

Abstract
Objective:
The aim of this study was to evaluate the anatomy of the nasopalatine canal in a Lebanese population using cone-beam computed tomography (CBCT) technology.
Materials and Methods:
CBCT images of 63 Lebanese adult patients were included in this study. The length, shape, diameter of the oral opening corresponding to the incisive foramen and inclination in relation to the hard palate of the nasopalatine canal were analyzed.
Results:
Of all canals assessed, 13 were hourglass-shaped, 23 were cylindrical-shaped, 23 were funnel-shaped and 4 were spindle-shaped. The mean canal length and the incisive foramen anteroposterior diameter were respectively 11.52 mm and 4.91 mm. The average canal inclination related to the hard palate was 17.09 degrees.
Conclusion:
Within the limits of this study, we conclude that in Lebanese patients, the shape of the nasopalatine canal is variable. No statistical significance was noticed between genders except for the canal length which was found shorter in our female sample.
Keywords: Cone-beam computed tomography, incisive foramen, nasopalatine canal, Lebanese population
1. INTRODUCTION
The nasopalatine canal (NPC) is a passage located in the premaxilla region connecting the hard palate to the nasal floor. Orally, it opens behind the maxillary central incisors as a single foramen called the incisive foramen (IF) while in the nasal cavity its opening is usually in the form of two foramina known as the foramina of Stenson. The NPC delivers passage to the nasopalatine nerve and the sphenopalatine artery whose destination is the anterior part of the palatal region (1).
Anatomic variations of the NPC have been described by many authors; they concern the shape, the length, the IF location and diameter, the number of openings at the nasal fossa, etc. (2, 3, 4).
Difficulties regarding the anatomy of the NPC have been reported during dental and surgical procedures in the premaxilla region such as local anesthesia, maxillary central incisors implant placement, etc. (2). In this respect, good knowledge of the anatomic details of the NPC is essential; consequently, taking benefit of the imaging technological advancement like cone-beam computed tomography (CBCT) may offer more precise evaluation (1, 3, 4).
The aim of this study was to assess the anatomy of the NPC using CBCT data obtained from Lebanese adult population.
2. MATERIAL AND METHODS
In this retrospective study, archived CBCT radiographs of Lebanese adult patients were examined. These radiographs were effectuated at a specialized maxillofacial imaging center for a multiplicity of dental and/or oral indications (e.g., sinus assessment, implant planning, impacted teeth, etc.).
The CBCT scans were acquired using the PaX-Zenith3D© machine (Vatech Co. Ltd., Yongin-Si, Republic of Korea). The technical parameters ranged between 70 to 100 kVp and 7 to 15 mA, with an exposure time of 20 s and medium to large FOVs according to the clinical case, in respect to the “As Low As Reasonably Achievable” (ALARA) principle.
Were excluded from the study the radiographs of patients:(a) younger than 18 year- old; (b) edentulous; and (c) presenting abnormalities in the maxilla.
Sixty-three CBCT images of 21 males and 42 females with an age ranging from 18 to 67 years met the inclusion criteria and were included in the study.
The images were examined by two radiologists having more than ten years of experience.
They considered for the NPC its shape, length, inclination related to the hard palate and the IF anteroposterior diameter.
This process extended over three sessions of approximately twenty cases each. A week period existed between the sessions. To estimate the measurements’ errors, they were repeated by the observers twenty days after the initial readings without having to resort the preliminary results. In the case of any disparity, the mean of the two values was taken.
The observations were made as follow:
The length of the NPC and the IF diameter: The measurement of the mean length of the NPC was made by marking in the sagittal plane the nasal and oral openings of the canal corresponding to its upper and lower limits; the canal was then measured in millimeters from these two limits.
As for the IF diameter, it was also calculated in the sagittal plane by measuring the anteroposterior distance of the oral entrance of the NPC (Figure 1).
The shape of the NPC: Many authors classified the canal shape into categories like cylindrical, funnel, spindle, hourglass, banana, etc. (2, 4).
Figure 1.
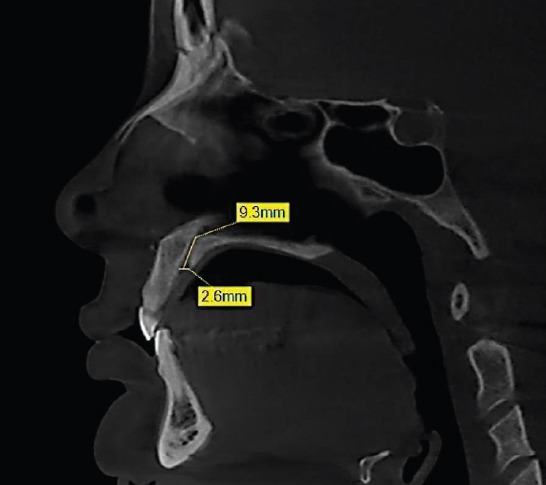
CBCT sagittal cut at the level of the premaxilla illustrating the method of determining the length of the NPC and the IF diameter.
In our study, we opted for the following classification based on the shape seen on the sagittal cuts (Figure 2):
Figure 2.
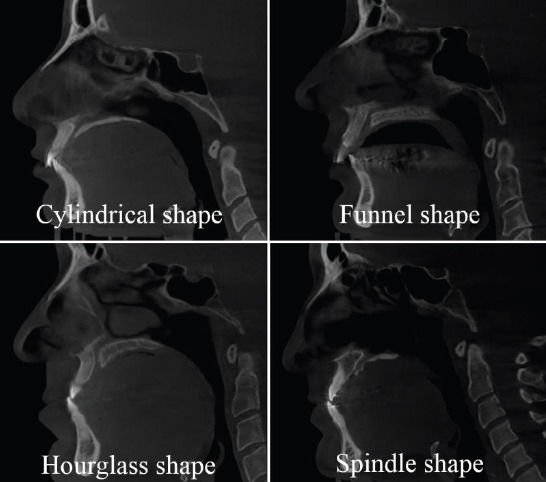
CBCT sagittal cuts at the level of the premaxilla illustrating the method of determining the shape of the NPC.
The cylindrical: when the labial and palatal walls of the canal are parallel.
The funnel: when the anteroposterior dimension of the canal increased from the nasal fossa to the hard palate.
The spindle: when the anteroposterior dimension is widest at the mid-level of the canal compared to the dimensions at the nasal and palatal levels.
The hourglass: when the anteroposterior dimension is narrowest at the mid-level of the canal compared to the dimensions at the nasal and palatal levels.
The inclination of the NPC related to the hard palate: A line was drawn in the middle of the oral and nasal openings of the NPC. The inclination is measured according to a perpendicular line parallel to the hard palate (Figure 3).
Figure 3.
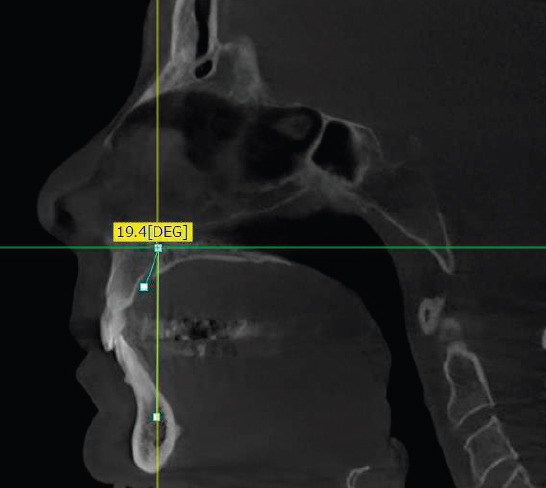
CBCT sagittal cut at the level of the premaxilla illustrating the method of determining the inclination of the NPC; the inclination is measured according to a line parallel to the hard palate.
Descriptive statistics of age and gender of the patients and for the NPC, its length, shape, inclination related to the hard palate and the IF diameter, were done. All statistical analyses were performed using IBM SPSS for Windows version 20.0 (SPSS, Chicago, IL, USA). Statistical significance was set at 0.05.
3. RESULTS
The length of the NPC and its inclination related to the hard palate as well as the IF diameter were measured for 42 females and 21 males, aged 18 to 67 years old (mean 37.74 years). The shortest canal in this study was 7.20 mm and the longest was 17.40 mm (mean 11.52 mm). The minimum NPC/hard palate inclination was 2.70 degrees and the maximum was 46.20 degrees (mean 17.09 degrees). The smallest IF anteroposterior diameter was 2.5 mm and the largest was 7.30 mm (mean 4.91 mm).
Thirteen canals were hourglass shaped, 23 were cylindrical, 23 were funnel and 4 were spindle.
Statistical analysis was done to determine: (a) if there is a relation between patient’s age and NPC length, inclination related to the hard palate and IF diameter; and (b) if the NPC mean length and inclination and the IF diameter in females are different than the ones in males.
Independent samples T-test and Mann-Whitney U test were conducted to evaluate the differences between genders considering canal’s length and inclination degree and the IF diameter. Spearman correlation analysis was used to assess the correlation between age, NPC length and inclination and the IF diameter.
P < 0.05 was taken to state statistical significance.
The Spearman correlation indicates a weak relationship between the length of the NPC and the IF diameter (r=0.254, P<0.05), as can easily be seen in the scatterplot (Figure 4).
Figure 4.
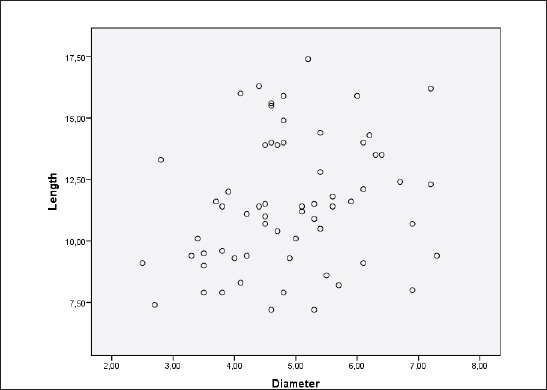
Scatter plot showing a weak relationship between the NPC length and the IF diameter.
No statistically significant relation was found between other variables (P>0.05).
The average length of the NPC for each patient was compared by gender, with the null hypothesis that the mean of the average lengths of the female canals is the same as the mean of the average lengths of the male canals. The average length of the female canals ranged from 7.20 to 16.30 mm, with a mean female length of 10.88 mm and a standard deviation of 2.53 mm. The average length of the male canals ranged from 8.00 to 17.40 mm, with a mean male length of 12.80 mm and a standard deviation of 2.45 mm. A t-test for two sample means was conducted on the length of the female canals compared to the length of the male canals. The p-value for the t-test was 0.006, indicating that the mean lengths of the female canals are significantly shorter than the mean lengths of the male canals when using a significance level of 0.05.
The average length of the NPC for each patient, by gender, is shown in the Boxplot (Figure 5).
Figure 5.
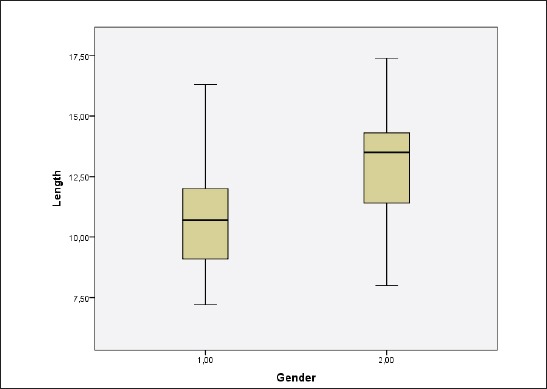
Box plot showing the average length of the NPC for each patient by gender (1,00: Female; 2,00: Male).
The average IF diameter for each patient was compared by gender, with the null hypothesis that the mean of the average of the IF diameter of the female canals is the same as the mean of the average of the male ones. The average IF diameter of the female canals ranged from 2.50 to 7.30 mm, with a mean of 4.74 mm and a standard deviation of 1.18 mm. The average IF diameter of the male canals ranged from 3.70 to 7.20 mm, with a mean of 5.25 mm and a standard deviation of 0.96 mm. A t-test for two sample means was conducted on the IF diameter of the female canals compared to the IF diameter of the male canals. The p-value for the t-test was 0.096, indicating that the mean IF diameters of the female canals is the same as the mean IF diameters of the male canals when using a significance level of 0.05. The average IF diameter of the NPC for each patient, by gender, is shown in the Box plot (Figure 6).
Figure 6.
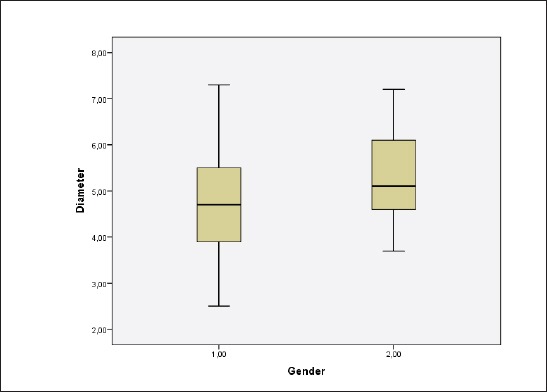
Box plot showing the average IF diameter for each patient by gender. (1,00: Female; 2,00: Male).
The average inclination degree of the NPC related to the hard palate for each patient was compared by gender, with the null hypothesis that the mean of the average inclination of the female canals is the same as the mean of the average inclination of the male canals. The average inclination of the female canals ranged from 5.60 to 46.20 degrees, with a mean female inclination of 16.74 degrees and a standard deviation of 7.77degrees. The average inclination of the male canals ranged from 2.70 to 34.90 degrees, with a mean male inclination of 17.80 degrees and a standard deviation of 8.87 degrees. Mann-Whitney U test for two sample means was conducted on the inclination of the female canals compared to the inclination of the male canals. The p-value for the t-test was 0.699, indicating that the mean inclination of the female canals is the same as the mean inclination of the male canals when using a significance level of 0.05.
The average inclination of the NPC for each patient, by gender, is shown in the Boxplot (Figure 7).
Figure 7.
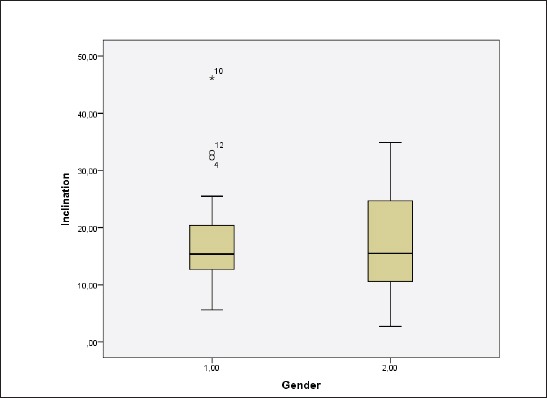
Box plot showing the average inclination of the NPC related to the hard palate for each patient by gender. (1,00: Female; 2,00: Male).
Finally, knowing that the measurement of the inclination of the NPC is the most delicate among the variables of our study, a Mann-Whitney U test for two sample means of canal inclination degree for observer 1 and observer 2 was conducted; no statistically significant difference was found between observers in terms of inclination evaluation (P>0.05).
The average of the two observers for each patient, by inclination degree of NPC, is shown in the Box plot (Figure 8).
Figure 8.
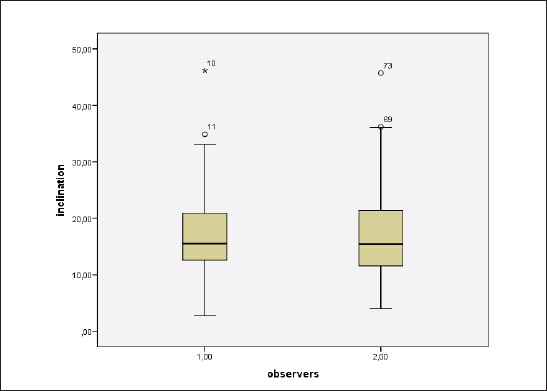
Box plot showing the difference between observers in terms of inclination evaluation. (1,00: First observer; 2,00: Second observer).
For the inter-examiner reliability of inclination degree of NPC, 42.9% of repeated measurement absolute differences were ≤ 1 mm, 82.5% were ≤ 3 mm, and 100% were ≤ 4 mm.
4. DISCUSSION
The nasopalatine canal has been investigated by many researchers in different ways and populations (1-14); some of them on dry skulls (12, 14), the others using the imaging technology, either by two-dimensional (4) or three-dimensional radiography (e.g., CBCT) (1-11, 13, 14).
In the present study, we evaluate the NPC using CBCT technology in a Lebanese population. In our sample, the form of the canal was variable. The cylindrical and funnel-shaped canals were the most detected [23 out of 63 each; (36.50%)] followed by the hourglass-shaped [13 out of 63; (20.63%)] and the spindle-shaped which was the rarest [4 out of 63; (6.34%)]. Our results that are consistent with the ones of Mardinger et al. (2), Tözüm et al. (5), and Liang et al. (6) who found that the NPC cylindrical shape was the most frequent, show a difference with the findings of Mraiwa et al. (4) where the Y-shaped corresponding to the funnel in our study was the most common [22 out of 34; (64.70%)] against the cylindrical [8 out of 34; (23.52%)]. This may be due to ethnicity reason or the limited size of their sample compared to ours.
As for the average length of the NPC, in our study, it was found to be 11.52 mm ranging from 7.20 mm to 17.40 mm; results close to the ones of Thakur et al. (1), Tözüm et al. (5), Fukuda et al. (14) whose mean canal length measurement in a sagittal plane was 10.08 ±2.25mm,10.86 ± 2.67 mm and 11.75 ± 1.70 mm respectively.
On the other hand, higher length canal means were identified by Al-Amery et al. (3) and Kajan et al. (7) and were respectively 16.33 ± 4.43 mm and 12.84 ± 2.88 mm while shorter mean value length (8.1 ± 3.4 mm) was detected by Mraiwa et al. (4).
Interestingly, in our sample, the female canals are significantly shorter than the male ones, a thing which was supported by the findings of Thakur et al. (1), Tözüm et al. (5), and Kajan et al. (7).
However, the study conducted by Al-Amery et al. (3), showed no statistical difference between gender where the mean males NPC length was 17.96 ± 3.96 mm and17.96 ± 4.18 mm for females.
In our study, the IF anteroposterior diameter ranged from 2.5 mm to 7.30 mm with an average of 4.91 mm; this was in agreement with the results of Mraiwa et al. (4) [4.3±0.9 mm (3.3 mm –5.5 mm)] and Salemi et al. (13) [4.74 ± 1.11mm (2.50 mm–8.50 mm)]. For Al-Amery et al. (3) and Kajan et al. (7), the labiopalatal (anteroposterior) diameter of the IF was 2.80 ±0.82 and 3.53 ± 1.1 mm respectively.
Concerning the inclination degree of the NPC in relation with the palatal bone, to the best of our knowledge, the measurement technique we used has not been reported in the literature yet; in our sample, the average finding was 17.09 degrees with a minimum of 2.70 degrees and a maximum of 46.20 degrees.
Finally, in our study, some limiting factors exist such as: (a) the small number of CBCT radiographs assessed making further studies on a larger sample essential to be performed in order to have more precise findings; (b) our group of Lebanese population concerns only the adults making the results not appropriate to younger generations; and (c) in our study, we did not examine the scans of the edentulous patients, something that would be subsequently of interest to be studied.
5. CONCLUSION
Within the limits of this study, we conclude that in Lebanese population, the form of the NPC is variable, predominantly cylindrical or funnel shaped. For the canal length, the inclination related to the hard palate and the IF anteroposterior diameter, no statistical significance between genders was noticed except for the canal height that was found shorter in our female sample.
Footnotes
• Conflict of interest: none declared
REFERENCES
- 1.Thakur AR, Burde K, Guttal K, Naikmasur VG. Anatomy and morphology of the nasopalatine canal using cone-beam computed tomography. Imaging Sci Dent. 2013;43(4):273–81. doi: 10.5624/isd.2013.43.4.273. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mardinger O, Namani-Sadan N, Chaushu G, Schwartz-Arad D. Morphologic changes of the nasopalatine canal related to dental implantation: a radiologic study in different degrees of absorbed maxillae. J Periodontol. 2008;79(9):1659–62. doi: 10.1902/jop.2008.080043. [DOI] [PubMed] [Google Scholar]
- 3.Al-Amery SM, Nambiar P, Jamaludin M, John J, Ngeow WC. Cone beam computed tomography assessment of the maxillary incisive canal and foramen: considerations of anatomical variations when placing immediate implants. PLoS One. 2015;10(2):e0117251. doi: 10.1371/journal.pone.0117251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mraiwa N, Jacobs R, Van Cleynenbreugel J, Sanderink G, Schutyser F, Suetens P, et al. The nasopalatine canal revisited using 2D and 3D CT imaging. Dentomaxillofac Radiol. 2004;33(6):396–402. doi: 10.1259/dmfr/53801969. [DOI] [PubMed] [Google Scholar]
- 5.Tözüm TF, Güncü GN, Yıldırım YD, Yılmaz HG, Galindo-Moreno P, Velasco-Torres M, et al. Evaluation of maxillary incisive canal characteristics related to dental implant treatment with computerized tomography: a clinical multicenter study. J Periodontol. 2012;83(3):337–43. doi: 10.1902/jop.2011.110326. [DOI] [PubMed] [Google Scholar]
- 6.Liang X, Jacobs R, Martens W, Hu Y, Adriaensens P, Quirynen M, et al. Macro- and micro-anatomical, histological and computed tomography scan characterization of the nasopalatine canal. J Clin Periodontol. 2009;36(7):598–603. doi: 10.1111/j.1600-051X.2009.01429.x. [DOI] [PubMed] [Google Scholar]
- 7.Kajan ZD, Kia J, Motevasseli S, Rezaian SR. Evaluation of the nasopalatine canal with cone-beam computed tomography in an Iranian population. Dent Res J. 2015;12:14–9. doi: 10.4103/1735-3327.150289. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Barkin S, Sandor GK, Keller A, Caminiti MF, Clokie C. The nasopalatine canal: an anatomic study and effects on dental implant placement. J Dent Res. 2002;81:437–45. [Google Scholar]
- 9.Bornstein MM, Balsiger R, Sendi P, von Arx T. Morphology of the nasopalatine canal and dental implant surgery: A radiographic analysis of 100 consecutive patients using limited cone-beam computed tomography. Clin Oral Implants Res. 2011;22(3):295–301. doi: 10.1111/j.1600-0501.2010.02010.x. [DOI] [PubMed] [Google Scholar]
- 10.Asaumi R, Kawai T, Sato I, Yoshida S, Yosue T. Three-dimentional observation of the incisive canal and the surrounding bone using cone-beam computed tomography. Oral Radiol. 2010;26:20–8. [Google Scholar]
- 11.Song WC, Jo DI, Lee JY, Kim JN, Hur MS, Hu KS, et al. Microanatomy of the incisive canal using three-dimensional reconstruction of microCT images: an ex vivo study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(4):583–90. doi: 10.1016/j.tripleo.2009.06.036. [DOI] [PubMed] [Google Scholar]
- 12.Jacob S, Zelano B, Gungor A, Abbott D, Naclerio R, McClintock MK. Location and gross morphology of the nasopalatine duct in human adults. Arch Otolaryngol Head Neck Surg. 2000;126(6):741–8. doi: 10.1001/archotol.126.6.741. [DOI] [PubMed] [Google Scholar]
- 13.Salemi F, Moghadam FA, Shakibai Z, Farhadian M. Three-dimensional assessment of the nasopalatine canal and the surrounding bone using cone-beam computed tomography. J Periodontal Implant Dent. 2016;8(1):1–7. [Google Scholar]
- 14.Fukuda M, Matsunaga S, Odaka K, Oomine Y, Kasahara M, Yamamoto M, Abe S. Three-dimensional analysis of incisive canals in human dentulous and edentulous maxillary bones. Int J Implant Dent. 2015;1(1):12. doi: 10.1186/s40729-015-0012-4. [DOI] [PMC free article] [PubMed] [Google Scholar]