United States by Luke et al46 who found neck muscle hemorrhage in 28% and 24.5% of cases, respectively. Thyroid hemorrhage were found in only 2% of cases, but Luke et al46 reported thyroid gland hemorrhage in 37.7% of hanging deaths.
Regarding the neck fracture, our study found hyoid/thyroid bone fracture in 0.8% of cases, a low number compared with the study by Dixit et al,50 who noted hyoid fractures in 14% and thyroid cartilage in 15% hanging deaths. In this study, vertebral fracture was found in only 1 (0.4%) case, similar to Ambade et al,37 who found cervical vertebra fracture was seen in 0.8% of cases. Regarding internal organ pathologies in this study, petechial hemorrhages of internal organs were significantly more prevalent in complete hanging, in contrast to the study by Elfawal and Awad51 in which petechial hemorrhage of internal organs occurred in 78.7% of cases, more commonly in cases of partial hanging without statistical analysis.
Conclusions
Hanging is the most common method of committing suicide in most countries in Asia, including Thailand. This study is only part of samples of hanging cases in Central Bangkok which is a specific characteristic of urban area. However, the patterns, ligature material, and contributing factors vary between societies, and this information might be important part for the government and public health policy to reduce risk of suicides and suicide prevention. In Thailand, the police and doctors or forensic pathologist are responsible for assessing whether the deaths are suicide or homicide. This report shows the pathologies of hanging and the significant number of strategic data of neck injuries which are associated with complete hanging, which differ from other studies. Because this could help to improve the diagnostic accuracy of hangings in central Bangkok and other cities, it is important to conduct further studies at other centers.
Footnotes
Peer review:Five peer reviewers contributed to the peer review report. Reviewers’ reports totaled 1213 words, excluding any confidential comments to the academic editor.
Funding:The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions: Study conception and design: NT, VP. Acquisition of data: SP. Analysis and interpretation of data: NT, SP. Drafting of manuscript: NT, VP. Critical revision: NT, VP.
Ethical Clearance: The analyses in this report have been approved by the Ethical Clearance Committee on Human Rights Related to Research Involving Human Subjects, Faculty of Medicine, Ramathibodi Hospital, Mahidol University (MURA 2015/113).
References
- 1. Reddy KSN. The Essentials of Forensic Medicine and Toxicology. 29th ed. Medical: book Coy. K Suguna Dev; 2010:296–297. [Google Scholar]
- 2. DiMaio VJ. Homicidal asphyxia. Am J Forensic Med Pathol. 2000;21:1–4. [DOI] [PubMed] [Google Scholar]
- 3. Peonim V, Sujirachato K, Srisont S, Udnoon J, Worasuwannarak W. Committed suicide: Forensic autopsy analysis at Ramathibodi hospital during year 2001–2010. J Med Assoc (Thai). 2014;97:662–668. [PubMed] [Google Scholar]
- 4. Kolpe DV. An analysis of suicidal hanging cases. J Med Educ Res. 2011;1:23–25. [Google Scholar]
- 5. He M, Fang Y-X, Lin J-Y, Ma K-J, Li B-X. Unnatural death in Shanghai from 2000 to 2009: a retrospective study of forensic autopsy cases at the Shanghai public security Bureau. PLoS ONE. 2015;10:e0131309. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Nandy A. Principle of Forensic Medicine Including Toxicology. 3rd ed. New Delhi, India: Central Book Agency; 2010:517–518. [Google Scholar]
- 7. Kanchan T, Menezes RG. Suicidal hanging in Manipal, South India—victim profile and gender differences. J Forensic Leg Med. 2008;15:493e6. [DOI] [PubMed] [Google Scholar]
- 8. Kevin CCW, Ying YC, Paul SFY. Suicide methods in Asia: implications in suicide prevention. Int J Environ Res Public Health. 2012;9:1135–1158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Tantipiwatanaskul P, Visrutratana S. Suicide: An Investigation and Prevention. Bangkok, Thailand: Department of Mental health; 1998. (in Thai). [Google Scholar]
- 10. Cheng AT, Lee CS. Suicide in Asia and the Far East. In: Hawton K, Van Heeringen K. eds. The International Handbook of Suicide and Attempted Suicide. Chichester, UK: John Wiley & Sons; 2000:29–48. [Google Scholar]
- 11. Uzun I, Buyuk Y, Gurpinar K. Suicidal hanging: fatalities in Istanbul retrospective analysis of 761 autopsy cases. J Forensic Leg Med. 2007;14:406–409. [DOI] [PubMed] [Google Scholar]
- 12. Brock A, Griffiths C. Trends in suicide by method in England and Wales 1979–2001. Health Stat Q. 2003;20:7–18. [Google Scholar]
- 13. Wiesner C. Suicidal methods: a comparison between East and West Germany. Epidemiological, forensic and sociomedical aspects. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz. 2004;47:1095–1106. [DOI] [PubMed] [Google Scholar]
- 14. Ojima T, Nakamura Y, Detels R. Comparative study about methods of suicide between Japan and the United States. J Epidemiol. 2004;19:823–829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Elfawal M. Cultural influence on the incidence and choice of method of suicide in Saudi Arabia. Am J Forensic Med Pathol. 1999;20:163–168. [DOI] [PubMed] [Google Scholar]
- 16. Jegesy A, Harsanyi L, Angyal M. A detailed study on suicides in Baranya County (Hungary). Int J Legal Med. 1995;108:150–153. [DOI] [PubMed] [Google Scholar]
- 17. Lotrakul M. Thailand. Suicide in Asia: Causes and Prevention, ed. Yip PSF. Hong Kong, China: Hong Kong University Press; 2008:81–100. [Google Scholar]
- 18. Thomyangkoon P, Leenaars AA, Wasserman D. Suicide in Thailand, 1977 to 2002. Arch Suicide Res. 2005;9:361–368. [DOI] [PubMed] [Google Scholar]
- 19. Simonsen J. Patho-anatomic findings in neck structures in asphyxiation due to hanging: a survey of 80 cases. Forensic Sci Int. 1988;38:83–91. [DOI] [PubMed] [Google Scholar]
- 20. Bowen DA. Hanging: a review. Forensic Sci Int. 1982;20:247–249. [DOI] [PubMed] [Google Scholar]
- 21. Davison A, Marshall TK. Hanging in Northern Ireland: a survey. Med Sci Law. 1986;26:23–28. [DOI] [PubMed] [Google Scholar]
- 22. Abd-Elwahab Hassan D, Ghaleb SS, Kotb H, Agamy M, Kharoshah M. Suicidal hanging in Kuwait: retrospective analysis of cases from 2010 to 2012. J Forensic Leg Med. 20:2013;1118–1121. [DOI] [PubMed] [Google Scholar]
- 23. James R, Silcocks P. Suicidal hanging in Cardiff: a 15 year retrospective study. Forensic Sci Int. 1992;56:167–175. [DOI] [PubMed] [Google Scholar]
- 24. Byard RW, Klitte A, Gilbert JD. Changing patterns of female suicide: 1986–2000. J Clin Forensic Med. 2004;11:123–128. [DOI] [PubMed] [Google Scholar]
- 25. Prasad J, Abraham VJ, Minz S, et al. Rates and factors associated with suicide in Kaniyambadi Block, Tamil Nadu, South India, 2000–2002. Int J Soc Psychiatry. 2006;52:65–71. [DOI] [PubMed] [Google Scholar]
- 26. Ahmed A, Randah HR, Mazin AK, Adel E. Suicide in Bahrain in the last decade. Crisis. 2007;28:11–15. [DOI] [PubMed] [Google Scholar]
- 27. Vijayakumari N. Suicidal hanging: a prospective study. J Indian Forensic Sci. 2011;33:355–357. [Google Scholar]
- 28. Ambade VN, Godbole HV, Kukde HG. Suicidal and homicidal deaths: a comparative and circumstantial approach. J Forensic Leg Med. 2007;14:253–260. [DOI] [PubMed] [Google Scholar]
- 29. Kalediene R, Starkuviene S, Petrauskiene J. Seasonal patterns of suicides over the period of socio-economic transition in Lithuania. BMC Public Health. 2006;6:40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Gunpolicy.org. Guns in Thailand: facts, figures and firearm law. http://www.gunpolicy.org/firearms/region/thailand. Updated October 29, 2013.
- 31. Mgaya E, Kazaura MR, Outwater A, Kinabo L. Suicide in the Dar es Salaam region, Tanzania, 2005. J Forensic Leg Med. 2008;15:172–176. [DOI] [PubMed] [Google Scholar]
- 32. Trémeau F, Darreye A, Staner L, et al. Suicidality in opioid-dependent subjects. Am J Addict. 2008;17:187–194. [DOI] [PubMed] [Google Scholar]
- 33. Wilcox HC, Conner KR, Caine ED. Association of alcohol and drug use disorders and completed suicide: an empirical review of cohort studies. Drug Alcohol Depend. 2004;76:S11–S19. [DOI] [PubMed] [Google Scholar]
- 34. Mostafazadeh B, Farzaneh E. Risks and risk factors of repeated suicidal attempt: study on unconscious poisoned patients. Asia Pac J Med Toxicol. 2012;2:28–31. [Google Scholar]
- 35. Darke S, Duflou J, Torok M. Toxicology and circumstances of completed suicide by means other than overdose. J Forensic Sci. 2009;54:490–494. [DOI] [PubMed] [Google Scholar]
- 36. Ranjbar MR, Liaghat AR, Ranlbar A, et al. Toxicologic findings in hanging death. Asia Pac J Med Toxicol (APJMT). 2013;2(3). http://apjmt.mums.ac.ir (accessed September 2013). [Google Scholar]
- 37. Ambade VN, Kolpe D, Tumram N, et al. Study of hanging deaths in Central India. J Forensic Sci. 2015;60(5):1216–1223. [DOI] [PubMed] [Google Scholar]
- 38. Patel AP, Bansal A, Sheikh IV, Sheikh KA. Study of hanging cases in Ahmedabad region. J Indian Forensic Sci. 2012;34:342–345. [Google Scholar]
- 39. Saisudheer T, Nagaraja TV. A study of ligature mark in cases of hanging deaths. Int J Pharm Biomed. 2012;3:80–84. [Google Scholar]
- 40. Sharma BR, Singh VP, Harish D. Neck structure injuries in hanging: comparing retrospective and prospective. Med Sci Law. 2005;45:321–330. [DOI] [PubMed] [Google Scholar]
- 41. Worawat A, Wongchanapai W, Thamtakerngkit S. Factors affecting neck injuries in hanging deaths. J Forensic Phys Assoc. 2008;2:23–32. [Google Scholar]
- 42. Suarez-Penaranda JM, Alvarez T, Miguens X, et al. Characterization of lesions in hanging deaths. J Forensic Sci. 2008;53:720–723. [DOI] [PubMed] [Google Scholar]
- 43. Spitz WU. ed. Spitz and Fisher’s Medicolegal Investigation of Death. 3rd ed. Springfield, IL: Charles C Thomas Publisher; 1993:444–497. [Google Scholar]
- 44. Di Maio V, DiMaio DJ. Forensic Pathology. New York, NY: CRC Press; 2001:229–277. [Google Scholar]
- 45. Clement R, Guay JP, Redpath M, Sauvageau A. Petechiae in hanging: a retrospective study of contributing variables. Am J Forensic Med Pathol. 2011;32:378–382. [DOI] [PubMed] [Google Scholar]
- 46. Luke JL, Reay DT, Eisele JW, Bonnell HJ. Correlation of circumstances with pathological findings in asphyxial deaths by hanging: a prospective study of 61 cases from Seattle, WA. J Forensic Sci. 1985;30:1140–1147. [PubMed] [Google Scholar]
- 47. Polson CJ, Gee DJ, Knight B. The Essentials of Forensic Medicine. 4th ed. London, England: Pergamon Press; 1985:357–388. [Google Scholar]
- 48. Khokhlov VD. Calculation of tension exerted on a ligature in incomplete hanging. Forensic Sci Int 2001;123:172–177. [DOI] [PubMed] [Google Scholar]
- 49. Nikolic S, Micic J, Atanasijevic T, Djokic V, Djonic D. Analysis of neck injuries in hanging. Am J Forensic Med Pathol. 2003;24:179–182. [DOI] [PubMed] [Google Scholar]
- 50. Dixit PG, Mohite PM, Ambade VN. Study of histopathological changes in thyroid, salivary gland and lymph nodes in hanging. J Forensic Med Toxicol. 2001;18:1–4. [Google Scholar]
- 51. Elfawal M, Awad O. Deaths from hanging in the Eastern Province of Saudi Arabia. Med Sci Law. 1994;34:307–312. [DOI] [PubMed] [Google Scholar]