

Abstract
Objectives:
The main objective of the study was to identify the most frequent isolates from female outpatients with urinary tract infection.
Material and methods:
The retrospective study was performed at the Department of Microbiology, Parasitology and Virology Faculty of Medicine, University of Sarajevo in period of 2015. The most frequent isolates were determined in 405 first urine samples from female outpatients of Hrasno community in Sarajevo, B&H. Identification of isolates was performed by the standard microbiological testing and the standard methods of descriptive statistics as well.
Results:
E. coli was identified with the frequency of (67.21%), followed by Proteus spp. (9.83%), Enterococcus faecalis (7.37%) and Enterobacter (5.73%). Pseudomonas aeruginosa and Pseudomonas spp. were found in (2.45%), while the frequency of Klebsiella spp., Streptococcus spp. and Acinetobacter spp. was lower (1.63%).
Conclusions:
The isolated strains of E. coli pointed the highest frequency among female outpatients of Hrasno community.
Keywords: Urinary tract infection, UTI, E. coli, isolates
1. INTRODUCTION
Urinary tract infections (UTIs) present microbial colonization of urine and infections of the lower and upper urinary tract. UTIs are among the most common bacterial infections of adulthood. They pose a major public health problem, due to the growing phenomenon of bacterial resistance to a wide range of antibiotics (1). The most common cause of these infections is bacteria. Enterobacteriaceae are causing more than 70% of UTIs, and among them the most important is Escherichia coli, found in 80% of cases (2). The family is ubiquity in the environment and animal hosts and it is very easy to acquire and transfer genetic determinants that confer resistance to most classes of antibiotics. E. coli is one of the most extensively researched Gram- negative bacteria in microbiology.
With an incidence of 12%, UTIs are the most common in female population within all age groups, where the incidence increases with age and peaks in the twenties (3). Within one year, 11% of female reported an UTI, while more than half of the female population has it at least once in their lives. Most UTI cases have been reported for children, elderly people and immunocompromised patients as well. A combination of various risk factors represent the most plausible cause, including physiological and anatomical changes, an active sex life, age, and the close proximity of the urethra, vagina, and rectum in women. In the period of 2009-2013, cystitis was recorded as one of the leading infection in the working population in Bosnia and Herzegovina with a trend of increasing rates (4).
Urinary tract represents a sterile space with the exception of the distal urethra which is colonized by saprophyte microbiota of the surrounding region therefore a urine sample obtained by urinating is not considered a primary sterile sample. Once the infection is present in a bladder, bacteria easily proliferate and reach high concentrations in the urine which supports their growth. The microorganisms can reach the urinary tract by blood circulation or the lymphatic expansion, but there is plenty of clinical and experimental evidence to show that the rise of microorganisms from the urethra is the most common way that leads to UTI, especially bacteria of intestinal origin (E. coli and other Enterobacteriaceae) (5). Haematogenous UTI is limited to a number of microorganisms, such as Staphylococcus aureus, Candida spp., Salmonella spp. and Mycobacterium tuberculosis, which cause primary infection elsewhere in the body. The concept of bacterial virulence in the urinary tract leads to the conclusion that not all bacterial species are capable of causing infection. The more endangered natural defence mechanisms (obstruction or bladder catheterization), the lower levels of bacterial virulence are needed to cause infection. The pathogenesis of UTI is complex; it is influenced by many biological and behavioral factors of the host, as well as nature of uropathogens. The most common cause of UTI is bacteria, while occasionally fungi and viruses could be detected as well. Escherichia coli strains are the most common isolate, founded in 80%of the urine samples of patients with a simple UTI (cystitis), followed by Staphylococcus saprophyticus (5-15%), whereas Klebsiella, Enterobacter or Proteus rarely cause infection outside the hospital (5- 10%) (6). UTI acquired in hospitals are usually caused by these species and Candida spp., while E. coli accounts for only 35-50% (7). The aim of the study was to describe the most frequent UTI isolates collected from female outpatients.
2. METHODS
Clinical samples for this study were obtained in 2015 at the Department of Microbiology, Parasitology and Virologyfrom all outpatients showing symptoms of UTI and referred for urine culture by attending clinician. A total of 405 urine samples were screened by CLSI standards (Clinical and Laboratory Standards Institute) at female outpatients of Hrasno community in Sarajevo.
The gold standard for the urine analysis is urine culture, with identification of pathogens, quantification and testing of sensitivity/resistance. For analysis we took a midstream of first morning urine (urine that was at least 4 hours in the bladder). The obvious drawback of this technique, bacterial contamination when urine is passing through the distal urethra is minimized by the cleaning of the skin and mucous membranes around the opening of the urethra before urination, omitting the first part of the flow of urine, and the collection of midstream urine. This method is simple, non-invasive, low-cost and no risk of complications. Colonies from urine samples collected in this way are correlated with those collected by suprapubic puncture or catheterization (8). Inoculation for urine culture was done on a MacConkey II Agar (the basis for the differentiation of Enterobacteriaceae), and CLED (Cysteine lactose electrolyte deficient) agar, where 1-10 colonies / plate, means that in 1 ml of the tested urine there is <103 bacteria; 10-100 colonies / plate, 1 ml of the tested urine has between 103-104 bacteria; 100-1000 colonies / plate, 1 ml of the tested urine has between 104-105 bacteria; > 1000 colonies / plate, in 1 ml of tested urine there is more than 105 bacteria. The primary isolates were inoculated into Muller-Hinton agar plates with antibiotic discs and incubated for 18-24h at 37°C. The results break points were interpreted according to Clinical and Laboratory Standards Institute guidelines (9).
Results were analyzed using the SPSS computer program for statistical analysis (SPSS Statistical Package for Social Sciences) version 16.0. and computer program Excel (Microsoft Office Excel 2007). Results are presented in tables and graphs as absolute numbers (N) and the percentage values (%). To determine the statistical significance we used Fisher’s exact test. Values of p < 0.05 were considered statistically significant.
3. RESULTS
During Among 492 patients, 70.53% were female (N=347) while male were 29.47% (N=145). There was a statistically significant difference (p <0.05) in favor of female.
Out of total number of urine samples that belonged to female (N=405), 30.12% (N = 122) were positive (they contained a bacteria), while other 69.88% (N=283) were negative (sterile). From samples that belonged to male, 14.57% (N= 22) were positive and the remaining 85.43% (N=129) were negative. There was a statistically significant difference in the positivity of urine culture in favor of female (p <0.05).
Figure 1.
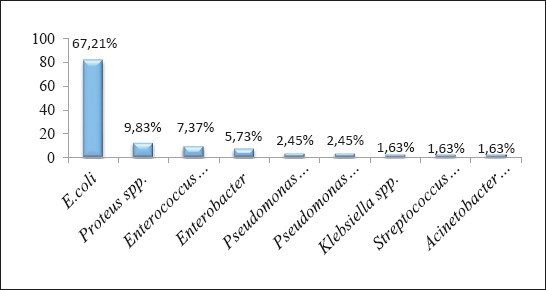
The incidence of the most frequent isolates in female outpatients
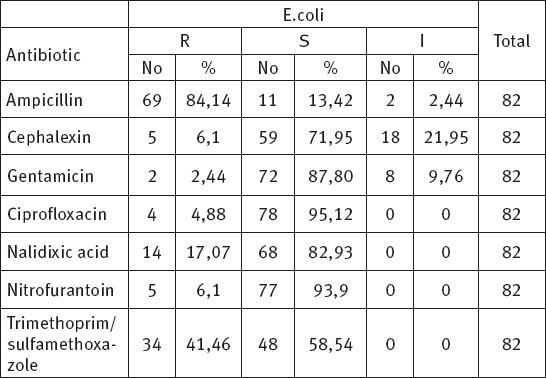
Table 1.
The results of antimicrobial susceptibility / resistance of isolated strains of E. coli in the test of the female population
In the urine cultures of samples that we took from female the most common isolate was E. coli occurred at a frequency of 67.21% (N = 82), followed by Proteus spp., with a incidence of 9.83% (N = 12), Enterococcus faecalis with an incidence of 7.37% (N = 9) and Enterobacter 5.73% (N = 7). Pseudomonas aeruginosa and Pseudomonas spp. were present in 3 (2.45%) urine cultures, while the frequency of Klebsiella spp., Streptococcus spp. and Acinetobacter spp. was 1.63% (2). There was a statistically significantly higher incidence of E. coli isolates as compared to other bacteria (p <0.05).
Within 82 positive urine culture, E. coli strains have shown the highest resistance to ampicillin (N=69, 84.14 %), trimethoprim/sulfamethoxazole (N=34, 41.46 %) and nalidixic acid (N=14, 17.07 %). The greatest susceptibility E. coli strains have shown to ciprofloxacin (N=78, 95.12 %), gentamicin (N=72, 87.80%) and nalidixic acid (N=68, 82.93%).
4. DISCUSSION
The most common bacterial infections in female outpatients are urinary tract infections. The inappropriate use of antibiotics and consequently increased incidence of antimicrobial resistance leads to many complications and it is prolonging the problem of UTI. This results in an extremely negative impact on the quality of life of the patients, and represents a significant financial implications. Urinary tract infections are a major public health problem worldwide with an estimates of 150 million cases per year (10). In Croatia, in 2009 and 2010, primary health care registered about 260.000 diagnosed cystitis (10-11) while pyelonephritis was registered 22.000 times (12). Acute uncomplicated pyelonephritis is much less frequent than cystitis (estimated ratio, 1 case of pyelonephritis in 28 cases of cystitis), with the peak of the annual incidence of 25 cases per 10.000 female 15-34 years of age. In Bosnia and Herzegovina, in the period from 2009 to 2013, cystitis is marked as one of the leading diseases in the working population, with a trend of increasing rates of disease (4).
With an incidence of 12% of female and 3% in male, urinary tract infections are still the most common in female and in all age groups. In primary health care 50% to 80% of women, with typical symptoms, have UTI (13).
According to our study of the total number of samples, the percentage referring to females is significantly higher (72.84%) compared to male samples. This data supports the high incidence of infections in female compared to male, which is confirmed by many studies. ARESC (Antimicrobial Resistance Epidemiological Survey on Cystitis) is an international study to explore the prevalence and sensitivity of pathogens that cause cystitis, conducted in nine European countries and Brazil, in the period from 2003 to 2006 (14).
Limited and predictable range of microorganisms is causing urinary tract infections in young, healthy female. Among ambulatory and hospitalized patients, E. coli is the primary pathogen in urinary tract and makes up 75-90% of the isolates in uncomplicated UTI (15).
Out of 122 isolates tested at the female outpatients, E. coli is isolated even in 82 samples, making it the most common cause of UTI. A similar result was obtained in a study conducted at the Urology Clinic, Clinical Center of Sarajevo, in the period from 2009 to 2011, as well as the General hospital Gracanica in which the most common isolate was E. coli (76.6 %) (16). At the Clinic for Infectious Diseases “Dr Fran Mihaljevic” in Zagreb, in the period of 2010 - 2014 years, E. coli is the leading cause of urinary tract infections. Isolation of E. coli as the most usual cause correlates with studies conducted in around the world (17). According to ARESC study, E. coli was the most common isolate (76.7%), followed by Enterococcus faecalis (4%), Staphylococcus saprophyticus (3.6%), Klebsiella pneumoniae (3.5%), and Proteus mirabilis (3, 5%). In France, as part ARESC studies, the percentage of isolated E. coli is 83.8%. In a study conducted at the outpatient population, which included 1.000 urine samples, the most dominant cause of UTI was E. coli with a prevalence of 66.7% (18). Presense of E.coli in UTI is a constant for a long time, and with it’s trend of increasing resistance to different groups of antibiotics, the treatment becomes more challenging. The increasing presence of resistant strains, in combination with a variety of virulent factors, makes E. coli the most dominant cause of UTI. After E. coli, according to our study, the most common isolates in the female population are Proteus spp., Enterococcus faecalis, Enterobacter, Pseudomonas spp., and Klebsiella spp., which represents a range of bacteria which, with small differences, makes most common isolates worldwide.
In ARESC study, after E. coli the most common isolate was also Enterococcus faecalis, Staphylococcus saprophyticus, Proteus mirabilis and Klebsiella pneumoniae (17). A study conducted at the Clinic for Infectious Diseases in Tuzla, as the most common causes of urinary tract infections other than E. coli and Klebsiella spp. were Proteus mirabilis, Pseudomonas aeruginosa and Enterococcus faecalis. Identifying bacterial species as the etiologic agents of urinary tract infections in observed female outpatient population, and in comparison with the studies in the US and worldwide, follows that the most common isolates are E. coli, Proteus spp., Enterococcus faecalis, Klebsiella spp., Pseudomonas spp.
It is essential to maintain the safety and feasibility of empirical therapy, as a strategy for managing urinary tract infections in female. This can be achieved by constant supervision and knowledge of the most common bacterial species as the etiologic agents of urinary tract infections, as well as their resistance profile (19).
5. CONCLUSION
The study found that E. coli is the most common pathogen in urine culture within female outpatients, with an incidence of 67.21%. In addition to E. coli, according to this study, the most frequent isolates in the female was Proteus spp. (9.83%), Enterococcus faecalis (7.73%) and Enterobacter (5.73%). Pseudomonas aeruginosa, Pseudomonas spp., Klebsiella spp., Streptococcus spp., and Acinetobacter spp. were detected with low frequency. Our research also has shown that the E. coli strains has shown the highest resistance to ampicillin, and the highest susceptibility to ciprofloxacin..
Footnotes
• Author’s contribution: Nadira Zatric and Velma Rebic - collecting data of patients. Mufida Aljicevic- collection of literature on antibiotic resistance. Amila Abduzaimovic–preparing data in Excel Sheet.
• Declaration of Interest: There is no conflict of interest.
REFERENCES
- 1.Grabe M, Bartoletti R, Bjerklund Johansen TE, Cai T, Çek M, Köves B, et al. European Association of Urology: Guidelines on Urological Infections [Online] 2015. [[cited 2015 Feb]]. Available from: http://uroweb.org/wp-content/uploads/19-Urological-infections_LR2.pdf .
- 2.Uzunović-Kamberović S. Medicinska mikrobiologija. I izd ed. Zenica: Štamparija Fojnica; 2009. pp. 367–75. [Google Scholar]
- 3.Foxman B. Epidemiology of urinary tract infections: incidence, morbidity, and economic costs. Dis Mon. 2003;49(2):53–70. doi: 10.1067/mda.2003.7. [DOI] [PubMed] [Google Scholar]
- 4.Zdravstveno stanje stanovništva i zdravstvena zaštita u Federaciji Bosne i Hercegovine 2013. godina Sarajevo. 2014:51–3. [Google Scholar]
- 5.Tambic-Andrašević A. Etiologija urogenitalnih infekcija. Medicus: Urogenitalne infekcije - izabrana poglavlja. 2012;21(1):15–21. [Google Scholar]
- 6.Hooton TM. Uncomplicated Urinary Tract Infection. N Engl J Med. 2012;366(11):1028–37. doi: 10.1056/NEJMcp1104429. [DOI] [PubMed] [Google Scholar]
- 7.Mahmutovic Vranic S, Uzunovic A. Antimicrobial resistance of Escherichia coli strains isolated from urine at outpatient population: a single laboratory experience. Mater Sociomed. 2016;28(2):84–7. doi: 10.5455/msm.2016.28.121-124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Schmiemann G, Kniehl E, Gebhardt K, Matejczyk MM, Hummers-Pradier E. The Diagnosis of Urinary Tract Infection. Dtsch Arztebl Int. 2010;107(21):361–7. doi: 10.3238/arztebl.2010.0361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Performance standards for antimicrobial susceptibility test; twenty-first information supplement. CLSI. 2011 Jan [Google Scholar]
- 10.Urology Care Foundation. The official Foundation of the American Urological Association. 2013. Mar, [Cited Februar 2017]. Available from http://www.urologyhealth.org .
- 11.Kuzman A, Znaor A. Javnozdravstvena važnost urogenitalnih i spolno prenosivih infekcija. Medicus: Urogenitalne infekcije - izabrana poglavlja. 2012 Mar;21(1):5–14. [Google Scholar]
- 12.Renard J, Ballarini S, Mascarenhas T, Zahran M, Quimper E, Choucair J, et al. Recurrent Lower Urinary Tract Infections Have a Detrimental Effect on Patient Quality of Life: a Prospective, Observational Study. Infect Dis Ther. 2015 Dec;4(1):125–35. doi: 10.1007/s40121-014-0054-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Schito GC, Naber KG, Botto H, Palou J, Mazzei T, Gualco L, Marchese A. The ARESC study: an international survey on the antimicrobial resistance of pathogens involved in uncomplicated urinary tract infections. Int J Antimicrob Agents. 2009 Nov;34(5):407–13. doi: 10.1016/j.ijantimicag.2009.04.012. [DOI] [PubMed] [Google Scholar]
- 14.Czaja CA, Scholes D, Hooton TM, Stamm WE. Population-based epidemiologic analysis of acute pyelonephritis. Clin Infect Dis. 2007;45(3):273–80. doi: 10.1086/519268. [DOI] [PubMed] [Google Scholar]
- 15.Junuzovic Dz, Zunic L, Dervisefendic M, Skopljak A, Pasagic A, Masic I. The toxic effect on leukocyte lineage of antimicrobial therapy in urinary and respiratory infections. Med Arch. 2014 Jun;68(3):167–9. doi: 10.5455/medarh.2014.68.167-169. doi:10.5455/medarh2014.68.167-169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hodžić S. Analiza kliničko epidemioloških parametara infekcija urinarnog trakta. Rauche. 2013;2 [Google Scholar]
- 17.Ajduković M, Kotarski V, Čeljuska Tošev E. Zagreb: Klinika za infektivne bolesti „Dr. Fran Mihaljević, Zagreb; 2015. Izvješće o radu referentnog centra ministarstva zdravlja za infekcije mokraćnog sustava od 2010 do 2014. godine. [Google Scholar]
- 18.Neuzillet Y, Naber KG, Schito G, Gualco L, Botto H. French results of the ARESC study: clinical aspects and epidemiology of antimicrobial resistance in female patients with cystitis. Implications for empiric therapy. Med Mal Infect. 2012;42(2):66–75. doi: 10.1016/j.medmal.2011.07.005. [DOI] [PubMed] [Google Scholar]
- 19.Abduzaimovic A, Aljicevic M, Rebic V, Vranic S, Abduzaimovic K, Sestic S. Antibiotic Resistance in Urinary Isolates of Escherichia coli. Mater Sociomed. 2016;28(6):416–9. doi: 10.5455/msm.2016.28.416-419. doi:10.5455/msm.2016.28.416-419. [DOI] [PMC free article] [PubMed] [Google Scholar]