

Abstract
Background
Non-invasive measures that can accurately estimate cardiac output may help identify volume-responsive patients. This study seeks to compare two non-invasive measures (corrected carotid flow time and carotid blood flow) and their correlations with invasive reference measurements of cardiac output. Consenting adult patients (n = 51) at Massachusetts General Hospital cardiac catheterization laboratory undergoing right heart catheterization between February and April 2016 were included. Carotid ultrasound images were obtained concurrently with cardiac output measurements, obtained by the thermodilution method in the absence of severe tricuspid regurgitation and by the Fick oxygen method otherwise. Corrected carotid flow time was calculated as systole time/√cycle time. Carotid blood flow was calculated as π × (carotid diameter)2/4 × velocity time integral × heart rate. Measurements were obtained using a single carotid waveform and an average of three carotid waveforms for both measures.
Results
Single waveform measurements of corrected flow time did not correlate with cardiac output (ρ = 0.25, 95% CI −0.03 to 0.49, p = 0.08), but an average of three waveforms correlated significantly, although weakly (ρ = 0.29, 95% CI 0.02–0.53, p = 0.046). Carotid blood flow measurements correlated moderately with cardiac output regardless of if single waveform or an average of three waveforms were used: ρ = 0.44, 95% CI 0.18–0.63, p = 0.004, and ρ = 0.41, 95% CI 0.16–0.62, p = 0.004, respectively.
Conclusions
Carotid blood flow may be a better marker of cardiac output and less subject to measurements issues than corrected carotid flow time.
Electronic supplementary material
The online version of this article (doi:10.1186/s13089-017-0065-0) contains supplementary material, which is available to authorized users.
Keywords: Cardiac output, Carotid ultrasound, Carotid flow time, Carotid blood flow
Background
To be able to identify patients who are fluid responsive is important in the management of those who are acutely ill. At present, there is no non-invasive method that can reliably and accurately identify fluid responsiveness. As such, in patients with undifferentiated shock, treatment often involves empiric fluid administration, in the hopes that volume expansion will increase preload, which will then serve to increase cardiac output (CO). However, for patients on the flat portion of the Starling curve, aggressive fluid administration results in no appreciable increase in CO and may be detrimental [1–3]. Thus, the ability to identify where each patient is on his/her Starling curve can help identify patients who would benefit from additional fluid (fluid responsive) and those who would not (fluid unresponsive). Unfortunately, traditional measures of preload such as central venous pressure have not consistently been shown to be helpful in identifying volume responsiveness [4, 5]. The use of pulse pressure variation shows promise in ventilated patients, but requires the insertion of an arterial line [5]. As such, there remains a pressing need to be able to identify fluid responsiveness non-invasively at the bedside.
Fluid responsiveness is typically defined as an increase in CO by 10–15% in response to fluid administration [6]. To avoid excess fluid administration, an increase of CO in response to maneuvers such as the passive leg raise (PLR) is considered indicative of fluid responsiveness [7]. PLR is typically performed with the patient either in the supine or semirecumbent position, followed by repeat measurements with the patient’s legs passively raised at 30–45° [7]. This maneuver is considered to result in an auto-bolus of fluid of approximately 300 mL in volume [8]. The benefit of the PLR is that its hemodynamic effects are rapidly reversible, since no fluid administration actually takes place.
Cardiac output, however, has been challenging to measure at the bedside. The traditional reference standard for measuring CO requires the insertion of a pulmonary artery catheter [5, 9] which is invasive, associated with a risk for serious complications [10], and its use may offer no clinical benefits [11–15]. Newer non-invasive devices using bioreactance parameters have mixed evidence in their accuracy and reliability [16–20], and require a dedicated machine that may not be readily available. Lastly, estimations of CO using echocardiography have been suggested as a bedside measure. However, its use may not be feasible due to high training requirements [21].
In the quest to identify feasible, non-invasive, and reproducible bedside estimates of CO, carotid Doppler imaging shows promise. In particular, two carotid measurements have emerged as candidate markers of CO: corrected carotid flow time (CFT) and carotid blood flow (CBF). CFT is the carotid systole time, with heart rate correction applied. This measure is easy to perform and may correlate with intravascular volume [22]. CBF is the integral of blood volume that is ejected through the carotid artery with each cardiac cycle. This measure has been shown to be feasible to perform at the bedside [23, 24].
Studies to date have shown that corrected CFT increases in response to fluid administration or consumption [25, 26], and decreases in response to volume removal in dialysis [22] and blood donation [27]. However, none of these studies correlated corrected CFT with CO. CBF has been less extensively studied. However, in one study of 34 patients, a change in CBF in response to PLR was found to correlate significantly with a change in stroke volume index, measured by bioreactance [28].
Despite these promising studies, neither measure has been correlated directly with a commonly used invasive reference standard for measuring CO via the pulmonary artery catheter. As such, this study seeks to compare corrected CFT and CBF with invasive measures of CO.
Methods
All adult patients at Massachusetts General Hospital cardiac catheterization laboratory undergoing right heart catheterization between February and April 2016 were invited to participate. Non-consenting patients, patients on mechanical ventilation, and those unable to tolerate a passive leg raise (PLR) maneuver were excluded (e.g., unable to lie supine or had pain with PLR).
Carotid ultrasound images were obtained concurrently with CO measures with the patient in the supine position. A PLR was then performed by elevating the legs using a standardized 30° foam wedge (RayShield® AADCO Medical Inc., Vermont). Repeat carotid ultrasound images and concurrent CO measurements were then obtained within 1 min after PLR, as maximal blood flow changes were felt to be observed within 1 min [8, 29].
Carotid ultrasound images were obtained by an emergency ultrasound fellow (I.M.). Images were obtained using a linear-array (15–4 MHz) transducer on a bedside ultrasound system (uSmart® Terason 3200T, Burlington, MA). The carotid vascular preset was used (pulse repetition frequency 5.0 kHz, wall filter 75 Hz). The common carotid artery was scanned in transverse and longitudinal planes. Spectral Doppler tracings were then obtained by placing a 0.5 mm sample gate through the center of vessel, within 2–3 cm proximal to the carotid bulb in the longitudinal plane, in accordance to standard guidelines [30]. The angle correction cursor was placed parallel to the direction of blood flow. Images with insonation angles >60° were excluded because of resultant inaccuracies of flow and velocity measurements at such angles [31].
Carotid measurements
Corrected CFT was calculated as systole time/√cycle time [27]. Systole time was measured from the start of systolic upstroke to the start of the dicrotic notch, while cycle time was the duration of the cycle (Fig. 1a).
Fig. 1.
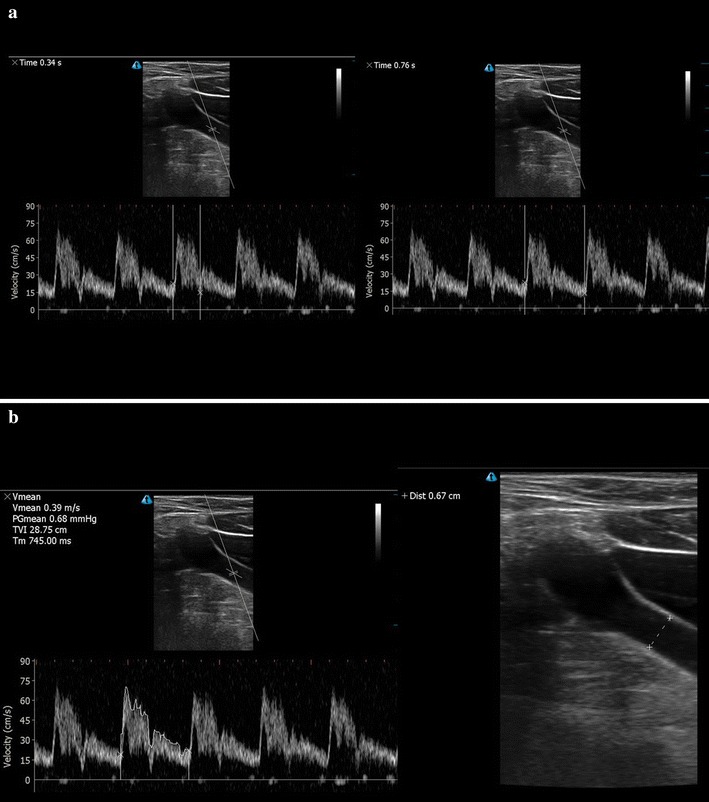
a Carotid systole time, as measured from the start of the systolic upstroke to the start of the dicrotic notch (left). Carotid cycle time, as measured from start of one systolic upstroke to the next (right). b Velocity time integral tracing of the spectral Doppler signal (left). Carotid diameter (right)
CBF was calculated as
where VTI indicates velocity time integral [28]. VTI of the Doppler signal was measured using manual tracings (Fig. 1b). Intimal-to-intimal carotid diameter was measured at the level of the sample gate (Fig. 1b).
All carotid measurements (systole time, cycle time, VTI, diameter) were measured on a single waveform by one investigator (I.M.) in order to calculate corrected CFT and CBF. Average corrected CFT and average CBF were then calculated using a mean of three waveforms. To establish interrater reliability on obtaining measurements, all measurements on obtained images were then repeated by a second independent investigator (C.W. or A.A., both with similar training to I.M.), who was blinded to all CO and carotid measurements. Results from the second investigator were used only to provide interrater reliability estimates.
Image acceptability was rated independently by two trained raters (C.W., A.A.), using five domains (internal reliability acceptable, Cronbach’s alpha = 0.84): correction angle parallel to vessel, sample gate in the center of the vessel, sufficient gain, vessel was non-oblique, and measurements made within 2–3 cm proximal to carotid bulb (see Additional file 1). All domains were rated using a 5-point Likert scale, where 1 = poor quality and 5 = excellent quality, with overall image quality rated as a summary measure, based on global expert opinion.
Cardiac output measurements were obtained by thermodilution method in the absence of severe tricuspid regurgitation, by an injection of 10 mL of sterile 0.9% saline injection into the proximal lumen of the pulmonary artery catheter and subsequent detection of the temperature change at the distal thermistor [32]. Fick oxygen method was used in the presence of severe tricuspid regurgitation [33]. The Fick method involved simultaneous arterial and mixed venous blood sample measurement, and cardiac output was determined based upon the ratio between estimated oxygen consumption and arteriovenous oxygen gradient [34]. Post hoc analyses of correlation measures were performed in subgroups of patients in and not in atrial fibrillation at the time of the procedure.
This study was approved by the Partners Human Research Committee Institution Review Board.
Statistical analysis
On the basis of Marik et al.’s prior study on estimates of stroke volume indices correlations with carotid blood flow [28], we estimated that 26 patients would have 90% power to detect a correlation of 0.59 (α = 0.05). However, as interim analyses revealed a lower than 0.59 correlation in our study sample. A repeat sample size calculation suggested that an estimated 48 patients would be needed to detect a correlation of 0.45 (α = 0.05, power = 0.9).
Pre- and post-PLR measurements were compared using paired t tests and Wilcoxon signed-rank tests, as appropriate. Correlations between CO and carotid parameters were made using Spearman’s rho, a non-parametric correlation coefficient. Confidence intervals around Spearman’s rho were based on Fisher’s r to z transformation [35]. Correlation coefficients of 0.10–0.29 were considered weak, 0.30–0.49 as moderate, and 0.50–1.00 as strong [36]. All p values were adjusted for multiple comparisons using the Benjamini–Hochberg procedure [37], which allows the false discovery rate to be controlled at the 0.05 level.
All analyses were performed using SAS 9.4 (SAS Institute Inc. Cary, NC) and SPSS version 24 (IBM Corp. Armonk, NY).
Results
Of the 67 eligible patients, 51 patients (76%) were included in the final analysis (Fig. 2; Table 1). The majority of patients had cardiac output measurements done using thermodilution (n = 44; 86%). Five patients were excluded because of angles of insonation of >60°. Of the included 51 patients, median angle of insonation was 60°, with a range of 38–60°. Overall image quality of the included patients was rated as above-average quality [mean score 4.1 ± standard deviation (SD) 0.6] based on global expert opinion. As there were no differences in CO, corrected CFT, or CBF between pre- and post-PLR maneuver (Table 2), only baseline measures (i.e., pre-PLR) will be further discussed. Interrater reliability for corrected CFT and CBF measurements on obtained images was excellent [intraclass correlation coefficient (ICC) 0.90, 95% CI 0.82–0.94; ICC 0.96, 95% CI 0.58–0.99, respectively].
Fig. 2.
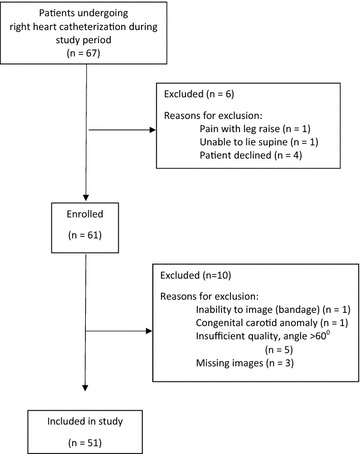
Flow chart of number of patients enrolled in the study and included in the analyses
Table 1.
Baseline characteristics of 51 patients included in the study
| Baseline characteristics | Number (%) |
|---|---|
| Mean age in years ± standard deviation | 59.6 ± 16.3 |
| Gender | |
| Male | 39 (76) |
| Female | 12 (24) |
| Body mass index (kg/m2) ± standard deviation | 26.3 ± 5.9 |
| History of | |
| Diabetes mellitus | 13 (25) |
| Hypertension | 26 (51) |
| Dyslipidemia | 22 (43) |
| Coronary artery disease | 17 (33) |
| Prior angioplasty and/stent placement | 7 (14) |
| Prior coronary bypass surgery | 4 (8) |
| Stroke or transient ischemic attacks | 11 (22) |
| Atrial fibrillation | 13 (25) |
| Moderate or severe aortic insufficiency | 1 (2) |
| Moderate or severe aortic stenosis | 5 (10) |
| Indication for right heart catheterization | |
| Diagnostic right heart catheterization only | 24 (47) |
| Cardiac biopsy | 27 (53) |
| Cardiac output measurement method | |
| Thermodilution | 44 (86) |
| Fick oxygen method | 7 (14) |
| Vascular access | |
| Internal jugular | 40 (78) |
| Forearm (cephalic or basilic) | 5 (10) |
| Femoral | 6 (12) |
Table 2.
Baseline mean cardiac output and median carotid ultrasound parameters (corrected flow time and blood flow) pre- and post-passive leg raise
| Parameter | Pre-passive leg raise median (interquartile range) | Post-passive leg raise median (interquartile range) | p value |
|---|---|---|---|
| Mean cardiac output ± standard deviation (SD) (L/min) | 5.15 ± 1.58 | 5.19 ± 1.58 | 0.69 |
| Corrected flow time (single waveform in milliseconds) | 331.7 (308.6–357.8) | 344.2 (321.6–360.6) | 0.06 |
| Corrected flow time (average of three waveforms in milliseconds) | 335.2 (311.0–359.3) | 339.6 (322.1–368.9) | 0.13 |
| Blood flow (single waveform in mL/min) | 576.3 (389.5–806.9) | 551.77 (441.5–763.5) | 0.45 |
| Blood flow (average of three waveforms in mL/min) | 555.4 (422.1–766.6) | 558.3 (452.7–741.6) | 0.45 |
Corrected carotid flow time (CFT)
Single waveform measurements of corrected CFT did not correlate with CO measurements [ρ = 0.25, 95% confidence interval (CI) −0.03 to 0.49, adjusted p = 0.08]. Corrected CFT measurements using three waveforms correlated significantly, but weakly, with CO (ρ = 0.29, 95% CI 0.02–0.53, adjusted p = 0.046).
Carotid blood flow (CBF)
Single waveform CBF correlated moderately and significantly with CO [ρ = 0.44, 95% CI 0.18–0.63, adjusted p = 0.004). CBF measurements using three waveforms also moderately and significantly correlated with CO (ρ = 0.41, 95% CI 0.16–0.62, adjusted p = 0.004).
Subgroup analysis
In a subgroup of patients not in atrial fibrillation at the time of the procedure (n = 45), single waveform measurements of corrected CFT did not correlate with CO (ρ = 0.26, 95% CI −0.04 to 0.51, adjusted p = 0.17). For patients in atrial fibrillation at the time of the procedure (n = 6), single waveform corrected CFT measurements did not correlate with CO (ρ = 0.09, 95% CI −0.78 to 0.84, adjusted p = 0.88). In patients not in atrial fibrillation (n = 45), corrected CFT measurements using three waveforms correlated moderately and significantly with CO (ρ = 0.33, 95% CI 0.04–0.56, adjusted p = 0.03). In patients in atrial fibrillation (n = 6), corrected CFT measurements using three waveforms did not correlate with CO (ρ = −0.14, 95% CI −0.86 to 0.76, adjusted p = 0.92).
Single waveform measurements of CBF correlated moderately and significantly with CO in patients not in atrial fibrillation at the time of the procedure (ρ = 0.42, 95% CI 0.15–0.64, adjusted p = 0.03). For the six patients in atrial fibrillation, single waveform measurements did not correlate with CO (ρ = 0.66, 95% CI −0.33 to 0.96, adjusted p = 0.28). In patients not in atrial fibrillation (n = 45), CBF measurements using three waveforms correlated moderately and significantly with CO (ρ = 0.40, 95% CI 0.12–0.62, adjusted p = 0.02). For the six patients in atrial fibrillation at the time of the procedure, CBF measurements using three waveforms did not correlate with CO (ρ = 0.60, 95% CI −0.41 to 0.95, adjusted p = 0.31).
Self-report feasibility
Overall, reported ease of carotid diameter measurement was high (mean score 4.1 ± SD 0.8, where 1 = very difficult and 5 = very easy). Reported ease of measuring VTI tracings was moderate (mean score 3.5 ± SD 0.8). Ease of systole time was moderate (3.7 ± SD 0.8) and high for cycle time (4.2 ± SD 0.7).
Discussion
In this study of 51 adult patients undergoing invasive right heart catheterization and simultaneous carotid ultrasound, CBF correlated moderately and significantly with CO. This relationship was present whether a single waveform or an average of three waveforms was used. Corrected CFT, on the other hand, when measured using only a single waveform, as per the method used by prior studies [22, 25–27], demonstrated no correlation with CO. Only by measuring three waveforms was corrected carotid flow time’s correlation with CO significant. However, the strength of this relationship was weak. Altogether, our findings suggest CBF may be a better surrogate marker for CO and that CBF measurements may be less subject to measurements issues than corrected CFT.
The ability to estimate CO in an accurate, reliable, and feasible manner is an important part of determining patients’ volume responsiveness. Carotid ultrasound is a promising tool for two reasons. First, unlike the traditional reference standard of CO measurement from a pulmonary artery catheter [5, 9], carotid ultrasound imaging is non-invasive and readily available in many centers. Second, as evidenced by reported ease of measurements in our study, and confirmed by prior studies [23, 24], carotid ultrasound is easy to perform. This is in contrast to echocardiographic measures of CO [21], which requires more extensive training [38], as its accuracy is dependent on scan techniques and patient factors such as obesity and availability of sonographic windows [39].
In deciding whether to use corrected CFT or CBF as an estimate of CO, one should consider the following factors: (1) strength of the correlation with reference standard, (2) contextual factors that may limit its accuracy, (3) reliability, (4) feasibility, and (5) sensitivity in detecting CO changes. We argue that CBF is superior for the first two factors, and that both CBF and corrected CFT demonstrated high interrater reliability and feasibility.
To our knowledge, ours is the first study to compare both carotid ultrasound measures with invasive measures of CO. Our study demonstrates that CBF correlates stronger than corrected CFT with CO and is less sensitive to measurements errors. We hypothesize that two sources of errors may be contributing to measurement errors in corrected CFT: cardiac arrhythmia and underlying cardiac conditions.
With respect to the cardiac arrhythmia hypothesis, we noted that corrected CFT measurements based on averaging three waveforms yielded a higher and significant correlation, compared to measurements based only on one waveform. The potential of respiratory contribution to the variations in cycle time and systole time (sinus arrhythmia) may contribute to this finding. The hypothesis regarding the contribution of arrhythmias to inaccurate measurements was further supported by findings from our subgroup analysis, whereby the correlation of corrected CFT with CO became significant in a subgroup of patients not in atrial fibrillation at the time of the procedure, and only if an average of three waveforms were used. Correlations were lower in general for patients in atrial fibrillation compared with those not in atrial fibrillation, whether a single waveform or three waveforms were used. Indeed, prior studies evaluating corrected carotid flow time excluded patients with atrial fibrillation [22, 25–27]. In our subgroup analysis of patients in atrial fibrillation, we were unable to detect significant correlations with cardiac output measurement regardless of whether CBF or corrected CFT was used, and regardless of whether a single waveform or an average of three waveforms was used. However, our small sample size (n = 6) is likely too small to demonstrate a significant correlation. Future studies should evaluate the use of these parameters in patients in atrial fibrillation. Until such studies are performed, it may be prudent to continue to exclude patients with significant cardiac arrhythmia when attempting to use carotid measurements as surrogates for CO.
With respect to the cardiac condition hypothesis, it is noteworthy that measurements of systole time require the identification of the start of the dicrotic notch. Valvular diseases are known to affect carotid tracings, which may render the dicrotic notch more difficult to appreciate [40–42]. Indeed, in our study, self-report ease of measuring cycle time was higher than for systole time, which may be a reflection of the difficulty in identifying the dicrotic notch in certain cases. Carotid blood flow, on the other hand, utilizes more clinical parameters (diameter, VTI, and heart rate) that may be less subject to the changes of any single parameter and may therefore more accurately estimate for the volumetric flow of blood through the carotid. For example, adaptation to a lower VTI may be accommodated by a larger carotid diameter and/or a faster heart rate. Therefore, accounting for these additional parameters may result in an overall more accurate estimate.
There are a number of limitations in our study. First, this is a single-centered study. Second, we are able to report only interrater reliability for image interpretation and not for image acquisition (a single sonographer performed all the scanning). Image acquisition by untrained sonographers may potentially result in unacceptable interrater reliability. Future studies should examine image acquisition interrater reliability and the role of training. Third, as our patients were largely euvolemic, PLR maneuvers resulted in no demonstrable changes in any of our measured parameters. Therefore, we cannot comment on the sensitivity of carotid measurements to changes imposed by dynamic maneuvers. Further, our use of a 30° foam wedge rather than the more commonly used 45° leg lift [7] may have further limited our ability to induce significant changes pre- and post-PLR. In addition, although it has been argued that the maximal blood flow changes occur within one minute [8, 29], the majority of studies evaluating PLR use a longer time frame [7]. The optimal timing remains unclear. Fourth, our subgroup analysis of patients in and not in atrial fibrillation was performed in a post hoc manner. Results from these analyses should be considered as hypothesis generating only. Fifth, our carotid VTI measurements were performed manually. Therefore, measurement errors may be present. However, measurement errors would be expected to dilute correlation coefficients towards the null [43]. Because many machines are equipped with automatic VTI tracings, correlation coefficients for CBF measured in an automated manner may yield higher correlations than those reported in our study. Sixth, we do not have information on the history of carotid disease. Therefore, we are unable to determine the impact of carotid disease on the accuracy of our carotid ultrasound measurements. Last but not least, the majority of our patients underwent the thermodilution method for cardiac output estimation. While its use is commonly accepted as the practical gold standard, its use is not without limitations, especially in the presence of significant tricuspid regurgitation, intracardiac shunts, or concurrent intravenous infusions [9, 44, 45].
Conclusions
Our study demonstrates that compared to corrected CFT, CBF demonstrated stronger and more consistent correlation with CO. Its use for assessing volume responsiveness should be further evaluated.
Authors’ contributions
IWYM contributed to conception and design, acquisition of data, analysis, interpretation of data, and drafting and revision of article. JDC, AA, CW, and MAF contributed to acquisition of data and interpretation of data and revision of article. AB and ASL contributed to conception and design, interpretation of data, and revision of article. VEN contributed to conception and design, acquisition of data, interpretation of data, and drafting and revision of article. All authors have provided final approval of the version submitted. All authors read and approved the final manuscript.
Acknowledgements
The authors would like to thank all the colleagues and patients at the Massachusetts General Hospital cardiac catheterization laboratory for their collaboration and participation in this work.
Competing interests
The authors declare that they have no competing interests.
Availability of data and materials
The datasets generated and/or analyzed in this study are not currently publicly available but are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
This study was approved by the Partners Human Research Committee Institution Review Board (protocol # 2015P002076/MGH).
Funding
Dr. Irene W. Y. Ma was funded by the University of Calgary Research and Scholarship Leave Grant. The funder has no role in the design and conduct of this study; in the collection, management, analysis, and interpretation of the data; or in the preparation, review, and approval of the manuscript.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abbreviations
- CBF
carotid blood flow
- CFT
carotid flow time
- CO
cardiac output
- CI
confidence interval
- ICC
intraclass correlation coefficient
- PLR
passive leg raise
- SD
standard deviation
- VTI
velocity time integral
Additional file
Additional file 1. Carotid artery doppler quality assessment tool (CADQAD).
Contributor Information
Irene W. Y. Ma, Phone: 403-210-7369, Email: ima@ucalgary.ca
Joshua D. Caplin, Email: JCAPLIN1@mgh.harvard.edu
Aftab Azad, Email: aftabazad@outlook.com.
Christina Wilson, Email: christinanwilson@gmail.com.
Michael A. Fifer, Email: Fifer.Michael@mgh.harvard.edu
Aranya Bagchi, Email: ABAGCHI@mgh.harvard.edu.
Andrew S. Liteplo, Email: ALITEPLO@PARTNERS.ORG
Vicki E. Noble, Email: Vicki.Noble@UHhospitals.org
References
- 1.Kelm DJ, Perrin JT, Cartin-Ceba R, Gajic O, Schenck L, Kennedy CC. Fluid overload in patients with severe sepsis and septic shock treated with early-goal directed therapy is associated with increased acute need for fluid-related medical interventions and hospital death. Shock. 2015;43:68–73. doi: 10.1097/SHK.0000000000000268. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Boyd JH, Forbes J, Nakada TA, Walley KR, Russell JA. Fluid resuscitation in septic shock: a positive fluid balance and elevated central venous pressure are associated with increased mortality. Crit Care Med. 2011;39:259–265. doi: 10.1097/CCM.0b013e3181feeb15. [DOI] [PubMed] [Google Scholar]
- 3.Acheampong A, Vincent J-L. A positive fluid balance is an independent prognostic factor in patients with sepsis. Crit Care. 2015;19:251. doi: 10.1186/s13054-015-0970-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Marik PE, Cavallazzi R. Does the central venous pressure predict fluid responsiveness? An updated meta-analysis and a plea for some common sense. Crit Care Med. 2013;41:1774–1781. doi: 10.1097/CCM.0b013e31828a25fd. [DOI] [PubMed] [Google Scholar]
- 5.Bentzer P, Griesdale DE, Boyd J, MacLean K, Sirounis D, Ayas NT. WIll this hemodynamically unstable patient respond to a bolus of intravenous fluids? JAMA. 2016;316:1298–1309. doi: 10.1001/jama.2016.12310. [DOI] [PubMed] [Google Scholar]
- 6.Bendjelid K, Romand JA. Fluid responsiveness in mechanically ventilated patients: a review of indices used in intensive care. Intensive Care Med. 2012;29:352–360. doi: 10.1007/s00134-002-1615-9. [DOI] [PubMed] [Google Scholar]
- 7.Cavallaro F, Sandroni C, Marano C, La Torre G, Mannocci A, De Waure C, Bello G, Maviglia R, Antonelli M. Diagnostic accuracy of passive leg raising for prediction of fluid responsiveness in adults: systematic review and meta-analysis of clinical studies. Intensive Care Med. 2012;36(9):1476–1483. doi: 10.1007/s00134-010-1929-y. [DOI] [PubMed] [Google Scholar]
- 8.Monnet X, Teboul JL. Passive leg raising: five rules, not a drop of fluid! Crit Care. 2015;19:18. doi: 10.1186/s13054-014-0708-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Pugsley J, Lerner AB. Cardiac output monitoring: is there a gold standard and how do the newer technologies compare? Semin Cardiothorac Vasc Anesth. 2010;14:274–282. doi: 10.1177/1089253210386386. [DOI] [PubMed] [Google Scholar]
- 10.Dee Boyd K, Thomas SJ, Gold J, Boyd AD. A prospective study of complications of pulmonary artery catheterizations in 500 consecutive patients. Chest. 1983;84:245–249. doi: 10.1378/chest.84.3.245. [DOI] [PubMed] [Google Scholar]
- 11.Harvey S, Harrison DA, Singer M, Ashcroft J, Jones CM, Elbourne D, Brampton W, Williams D, Young D, Rowan K. Assessment of the clinical effectiveness of pulmonary artery catheters in management of patients in intensive care (PAC-Man): a randomised controlled trial. Lancet. 2005;366:472–477. doi: 10.1016/S0140-6736(05)67061-4. [DOI] [PubMed] [Google Scholar]
- 12.Sandham JD, Hull RD, Brant RF, Knox L, Pineo GF, Doig CJ, Laporta DP, Viner S, Passerini L, Devitt H, Kirby A, Jacka M. A Randomized, controlled trial of the use of pulmonary-artery catheters in high-risk surgical patients. N Engl J Med. 2003;348:5–14. doi: 10.1056/NEJMoa021108. [DOI] [PubMed] [Google Scholar]
- 13.Richard C, Warszawski J, Anguel N, Deye N, Combes A, Barnoud D, Boulain T, Lefort Y, Fartoukh M, Baud F. Early use of the pulmonary artery catheter and outcomes in patients with shock and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2003;290:2713–2720. doi: 10.1001/jama.290.20.2713. [DOI] [PubMed] [Google Scholar]
- 14.Shah MR, Hasselblad V, Stevenson LW, Binanay C, O’Connor CM, Sopko G, Califf RM. Impact of the pulmonary artery catheter in critically ill patients: meta-analysis of randomized clinical trials. JAMA. 2005;294:1664–1670. doi: 10.1001/jama.294.13.1664. [DOI] [PubMed] [Google Scholar]
- 15.Wheeler A, Bernard G, Thompson B, Schoenfeld D, Wiedemann H, DeBoisblanc B, Connors A, Jr, Hite R, Harabin A. Pulmonary-artery versus central venous catheter to guide treatment of acute lung injury. N Engl J Med. 2006;354:2213–2224. doi: 10.1056/NEJMoa061895. [DOI] [PubMed] [Google Scholar]
- 16.Benomar B, Ouattara A, Estagnasie P, Brusset A, Squara P. Fluid responsiveness predicted by noninvasive bioreactance-based passive leg raise test. Intensive Care Med. 2010;36:1875–1881. doi: 10.1007/s00134-010-1990-6. [DOI] [PubMed] [Google Scholar]
- 17.Fagnoul D, Vincent J-L, Backer D. Cardiac output measurements using the bioreactance technique in critically ill patients. Crit Care. 2012;16:460. doi: 10.1186/cc11067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Raval NY, Squara P, Cleman M, Yalamanchili K, Winklmaier M, Burkhoff D. Multicenter evaluation of noninvasive cardiac output measurement by bioreactance technique. J Clin Monit Comput. 2008;22:113–119. doi: 10.1007/s10877-008-9112-5. [DOI] [PubMed] [Google Scholar]
- 19.Squara P, Denjean D, Estagnasie P, Brusset A, Dib JC, Dubois C. Noninvasive cardiac output monitoring (NICOM): a clinical validation. Intensive Care Med. 2007;33:1191–1194. doi: 10.1007/s00134-007-0640-0. [DOI] [PubMed] [Google Scholar]
- 20.Kupersztych-Hagege E, Teboul JL, Artigas A, Talbot A, Sabatier C, Richard C, Monnet X. Bioreactance is not reliable for estimating cardiac output and the effects of passive leg raising in critically ill patients. Br J Anaesth. 2013;111:961–966. doi: 10.1093/bja/aet282. [DOI] [PubMed] [Google Scholar]
- 21.Gunst M, Ghaemmaghami V, Sperry J, Robinson M, O’Keeffe T, Friese R, Frankel H. Accuracy of cardiac function and volume status estimates using the bedside echocardiographic assessment in trauma/critical care. J Trauma. 2008;65:509–516. doi: 10.1097/TA.0b013e3181825bc5. [DOI] [PubMed] [Google Scholar]
- 22.Hossein-Nejad H, Mohammadinejad P, Lessan-Pezeshki M, Davarani SS, Banaie M. Carotid artery corrected flow time measurement via bedside ultrasonography in monitoring volume status. J Crit Care. 2015;30:1199–1203. doi: 10.1016/j.jcrc.2015.08.014. [DOI] [PubMed] [Google Scholar]
- 23.Stolz LA, Mosier JM, Gross AM, Douglas MJ, Blaivas M, Adhikari S. Can emergency physicians perform common carotid Doppler flow measurements to assess volume responsiveness? W J Emerg Med. 2015;16:255–259. doi: 10.5811/westjem.2015.1.24301. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Adedipe AA, Fly DL, Schwitz SD, Jorgenson DB, Duric H, Sayre MR, Nichol G. Carotid Doppler blood flow measurement during cardiopulmonary resuscitation is feasible: a first in man study. Resuscitation. 2015;96:121–125. doi: 10.1016/j.resuscitation.2015.07.024. [DOI] [PubMed] [Google Scholar]
- 25.Blehar DJ, Glazier S, Gaspari RJ. Correlation of corrected flow time in the carotid artery with changes in intravascular volume status. J Crit Care. 2014;29:486–488. doi: 10.1016/j.jcrc.2014.03.025. [DOI] [PubMed] [Google Scholar]
- 26.Shokoohi H, Berry GW, Shahkolahi M, King J, Salimian M, Poshtmashad A, Pourmand A. The diagnostic utility of sonographic carotid flow time in determining volume responsiveness. J Crit Care. 2016;38:231–235. doi: 10.1016/j.jcrc.2016.10.025. [DOI] [PubMed] [Google Scholar]
- 27.Mackenzie DC, Khan NA, Blehar D, Glazier S, Chang Y, Stowell CP, Noble VE, Liteplo AS. Carotid flow time changes with volume status in acute blood loss. Ann Emerg Med. 2015;66:277–282. doi: 10.1016/j.annemergmed.2015.04.014. [DOI] [PubMed] [Google Scholar]
- 28.Marik PE, Levitov A, Young A, Andrews L. The use of bioreactance and carotid doppler to determine volume responsiveness and blood flow redistribution following passive leg raising in hemodynamically unstable patients. Chest. 2013;143:364–370. doi: 10.1378/chest.12-1274. [DOI] [PubMed] [Google Scholar]
- 29.Monnet X, Rienzo M, Osman D, Anguel N, Richard C, Pinsky MR, Teboul JL. Passive leg raising predicts fluid responsiveness in the critically ill. Crit Care Med. 2006;34:1402–1407. doi: 10.1097/01.CCM.0000215453.11735.06. [DOI] [PubMed] [Google Scholar]
- 30.American College of Radiology (2016) ACR-AIUM-SRU practice parameter for the performance of an ultrasound examination of the extracranial cerebrovascular system. http://www.acr.org/~/media/5d63a45f7a54417c93cd58f109f0fdd2.pdf. Accessed 5 Apr 2017 [DOI] [PubMed]
- 31.Tola M, Yurdakul M. Effect of Doppler angle in diagnosis of internal carotid artery stenosis. J Ultrasound Med. 2006;25:1187–1192. doi: 10.7863/jum.2006.25.9.1187. [DOI] [PubMed] [Google Scholar]
- 32.Ganz W, Donoso R, Marcus HS, Forrester JS, Swan HJ. A new technique for measurement of cardiac output by thermodilution in man. Am J Cardiol. 1971;27:392–396. doi: 10.1016/0002-9149(71)90436-X. [DOI] [PubMed] [Google Scholar]
- 33.Callan P, Clark AL. Right heart catheterisation: indications and interpretation. Heart. 2016;102:147–157. doi: 10.1136/heartjnl-2015-307786. [DOI] [PubMed] [Google Scholar]
- 34.Wilkinson JL. Haemodynamic calculations in the catheter laboratory. Heart. 2001;85:113–120. doi: 10.1136/heart.85.1.113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Shen D, Lu Z (2006) Computation of correlation coefficient and its confidence interval in SAS. http://www2.sas.com/proceedings/sugi31/170-31.pdf. Accessed 5 Apr 2017
- 36.Cohen J. Statistical power analysis for the behavioral sciences. New York: Academic Press; 1988. [Google Scholar]
- 37.Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc B Methodol. 1995;57:289–300. [Google Scholar]
- 38.Garcia X, Mateu L, Maynar J, Mercadal J, Ochagavía A, Ferrandiz A. Estimating cardiac output. Utility in the clinical practice. Available invasive and non-invasive monitoring. Med Intensiva. 2011;35:552–561. doi: 10.1016/j.medin.2011.01.014. [DOI] [PubMed] [Google Scholar]
- 39.Nicolosi GL, Pungercic E, Cervesato E, Pavan D, Modena L, Moro E, Dall’Aglio V, Zanuttini D. Feasibility and variability of six methods for the echocardiographic and Doppler determination of cardiac output. Br Heart J. 1988;59:299–303. doi: 10.1136/hrt.59.3.299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Madhwal S, Yesenko S, Kim ESH, Park M, Begelman SM, Gornik HL. Manifestations of cardiac disease in carotid Duplex ultrasound examination. JACC. 2014;7:200–203. doi: 10.1016/j.jcmg.2013.09.015. [DOI] [PubMed] [Google Scholar]
- 41.O’Boyle MK, Vibhakar NI, Chung J, Keen WD, Gosink BB. Duplex sonography of the carotid arteries in patients with isolated aortic stenosis: imaging findings and relation to severity of stenosis. AJR Am J Roentgenol. 1996;166:197–202. doi: 10.2214/ajr.166.1.8571875. [DOI] [PubMed] [Google Scholar]
- 42.Kallman C, Gosink B, Gardner D. Carotid duplex sonography: bisferious pulse contour in patients with aortic valvular disease. AJR Am J Roentgenol. 1991;157:403–407. doi: 10.2214/ajr.157.2.1853828. [DOI] [PubMed] [Google Scholar]
- 43.Kelsey JL, Whittemore AS, Evans AS, Thompson WD. Methods in observational epidemiology. New York: Oxford University Press Inc; 1996. [Google Scholar]
- 44.Lee AJ, Cohn JH. Ranasinghe JS (2011) Cardiac output assessed by invasive and minimally invasive techniques. Anesthesiol Res Pract. 2011;17:475151. doi: 10.1155/2011/475151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Marino PL. The ICU Bok. 4. Philadelphia: Lippincott Williams & Wilkins; 2014. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and/or analyzed in this study are not currently publicly available but are available from the corresponding author on reasonable request.