

Abstract
Objective:
To assess retinal nerve fiber layer (RNFL) thickness measurements of normal Northern Nigerian adults using optical coherence tomography (OCT).
Subjects and Methods:
The OCT procedure was carried out with the Carl Zeiss Stratus OCT Model 3000 software version 4.0 (Carl Zeiss Meditec AG, Jena, Germany). The fast RNFL scan protocol was used to obtain RNFL thickness measurements. Student's t-test was used to compare mean RNFL thickness values. P ≤ 0.05 was considered as statistically significant. Average RNFL thickness was correlated with age.
Results:
Two hundred and twenty eyes of 110 subjects aged 18–51 years were examined. The average RNFL thickness was 104.17 ± 10.71 μm. The mean values for the RNFL thickness were 129.15 ± 16.87 μm, 135.34 ± 20.40 μm, 85.10 ± 23.60 μm, and 67.19 ± 13.27 μm for the inferior, superior, nasal, and temporal quadrants, respectively. A statistically significant difference was found between males and females for the mean RNFL thickness (t = 3.30, P = 0.001) and for the mean superior and inferior RNFL thickness. There was a statistically significant difference between right and left eyes (t = 3.73, P = 0.001) for the mean RNFL thickness. A negative correlation was found between RNFL thickness and age (r = −0.313, P = 0.002).
Conclusion:
Normal RNFL thickness measurements in healthy Nigerian adults are presented. The RNFL was found to be thicker in females and in right eyes. The values were comparable to those of the Indian population but higher than some Caucasian values.
Keywords: Normal adults, optical coherence tomography, retinal nerve fiber layer thickness, Les adultes normaux, tomographie à cohérence optique, épaisseur de couche de fibres nerveuses rétiniennes
Résumé
Objectif:
Afin d'évaluer les mesures d'épaisseur couche (CFNR) nerveuses rétiniennes fibre des adultes normaux de nigérians du Nord à l'aide de la tomographie par cohérence optique (OCT).
Sujets et Méthodes:
La procédure de OCT a été réalisée avec la version du logiciel Carl Zeiss Stratus OCT modèle 3000 4.0 (Carl Zeiss Meditec AG, Jena, Allemagne). Le protocole de scan rapide CFNR servait à obtenir des mesures d'épaisseur de CFNR. Test t de Student a été utilisé pour comparer les valeurs d'épaisseur CFNR moyennes. P ≤ 0,05 était considérée comme statistiquement significatif. Épaisseur moyenne de CFNR est corrélée avec l'âge.
Résultats:
Deux cent vingt yeux de 110 sujets âgés de 18 à 51 ans ont été examinés. L'épaisseur moyenne de la CFNR est 104.17 ± 10,71 μm. Les valeurs moyennes pour l'épaisseur de la CFNR étaient 129.15 ± 16,87 μm, 135.34 ± 20.40 μm, 85.10 ± 23,60 μm et 67,19 ± 13,27 μm pour les quadrants inférieurs, supérieurs, nasales et temporelles, respectivement. Aucune différence statistiquement significative a été trouvée entre les mâles et les femelles pour l'épaisseur moyenne de la CFNR (t = 3.30, P = 0,001) et pour l'épaisseur moyenne de CFNR supérieur et inférieur. Il y avait un statistiquement différence de significatif entre les yeux droit et gauche (t = 3.73, P = 0,001) pour l'épaisseur moyenne de la CFNR. Une corrélation négative entre l'âge et l'épaisseur de CFNR (r = −0.313, P = 0,002).
Conclusion:
Mesures d'épaisseur normale CFNR adulte en bonne santé nigérian sont présentés. La CFNR s'est avéré pour être plus épais chez les femelles et les yeux droit. Les valeurs étaient comparables à ceux de la population indienne, mais plus élevé que certaines valeurs de la race blanche.
Introduction
Optical coherence tomography (OCT) is a noncontact, noninvasive diagnostic imaging technique which provides in vivo images of retinal nerve fiber layer (RNFL) thickness that are reproducible, quantitative, and objective.[1,2] OCT shows a cross-sectional living histology of the retina.[1] This modern diagnostic imaging technique was introduced in ophthalmology as a means to assess superficial and deep retinal layers including the choriocapillaris. OCT can also be used for cross-sectional imaging and measurements of the optic disc. The OCT is a computer-assisted precision optical instrument that allows analysis of the retinal structure by means of high-resolution tomographic cross-sections of the retina with ≤10 µm axial resolution. It allows visualization of cross-sections of the retina, enabling diagnosis and follow-up in glaucoma and numerous retinal conditions. It works on the principle of low coherence interferometry.[3,4]
OCT imaging is similar to ultrasound but here light is used instead of sound. A near infrared light beam is projected on the retina. The instrument contains an optical interferometer which detects reflection delay and backscattering of light and compares it with a reference reflection from a built-in mirror.[5] The interferometer gives a signal, the strength of which depends upon the optical reflectivity of each retinal structure allowing construction of high-resolution B-scan images. RNFL thickness is measured using algorithms based upon reflectivity changes between adjacent structures.[6]
The aim of the study was to assess RNFL thickness measurements of normal Northern Nigerian adults in Aminu Kano Teaching Hospital (AKTH), Kano, Nigeria using OCT. This is of importance in the diagnosis and monitoring of patients with glaucoma and would serve as a reference data of normal RNFL thickness in our environment. To the best of the authors’ knowledge, no study has been carried out in Nigeria to determine normal RNFL thickness measurements using OCT.
Subjects and Methods
The study adhered to the Tenets of the Helsinki Declaration. Ethical approval was obtained from the Ethics Review Board of AKTH. This descriptive cross-sectional study was carried out from April 2010 to January 2011. The minimum sample size calculated for the study was 100 using Fisher's formula. Consecutive subjects that consented and had normal findings on basic eye examination were recruited into the study. One hundred and ten subjects took part in the study. These were randomly selected and comprised of staff of the hospital, medical students of Bayero University Kano, students from the School of Information Management AKTH and outpatients that presented to the eye clinic of AKTH who met the inclusion criteria. Criteria for the inclusion were age 18 years and above, consent to be part of the study, unaided visual acuity of 6/6 or better, normal intraocular pressure (10–21 mmHg),[7,8,9] a clinically normal optic disc (pink, well defined margins, normal vasculature in the absence of other pathologies). Subjects with a history of glaucoma, intraocular surgery, a laser procedure, ocular trauma, and a history of systemic diseases such as diabetes mellitus, hypertension, and sickle cell disease were excluded from the study. Visual acuity was tested using an illuminated Snellen's chart; anterior segment examination was done using a slit lamp bio microscope while fundus examination was done using a Keeler professional Direct Ophthalmoscope. The intraocular pressure was measured by applanation tonometry. The OCT procedure was carried out with the Carl Zeiss Stratus OCT Model 3000 software version 4.0 (Carl Zeiss Meditec AG, Jena, Germany). The fast RNFL scan protocol was used to obtain RNFL thickness measurements from both eyes of the subjects. The computer gave an analysis of the average RNFL thickness, the thickness of the superior, inferior, nasal and temporal quadrants, and thickness of clock hours. Scans with signal strengths of 6 or more out of a maximum of 10 were included in the study and those with <6 were canceled. In addition, scans that showed “scan too high,” “scan too low,” or “missing data” were repeated.
Data analysis was done using the statistical software Statistical Package for the Social Sciences version 16.0, International Business Machines Corporation, Armonk, New York, United States of America. Student's t-test was used to compare the mean RNFL thickness values between males and females and between right and left eyes. A P ≤ 0.05 was considered as statistically significant. Average RNFL thickness was correlated with age, and the correlation coefficient was estimated.
Results
One hundred and ten subjects took part in the study. There were 77 males and 33 females (male:female = 7:3). Their ages ranged from 18 to 51 years and the mean age was 30.47 ± 7.80 years. Table 1 shows a summary of the age and sex distribution of the subjects.
Table 1.
Age and sex distribution of subjects
| Age (years) | Male (%) | Female (%) | Total (%) |
|---|---|---|---|
| 18-27 | 27 (58.7) | 19 (41.3) | 46 (100) |
| 28-37 | 27 (71.1) | 11 (28.9) | 38 (100) |
| 38-47 | 21 (87.5) | 3 (12.5) | 24 (100) |
| 48-57 | 2 (100) | 0 (0) | 2 (100) |
| Total | 77 (70) | 33 (30) | 110 (100) |
Two hundred and twenty eyes of 110 subjects were tested in the study. The overall average RNFL thickness was 104.17 ± 10.71 µm. The mean values of the RFNL thickness in the inferior, superior, nasal and temporal quadrants, and are summarized in Table 2. The mean RNFL thickness for the male and female subjects was 102.64 ± 10.22 µm and 107.73 ± 11.08 µm, respectively. There was a statistically significant difference (t = 3.30, P = 0.001) with the RNFL being thicker in females. The mean RNFL thickness by quadrants for the male and female subjects is summarized in Table 3. The gender difference between the mean measurements for the inferior and superior quadrants was statistically significant.
Table 2.
Mean RNFL thickness by quadrant (n=220)
| Quadrant | Mean±SD (µm) |
|---|---|
| Inferior | 129.15±16.87 |
| Superior | 135.34±20.40 |
| Nasal | 85.10±23.60 |
| Temporal | 67.19±13.27 |
n=Number of eyes, SD=Standard deviation, RNFL=Retinal nerve fiber layer
Table 3.
Mean male and female RNFL thickness by quadrant
| Quadrant | RNFL thickness±SD (µm) | Student's t-test | P | Significance | |
|---|---|---|---|---|---|
| Male (n=154) | Female (n=66) | ||||
| Inferior | 126.48±15.85 | 135.36±17.63 | 3.68 | 0.001 | Significant |
| Superior | 133.36±19.45 | 139.95±21.94 | 2.21 | 0.028 | Significant |
| Nasal | 84.32±22.67 | 86.91±25.74 | 0.75 | 0.457 | Not significant |
| Temporal | 66.60±13.96 | 68.55±11.48 | 1.00 | 0.319 | Not significant |
RNFL=Retinal nerve fiber layer, SD=Standard deviation
The mean RNFL thickness of the right and left eyes was 106.78 ± 10.26 µm and 101.55 ± 10.56 µm, respectively. This difference was statistically significant (t = 3.73, P = 0.001). In all quadrants, RNFL was thicker in right eyes with a statistically significant difference in the mean values between the right and left eyes in the superior, nasal, and temporal quadrants.
A negative correlation was found between mean RNFL thickness and age as shown in Figure 1. RNFL thickness decreased with increasing age (Pearson's correlation coefficient r = −0.313, P = 0.002). Figure 2 shows the RNFL OCT print out of a normal male subject.
Figure 1.
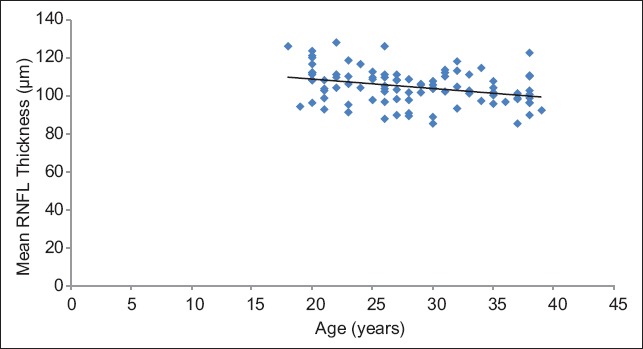
Correlation between mean retinal nerve fiber layer thickness and age
Figure 2.
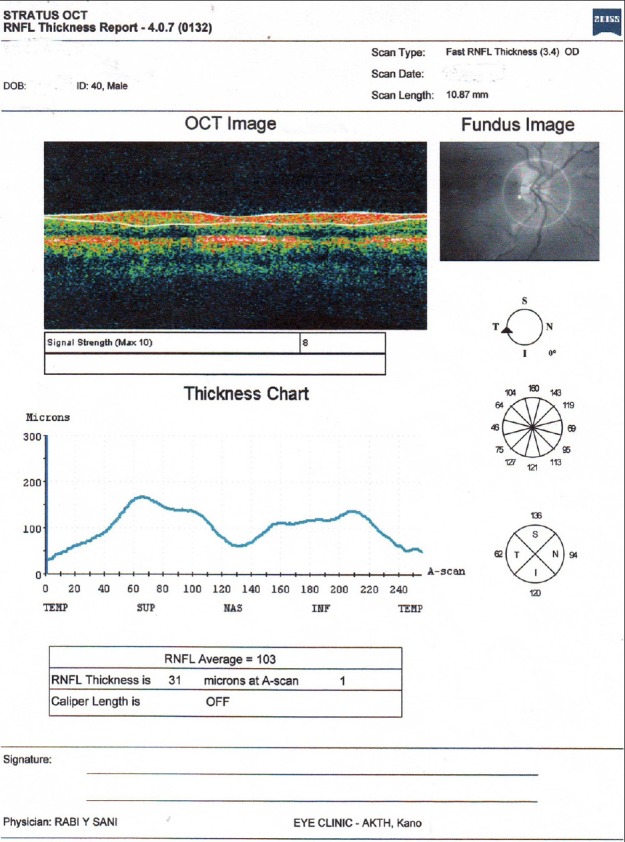
Retinal nerve fiber layer thickness optical coherence tomography print out of the right eye of a normal male subject
Discussion
There appears to be paucity of studies giving normal data values for peripapillary RNFL thickness in adults using OCT in our setting. To the best of the authors’ knowledge, no study has been done in Africa to generate the normative database for RNFL thickness in adults using OCT. Normal data for RNFL thickness enables distinguishing normal from disease conditions. The OCT technology measures RNFL thickness objectively and detects thinning of this layer, which can occur in conditions like glaucoma.[10]
In this study, the subjects were mainly in the young and middle-age group. There were also more males than females. This is in line with the pattern of the hospital attendance.
Average RNFL thickness of subjects in this study was found to be similar to that of Indians[1,2,11,12] and Japanese.[13] Lower mean RNFL thickness values were obtained in similar studies carried out in California,[14] New England,[15] and Italy.[16] Racial differences could be the possible explanation for this. All these studies were carried out using the Stratus OCT. Studies have shown that RNFL thickness values differ between different OCT types and these should not be used interchangeably.[17,18]
The mean RNFL thickness in this study was most in the superior quadrant, followed by the inferior quadrant, then the nasal, and finally, the temporal quadrant. This finding is contrary to the ISNT rule and a significant difference. Similar findings were seen in some Indian studies.[1,2,11]
The thickness of the RNFL was found to be more in females in this study. A Latin American study showed the inferior RNFL to be thicker in Latino women than in Latino men. This could be due to racial or ethnic differences.[19]
Findings from this study showed the RNFL to be thicker in right eyes. To the best of the authors’ knowledge, there is no study with a similar finding. The possible reason for this finding is difficult to explain. More studies are needed to give more evidence of this finding.
There was a decrease in RNFL thickness with increasing age of the subjects studied. Increasing age is associated with a decline in RNFL thickness. This is in keeping with findings of other studies in North America,[6,20] Latin America,[19] Germany,[21,22] India,[1,2,12,23] Iran,[24] and Japan.[13,25,26,27] Lower RNFL values in older patients may not be due to a pathological cause.
A limitation of this study is that it was carried out in North-Western Nigeria, the population of which comprises mostly the Hausa-Fulani ethnic group. This makes up one-third of the major ethnic groups in the country therefore, not giving a full picture of what could be obtained in other parts of the country. Second, the study population consisted mostly of young and middle-aged individuals. Values obtained therefore, may not be generalizable. Visual field testing was not done on the subjects. However, those with characteristic optic disc changes suggestive of glaucoma were excluded. In the future, similar studies should be carried out in other geopolitical zones of Nigeria so that RNFL thickness values obtained could be compared to know if the findings from this study are peculiar to the Northern part of Nigeria or if the same findings are obtained in all parts of Nigeria. In addition, older subjects should be included in future studies to give evidence of stronger negative correlations between RNFL thickness and age. Importantly, the OCT technology should be made more available in training centers in Nigeria and other parts of Africa to generate normal data of RNFL thickness measurements. OCT is essential in the management of diseases of the retina and optic nerve.
Conclusion
Normal RNFL thickness measurements of healthy Northern Nigerian adults are presented. RNFL was found to be thicker in females and in right eyes. In view of this, females with apparently normal RNFL thickness may have glaucomatous damage. The values were comparable to those of the Indian population but higher than some Caucasian values.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Sony P, Sihota R, Tewari HK, Venkatesh P, Singh R. Quantification of the retinal nerve fibre layer thickness in normal Indian eyes with optical coherence tomography. Indian J Ophthalmol. 2004;52:303–9. [PubMed] [Google Scholar]
- 2.Ramakrishnan R, Mittal S, Ambatkar S, Kader MA. Retinal nerve fibre layer thickness measurements in normal Indian population by optical coherence tomography. Indian J Ophthalmol. 2006;54:11–5. doi: 10.4103/0301-4738.21608. [DOI] [PubMed] [Google Scholar]
- 3.Ramakrishnan R, Kader MA, Budde WM. Optic disc morphometry with optical coherence tomography: Comparison with planimetry of fundus photographs and influence of parapapillary atrophy and pigmentary conus. Indian J Ophthalmol. 2005;53:187–91. doi: 10.4103/0301-4738.16678. [DOI] [PubMed] [Google Scholar]
- 4.Brancato R, Lumbroso B. Guide to Optical Coherence Tomography Interpretation. Italy: I.N.C Innovation-News-Communication; 2005-2006. pp. 1–11. [Google Scholar]
- 5.Bressler NM, Ahmed IK, Nguyen QD, Shah M, Do DV, Hwang T. The Stratus OCT Primer Essential OCT. 1st ed. California: Carl Zeiss Meditec; 2006. About OCT; pp. 1–2. [Google Scholar]
- 6.Budenz DL, Anderson DR, Varma R, Schuman J, Cantor L, Savell J, et al. Determinants of normal retinal nerve fiber layer thickness measured by Stratus OCT. Ophthalmology. 2007;114:1046–52. doi: 10.1016/j.ophtha.2006.08.046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Kwon YH, Fingert JH, Greenlee EC. Section 6-B: Intraocular Pressure and Corneal Pachymetry. A Patient's Guide to Glaucoma. [Last accessed on 2011 Jun 11]. Available from: www.medrounds.org/…/section-6-b-intraocular-pressure-and.html .
- 8.Noecker RJ. Glaucoma Overview. [Last accessed on 2015 Aug 07]. Available from: www.emedicinehealth.com/glaucoma_overview/article_em.htm .
- 9.American Academy of Ophthalmology. Introduction to glaucoma: Terminology, epidemiology and heredity. Glaucoma 2007-2008. Basic and Clinical Science Course Section 10. San Francisco: The Eye MD Association; 2007. [Google Scholar]
- 10.Ip M, Liao OC, Duker JS. Foundation. Ch. 107. Vol. 2. New York: Lippincott Williams and Wilkins; 2003. Optical coherence tomography. Duane's Clinical Ophthalmology on CD-ROM 2004 ed. [Google Scholar]
- 11.Sihota R, Sony P, Gupta V, Dada T, Singh R. Diagnostic capability of optical coherence tomography in evaluating the degree of glaucomatous retinal nerve fiber damage. Invest Ophthalmol Vis Sci. 2006;47:2006–10. doi: 10.1167/iovs.05-1102. [DOI] [PubMed] [Google Scholar]
- 12.Malik A, Singh M, Arya SK, Sood S, Ichhpujani P. Retinal nerve fiber layer thickness in Indian eyes with optical coherence tomography. Nepal J Ophthalmol. 2012;4:59–63. doi: 10.3126/nepjoph.v4i1.5852. [DOI] [PubMed] [Google Scholar]
- 13.Oshitari T, Hanawa K, Adachi-Usami E. Macular and retinal nerve fiber layer thickness in Japanese measured by Stratus optical coherence tomography. Clin Ophthalmol. 2007;1:133–40. [PMC free article] [PubMed] [Google Scholar]
- 14.Nouri-Mahdavi K, Hoffman D, Tannenbaum DP, Law SK, Caprioli J. Identifying early glaucoma with optical coherence tomography. Am J Ophthalmol. 2004;137:228–35. doi: 10.1016/j.ajo.2003.09.004. [DOI] [PubMed] [Google Scholar]
- 15.Paunescu LA, Schuman JS, Price LL, Stark PC, Beaton S, Ishikawa H, et al. Reproducibility of nerve fiber thickness, macular thickness, and optic nerve head measurements using Stratus OCT. Invest Ophthalmol Vis Sci. 2004;45:1716–24. doi: 10.1167/iovs.03-0514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Carpineto P, Ciancaglini M, Aharrh-Gnama A, Cirone D, Mastropasqua L. Custom measurement of retinal nerve fiber layer thickness using STRATUS OCT in normal eyes. Eur J Ophthalmol. 2005;15:360–6. doi: 10.1177/112067210501500308. [DOI] [PubMed] [Google Scholar]
- 17.Seibold LK, Mandava N, Kahook MY. Comparison of retinal nerve fiber layer thickness in normal eyes using time-domain and spectral-domain optical coherence tomography. Am J Ophthalmol. 2010;150:807–14. doi: 10.1016/j.ajo.2010.06.024. [DOI] [PubMed] [Google Scholar]
- 18.Huang J, Liu X, Wu Z, Guo X, Xu H, Dustin L, et al. Macular and retinal nerve fiber layer thickness measurements in normal eyes with the Stratus OCT, the Cirrus HD-OCT, and the Topcon 3D OCT-1000. J Glaucoma. 2011;20:118–25. doi: 10.1097/IJG.0b013e3181d786f8. [DOI] [PubMed] [Google Scholar]
- 19.Varma R, Bazzaz S, Lai M. Optical tomography-measured retinal nerve fiber layer thickness in normal latinos. Invest Ophthalmol Vis Sci. 2003;44:3369–73. doi: 10.1167/iovs.02-0975. [DOI] [PubMed] [Google Scholar]
- 20.Bowd C, Weinreb RN, Williams JM, Zangwill LM. The retinal nerve fiber layer thickness in ocular hypertensive, normal, and glaucomatous eyes with optical coherence tomography. Arch Ophthalmol. 2000;118:22–6. doi: 10.1001/archopht.118.1.22. [DOI] [PubMed] [Google Scholar]
- 21.Bendschneider D, Tornow RP, Horn FK, Laemmer R, Roessler CW, Juenemann AG, et al. Retinal nerve fiber layer thickness in normals measured by spectral domain OCT. J Glaucoma. 2010;19:475–82. doi: 10.1097/IJG.0b013e3181c4b0c7. [DOI] [PubMed] [Google Scholar]
- 22.Alamouti B, Funk J. Retinal thickness decreases with age: An OCT study. Br J Ophthalmol. 2003;87:899–901. doi: 10.1136/bjo.87.7.899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Mansoori T, Viswanath K, Balakrishna N. Retinal Nerve Fiber Layer Thickness in Normal Population Using Spectral Domain Optical Domain Tomography. [Last accessed on 2011 Apr 22]. Available from: http://www.aios.org/proceed10/GLU-11/Glu-114.pdf .
- 24.Pakravan M, Aramesh S, Yazdani S, Yaseri M, Sedigh-Rahimabadi M. Peripapillary retinal nerve fiber layer thickness measurement by three-dimensional optical coherence tomography in a normal population. J Ophthalmic Vis Res. 2009;4:220–7. [PMC free article] [PubMed] [Google Scholar]
- 25.Hirasawa H, Tomidokoro A, Araie M, Konno S, Saito H, Iwase A, et al. Peripapillary retinal nerve fiber layer thickness determined by spectral-domain optical coherence tomography in ophthalmologically normal eyes. Arch Ophthalmol. 2010;128:1420–6. doi: 10.1001/archophthalmol.2010.244. [DOI] [PubMed] [Google Scholar]
- 26.Kanno M, Nagasawa M, Suzuki M, Yamashita H. Peripapillary retinal nerve fiber layer thickness in normal Japanese eyes measured with optical coherence tomography. Jpn J Ophthalmol. 2010;54:36–42. doi: 10.1007/s10384-009-0753-9. [DOI] [PubMed] [Google Scholar]
- 27.Nagai-Kusuhara A, Nakamura M, Fujioka M, Tatsumi Y, Negi A. Association of retinal nerve fibre layer thickness measured by confocal scanning laser ophthalmoscopy and optical coherence tomography with disc size and axial length. Br J Ophthalmol. 2008;92:186–90. doi: 10.1136/bjo.2007.127480. [DOI] [PubMed] [Google Scholar]