

Abstract
Background
The aim of this study was to investigate the effects of sleep duration and bedtime on sperm health, and the possible mechanism involved.
Material/Methods
We randomly divided 981 healthy Chinese men into groups according to research-set bedtimes (A=8–10 PM, B=after 10 PM, and C=after midnight) and sleep durations: group 1=<6.0 h (short), group 2=7.0–8.0 h (average), and group 3=>9.0 h (long). Sperm morphology, count, survival, and motility were examined according to sleep patterns. Antisperm antibody (ASA) production in semen was determined.
Results
Sperm counts and their survival rates were lower in the short sleepers as compared to others within each group (all P<0.01). The lower counts and survival rates were observed in different bedtimes, with significant differences found between measurements of C1 vs. A1 and C2 vs. A2 or B2 (all P<0.05 or 0.01). Semen motility was lower in the short sleepers as compared to the average and long sleepers (all P<0.01). There were differences in the bedtime-related results between measurements of C1 vs. A1 or B1 (P<0.05 or 0.01). Additionally, the population proportion for the ASA-positive participates and incidence of the ASA-expressed population obviously increased in the short sleepers as compared to others within each group (all P<0.05).
Conclusions
Short and long sleep durations and late bedtime were associated with impaired sperm health in the study cohort, partly through increasing ASA production in the semen.
MeSH Keywords: Semen Analysis, Sperm Count, Survival Rate
Background
Sleep is a natural and periodic state of rest for the mind and body, occurring at regular intervals. Proper sleep is a fundamental component of a healthy lifestyle. The amount of sleep each person needs depends on many factors, including age. For most adults, 7 to 8 h per night appears to be the best amount of sleep [1–3]. Sleep deprivation is now being recognized as an increasingly common condition inherent to modern society [4], so sleep loss not only is a social issue but also leads to a large number of human disorders, including male reproductive impairment [5]. It has been found that the frequency of sleep disturbances has increased in the industrialized world during the past few decades, and inadequate sleep can decrease semen quality [6,7].
Some studies have shown that sleep deprivation may impair immune function; the levels of IgG, IgA, and IgM were enhanced in the sleep-deprived cohort, suggesting that insufficient sleep may induce changes in the parameters of serum humoral immunity [8,9]. Despite the growing literature on the relationship between sleep loss and reduced sperm quality [5,7], the effects of sleep duration and bedtime on ASA production have been studied less extensively.
The purpose of this study was to investigate effects of sleep duration and the research-set bedtimes on affecting sperm quality and the ASA production in 981 healthy Chinese men living in the northeast region of China. Our results not only indicated the effects of inappropriate sleep experiences on influencing sperm health, but also revealed an important molecular mechanism involved.
Material and Methods
Study population and inclusion criteria
In this prospective study, 981 healthy male adults voluntarily participated in an investigation on the effects of sleep duration and bedtime on i sperm quality during the period from September 2013 to April 2014. The volunteers, ages 18–50 years (mean 29.56+5.38 years), were selected for this study according to the following criteria: 1) a good and regular sleep duration and ideal bedtime established over the last 6 months prior to starting the study; 2) no clinical manifestations of neurological or psychiatric disorders, and no history of trauma or surgical treatments; 3) no medical conditions in which a man does not have any measurable level of sperm in his semen or there is no sperm in the ejaculate; 4) no medical problems such as chronic systemic disease, endocrine disease, urinary tract infections, or varicocele; 5) no prescribed drugs taken within 1 month prior to the study; and 6) written informed consent for using the sperm. This study was approved by the Ethics Committee of the Second Affiliated Hospital of Harbin Medical University.
Design of experiments
In this prospective study, we randomly divided 981 healthy male adults into groups according the research-set bedtimes and the length of sleeping time (in hours). All participants had been in consistent sleep patterns for 3 consecutive months. The volunteers in groups A, B, and C started to sleep at bedtimes of 8–10 PM, 10 PM–midnight, and after midnight, respectively. The participants in each group were subdivided into 3 subgroups based on duration of sleep (in hours): <6.0 h (short sleepers), 7.0–8.0 h (average sleepers), and >9.0 h (long sleepers). The numbers of participants in each group were 110, 105, and 113 in A1–3; 106, 111 and 114 in B1–3; and 111, 104, and 107 in C1–3.
Preparation of semen samples
Semen collection refers to the process of obtaining semen from male humans via masturbation, which is the most common way to collect a semen sample [10]. All donors were required to refrain from any sexual activity for 3–7 days before collecting semen at our Hospital Reproduction Health Center, since longer or shorter periods of abstinence may result in a lower sperm count or decreased sperm motility. After washing hands with soap and water, all donors collected a semen specimen by masturbation into a wide-mouth sterile sample cup in a room close to the semen laboratory. The donors were instructed to capture the first part of the ejaculate in the process of collecting a semen sample and to not attempt to collect any spilled semen. They were told to cap the container as soon as a sample collection has been finished. The sample cups were rapidly placed in a water tank at 37°C. Semen tests were not carried out until samples fully turned to liquid.
Semen analyses
A semen analysis typically measures the number of sperm per milliliter of ejaculate, and analyzes sperm morphology and motility. In order to achieve the most accurate results, the semen specimens obtained by masturbation were delivered to the lab for semen analysis within 30 min of the specimen collection time. The semen analysis was performed by use of a computer image analyzer system (Cellsoft; Cryo Resources Co., NY). The outcomes of analysis mainly included: 1) Sperm morphology, which was viewed under a microscope (Olympus, Japan) at a magnification of 400 and was expressed as a percentage of normal sperm having an oval head with a long tail; 2) Sperm count, expressed as the number of sperm per milliliter (mL) of semen in 1 ejaculation; 3) Survival rate, calculated as a percentage of the sperm with movement characteristics in total sperm counts in the semen; and 4) Sperm motility, which is sperm swimming forward progressively, expressed as a percentage of motile sperm according to WHO criteria [11]. More specified measures were defined by motility grades of A (progressive motility) and B (non-progressive motility).
Assay of antisperm antibody
The ASA test was used to identify a special protein (antibody) that attacks sperm. The kit for ASA detection was purchased from Yilikang Biochemistry Technology Co., LTD (ZheJiang, China). Content of the ASA production in the semen was measured by enzyme-linked immunosorbent assay (ELISA) according to the manufacturer’s instructions. Briefly, 100 ml of semen sample was added into the ELISA plate coated with a primary antibody (1: 100) for human spermatozoa protein and then incubated for 30 min at 37°C. After washing, horseradish peroxidase-conjugated secondary antibody (1: 200) was added into each well of the plate and incubated for 30 min. After washing, 50 ml of a substrate TMB (3,3′,5,5′-tetramethylbenzidine) was added to yield a color reaction. Absorbance values were determined at a wavelength of 450 nm using a microplate reader. The experimental operation and analysis of results were implemented strictly in accordance with the kit instructions.
Statistical analyses
Values are expressed as Mean ± Standard Deviation (SD). Results were calculated as absolute numbers and a percentage of sperm counts in semen samples harvested from the grouped participants. Statistical analysis was performed using the SAS 9.1 software package. Comparisons from groups with individual measurements were performed by Fisher’s least significant difference (LSD) or Dunnett’s test. The chi-square test (χ2) was conducted to analyze the significance of parameters within groups. A P value of <0.05 was considered significant.
Results
Age distribution and sperm morphology
In this prospective study, 981 healthy male adults were selected for assessing the effects of sleep conditions on sperm production. Age distribution (in years) was first examined in the grouped participants and the results are shown in Figure 1A. In contrast, a similar distribution model for the average age may clearly be observed at the ranges of 28.93–30.16 years in the investigated participants. There were no statistically significant differences found in the values of average ages between any 2 groups.
Figure 1.

Age distribution and sperm morphology. Age distribution for the grouped participants was examined in sleep conditions with an average age (A) presented for the study cohort. Changes in sperm morphology were calculated as a percentage (B) of normally shaped sperm cells in the total sperm counts. Data are expressed as Mean ±SD. A, B, and C were the research-set bedtimes. Sleep duration is grouped as 1, 2, and 3.
Sperm morphology in sleep conditions was examined under a microscope. The numbers of normally shaped sperm in semen samples from the grouped participants was calculated as a percentage (%) in a total sperm count and the results are shown in Figure 1B. An average value (%) for the normal sperm was displayed at the ranges of 68.27–70.71 years in all groups. In further observation, the sperm cells in the semen were abundant in reaching over 68% of the total sperm count in the study cohort. In contrast, there were no significant differences in sperm morphology between any 2 groups.
Sperm count and survival rate
Sperm counts in the semen obtained from the grouped participants were examined according to sleep patterns. Sperm cells (million/ml) in the semen are expressed as an absolute count in the semen volume and the results are shown in Figure 2A. In data analysis, there were significant decreases in the values of A1, A3, B1, B3, and C1 as compared to A2, B2, and C2 within each group (all P<0.01). Furthermore, the sperm counts in groups C1 and C2 significantly decreased with between C1 vs. A1 and C2 vs. A2 or B2 (all P<0.01).
Figure 2.

Sperm count and survival rate. Sperm counts (A) in semen samples and their survival rates (B) were examined in sleep patterns in the grouped participants. Sperm counts (million/ml) and survival rates (%) are shown as an absolute number of sperm cells in the semen volume. The results are expressed as Mean ±SD. A, B, and C were the research-set bedtimes. Sleep duration is grouped as 1, 2, and 3. ** P<0.01 vs. A1, A3, B1, B3, and C1. #, ## P<0.05 vs. A2 and B2 in survival rate or <0.01 vs. A2 and B2 in sperm counts. $$ P<0.01 vs. A1.
Survival rates for sperm cells in the semen were examined with sleep experiences in the grouped participants and the results are shown in Figure 2B. In statistical analysis of the survival rate, there were obvious decreases in the values from the A1-, A3-, B1-, B3- and C1-grouped cohorts as compared to others within each group (all P<0.01). Moreover, a significant decrease in the survival rate was also observed in the C2-grouped participants with a difference between C2 vs. A2 or B2 (both P<0.05).
Observation on sperm motility
Sperm motility at levels A and B was analyzed according sleep conditions. Data regarding the motility were calculated as a percentage in the total sperm cells in each group and the results are shown in Figure 3A and 3B. In analysis of the A level, there were significant lower values of A1, A3, B1, B3, and C1 as compared to others within each group (all P<0.01). Additionally, there were significantly lower sperm counts in the C1-grouped participants, with significant differences between C1 vs. A1 or B1 (both P<0.05). In terms of the B level, there were significantly lower values of A1 and C1 as compared to others within each group (all P<0.01). In further analysis, obviously lower levels were observed in the C1- and C2-grouped cohorts, with significant differences between C1 vs. B1 and C2 vs. A2 (P<0.05 or 0.01).
Figure 3.

Sperm motility. Sperm motility at the levels of A and B was tested in sleep conditions. Data were calculated as a percentage in the total sperm cells in each group of participants. The results are expressed as Mean ±SD. A, B, and C were the research-set bedtimes. Sleep duration is grouped as 1, 2, and 3. ** P<0.01 vs. A1, A3, B1, B3, and C1 in the A level and vs. A1 and C1 in the B level. ## P<0.01 vs. A2. $, $$ P<0.05 or 0.01 vs. A1 and B1 in the A level and vs. B1 in the B level.
Demographic distribution and incidence of ASA-positive participants
Demographic data from the grouped volunteers were collected from groups with different sleep conditions. The numbers of the grouped participants were shown at the ranges of 104–114 (Figure 4). Population proportions of ASA-positive participants were significantly higher in the A1-, B1-, and C1-grouped cohorts as compared to others within each group (all P<0.05). In comparison of the proportions from groups A1, B1, and C1, there were no significant differences in the proportional distributions of ASA-positive individuals between any 2 groups.
Figure 4.
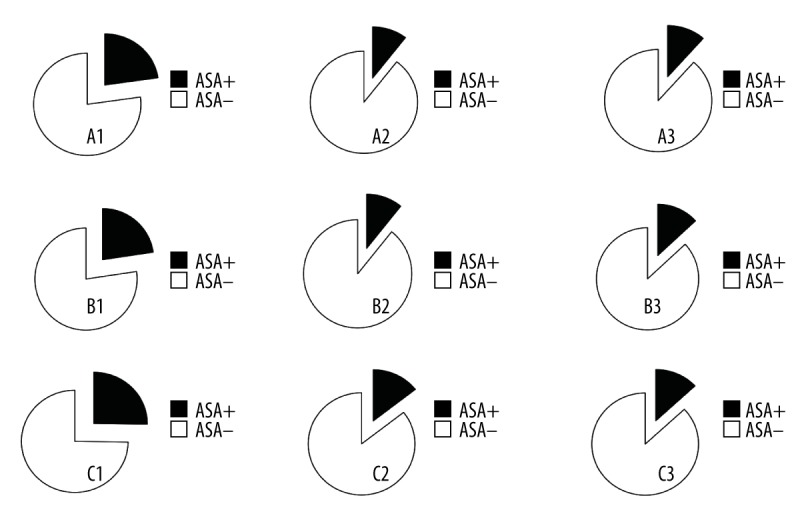
Distribution for ASA-positive population. Demographic data from the grouped participants was analyzed in sleep conditions in presence (black) and absence (white) of ASA production. A population proportion for the ASA-positive participants presented as individual numbers in each group. A, B, and C indicate the research-set bedtimes. Sleep duration is grouped as 1, 2, and 3. A χ2 test showed a p value of <0.05 vs. others within each group, respectively. * P<0.05 vs. other incidences within each group.
The proportion of ASA-expressing participants was calculated as a percentage in the total population in each group (Figure 5). In contrast, the numbers of ASA-positive individuals in groups A1, B1, and C1 were significantly higher (2-fold) within each group (all P<0.05). In further analysis of A1, B1, and C1, there were no significant differences in the incidence between any 2 groups.
Figure 5.
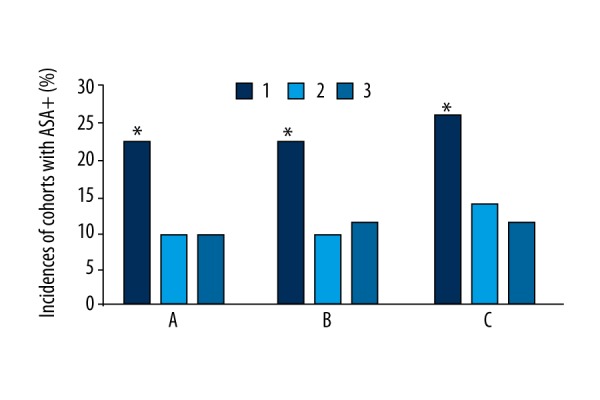
Incidence of ASA-positive individuals. Proportion of ASA-positive individuals was examined according to sleep conditions in the grouped participants, expressed as a percentage of the total participants in each group. The results are shown as Mean ±SD. A, B, and C indicate the research-set bedtimes. Sleep duration is grouped as 1, 2, and 3. * P<0.05 vs. other incidences within each group.
Discussion
Sleep is essential for mental and physical health. Human sleep needs vary by age and among individuals; therefore, the effect of age must be accounted for in research on the effect of length of sleep on male fertility [12,13]. Demographic data obtained from these healthy male adults manifested a similar distribution pattern of the average age with a slight change of about 2 years among the grouped participants. In contrast, there was no significant difference seen between any 2 groups, indicating that the age factor did not need to be considered in further measures and statistical analysis regarding these effects of sleep experiences on sperm health in the investigated cohort.
Sperm morphology is used to observe the size and shape of sperm cells [14], which is one of the semen examinations in evaluating the effects of sleep on sperm production. Our results showed that the percentages of normally shaped sperm in the total sperm count reached 68.27–70.37%. Furthermore, there was no significant difference observed between any 2 groups, indicating that differences in sperm morphology are not a sensitive parameter for assessing the effects of sleep conditions on sperm quality.
Sperm count and survival rates were analyzed according to sleep patterns. Our data revealed that the numbers of sperm cells in the semen and their survival rates were significantly lower in all of the short sleepers and the most of the long sleepers, suggesting that reduction in the sperm cells depended on the length of sleep time. It has been reported that short and long sleep were associated with a higher prevalence of coronary heart disease, stroke, and diabetes, in addition to obesity and frequent mental distress, compared with optimal sleepers [15,16]. Lack of sleeping time may reduce sperm quality [7]. However, an extra hour of sleep in this study also showed lower sperm count and survival rate, suggesting the negative effect of sleeping too little or too much. Furthermore, sleeping longer does not necessarily produce higher-quality sleep. For most adults, the optimal length of sleeping time is about 7–8 h a night [1–3]. Long sleeping commonly is >9.0 h of sleep each night for adults [17], which may disrupt circadian rhythms, affecting the depth and length of sleep on subsequent nights, thereby impairing sperm health.
In contrast to the individuals who went to bed at 10 PM-midnight, our data clearly show that late bedtime is associated with lower sperm counts and survival in all of the short sleepers and some of the average sleepers, suggesting that late bedtime is an important factor. Frequent shifts in sleep timing were associated with metabolic problems and increased prevalence of depressive symptoms [18,19]. However, the literature on effects of bedtime on sperm health is scant. Based on the effect of late bedtime on reduction of sperm production, it is likely that a later bedtime could reduce the depth of sleep, which in turn can lead to poor sleep quality on subsequent nights due to feeling sleepy the next day.
In support of the above findings, sperm motility at the A and B levels were examined in sleep conditions. The data from the A level showed that the proportion of progressively motile sperm was significantly lower in all of the short sleepers and most of the long sleepers, which was identical to the results on the sperm count and survival. In the B level, our results show that the numbers of non-progressively motile sperm were lower only in most of the short sleepers, suggesting that impairment of sleep had less effect on sperm motility at the B level than on the A level. In association with these findings, our results also revealed that a late bedtime decreased the numbers of motile sperm at both levels, suggesting that later bedtime reduced sperm movement. Numerous studies have shown that sperm motility can be affected by unhealthy lifestyle [20,21]. Moreover, a poor sleep schedule can make affect the quantity and quality of sleep [22,23]. The lower sperm motility is probably due to a ripple effect of the bedtime-induced poor sleep quality.
A possible mechanism by which sleep experiences influenced sperm quality was investigated in the grouped participants. Our results showed a similar distribution pattern of population proportions for the average and long sleepers who were ASA-positive. There was a significantly higher proportion of ASA-positive individuals among short sleepers, with no differences in bedtimes between the grouped cohorts, suggesting that the increased ASA production was associated with shorter duration of sleep but not bedtimes. In association with this finding, the proportion of individuals who were ASA-positive was obviously higher in the short sleepers as compared to others within each group, strongly supporting that deficient sleep was a major contributor to presence of ASA in the semen. Antisperm antibodies are immune-reactive particles produced by the body as a response against the proteins contained in sperm [24]. The antibodies target sperm in the body and destroy healthy sperm [25]. The male may produce antibodies to his own sperm as a result of contact between blood cells and sperm, as through testis inflammation, varicocele, intercourse, or sometimes for unknown reasons [26–28]. Our study revealed a relationship between insufficient sleep duration and increased ASA content, and it would be useful to know how sleep deprivation affects sperm health. Since the lower ASA level in the short sleepers was not associated with changes in the research-set bedtimes, it is likely that the effect of bedtime in impairing sperm health was a separate factor, with a potential effect on production of sperm cells. Further research is needed to determine the exact mechanism involved.
Conclusions
Our study results show that short and long sleep durations and later bedtime can reduce sperm count, survival, and motility, partly through increasing ASA production.
Acknowledgments
We would like to thank Dr. Zhuofu Liu for help with statistical analysis.
Footnotes
Conflict of interest disclosures
None.
Source of support: This study was supported by the Harbin Scientific Innovation Project for Elite Young Researchers (Grant No. 2013RFQXJ096)
References
- 1.Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Sleep duration and all-cause mortality: A systematic review and meta-analysis of prospective studies. Sleep. 2010;33:585–92. doi: 10.1093/sleep/33.5.585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ayas NT, White DP, Manson JE, et al. A prospective study of sleep duration and coronary heart disease in women. Arch Intern Med. 2003;163:205–9. doi: 10.1001/archinte.163.2.205. [DOI] [PubMed] [Google Scholar]
- 3.Marshall NS, Glozier N, Grunstein RR. Is sleep duration related to obesity? A critical review of the epidemiological evidence. Sleep Med Rev. 2008;12:289–98. doi: 10.1016/j.smrv.2008.03.001. [DOI] [PubMed] [Google Scholar]
- 4.Zager A, Andersen ML, Ruiz FS, et al. Effects of acute and chronic sleep loss on immune modulation of rats. Am J Physiol Regul Integr Comp Physiol. 2007;293:R504–9. doi: 10.1152/ajpregu.00105.2007. [DOI] [PubMed] [Google Scholar]
- 5.Niederberger C. Re: Impairment of male reproductive function after sleep deprivation. J Urol. 2015;194:1712. doi: 10.1016/j.juro.2015.09.046. [DOI] [PubMed] [Google Scholar]
- 6.Swan SH, Elkin EP, Fenster L. Have sperm densities declined? A reanalysis of global trend data. Environ Health Perspect. 1997;105:1228–32. doi: 10.1289/ehp.971051228. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Jensen TK, Andersson AM, Skakkebæk NE, et al. Association of sleep disturbances with reduced semen quality: A cross-sectional study among 953 healthy young Danish men. Am J Epidemiol. 2013;177:1027–37. doi: 10.1093/aje/kws420. [DOI] [PubMed] [Google Scholar]
- 8.Besedovsky L, Lange T, Born J. Sleep and immune function. Pflugers Arch. 2012;463:121–37. doi: 10.1007/s00424-011-1044-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hui L, Hua F, Diandong H, Hong Y. Effects of sleep and sleep deprivation on immunoglobulins and complement in humans. Brain Behav Immun. 2007;21:308–10. doi: 10.1016/j.bbi.2006.09.005. [DOI] [PubMed] [Google Scholar]
- 10.Purvis K, Magnus O, Mørkås L, et al. Ejaculate composition after masturbation and coitus in the human male. Int J Androl. 1986;9:401–6. doi: 10.1111/j.1365-2605.1986.tb00902.x. [DOI] [PubMed] [Google Scholar]
- 11.Cooper TG, Noonan E, von Eckardstein S, et al. World Health Organization reference values for human semen characteristics. Hum Reprod Update. 2010;16:231–45. doi: 10.1093/humupd/dmp048. [DOI] [PubMed] [Google Scholar]
- 12.Hirshkowitz M, Whiton K, Albert SM, et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health. 2015;1:40–43. doi: 10.1016/j.sleh.2014.12.010. [DOI] [PubMed] [Google Scholar]
- 13.Singh NP, Muller CH, Berger RE. Effects of age on DNA double-strand breaks and apoptosis in human sperm. Fertil Steril. 2003;80:1420–30. doi: 10.1016/j.fertnstert.2003.04.002. [DOI] [PubMed] [Google Scholar]
- 14.Davis RO, Gravance CG. Consistency of sperm morphology classification methods. J Androl. 1994;15:83–91. [PubMed] [Google Scholar]
- 15.Buxton OM, Marcelli E. Short and long sleep are positively associated with obesity, diabetes, hypertension, and cardiovascular disease among adults in the United States. Soc Sci Med. 2010;71:1027–36. doi: 10.1016/j.socscimed.2010.05.041. [DOI] [PubMed] [Google Scholar]
- 16.Sabanayagam C, Shankar A. Sleep duration and cardiovascular disease: Results from the National Health Interview Survey. Sleep. 2010;33:1037–42. doi: 10.1093/sleep/33.8.1037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kant AK, Graubard BI. Association of self-reported sleep duration with eating behaviors of American adults: NHANES 2005–2010. Am J Clin Nutr. 2014;100:938–47. doi: 10.3945/ajcn.114.085191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Taylor BJ, Matthews KA, Hasler BP, et al. Bedtime variability and metabolic health in midlife women: The SWAN Sleep Study. Sleep. 2016;39:457–65. doi: 10.5665/sleep.5464. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sakamoto N, Nanri A, Kochi T, et al. Bedtime and sleep duration in relation to depressive symptoms among Japanese workers. J Occup Health. 2013;55:479–86. doi: 10.1539/joh.13-0074-oa. [DOI] [PubMed] [Google Scholar]
- 20.Janevic T, Kahn LG, Landsbergis P, et al. Effects of work and life stress on semen quality. Fertil Steril. 2014;102:530–38. doi: 10.1016/j.fertnstert.2014.04.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wogatzky J, Wirleitner B, Stecher A, et al. The combination matters – distinct impact of lifestyle factors on sperm quality: A study on semen analysis of 1683 patients according to MSOME criteria. Reprod Biol Endocrinol. 2012;10:115. doi: 10.1186/1477-7827-10-115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cheek RE, Shaver JL, Lentz MJ. Variations in sleep hygiene practices of women with and without insomnia. Res Nurs Health. 2004;27:225–36. doi: 10.1002/nur.20025. [DOI] [PubMed] [Google Scholar]
- 23.Jefferson CD, Drake CL, Scofield HM, et al. Sleep hygiene practices in a population-based sample of insomniacs. Sleep. 2005;28:611–15. doi: 10.1093/sleep/28.5.611. [DOI] [PubMed] [Google Scholar]
- 24.Naz RK. Vaccine for human contraception targeting sperm Izumo protein and YLP12 dodecamer peptide. Protein Sci. 2014;23:857–68. doi: 10.1002/pro.2476. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Cui D, Han G, Shang Y, et al. Antisperm antibodies in infertile men and their effect on semen parameters: A systematic review and meta-analysis. Clin Chim Acta. 2015;444:29–36. doi: 10.1016/j.cca.2015.01.033. [DOI] [PubMed] [Google Scholar]
- 26.Silva CA, Cocuzza M, Carvalho JF, Bonfá E. Diagnosis and classification of autoimmune orchitis. Autoimmun Rev. 2014;13:431–34. doi: 10.1016/j.autrev.2014.01.024. [DOI] [PubMed] [Google Scholar]
- 27.Agarwal A, Deepinder F, Cocuzza M, et al. Efficacy of varicocelectomy in improving semen parameters: new meta-analytical approach. Urology. 2007;70:532–38. doi: 10.1016/j.urology.2007.04.011. [DOI] [PubMed] [Google Scholar]
- 28.Wang YX, Zhu WJ, Jiang H. Sperm exposure during menses is a risk factor for developing antisperm antibody (ASA) in female. Arch Gynecol Obstet. 2013;288:1145–48. doi: 10.1007/s00404-013-2883-z. [DOI] [PubMed] [Google Scholar]