

Abstract
Background:
Firefighters for difficult activities and rescue of damaged people must be in appropriate physical ability. Maximal oxygen capacity is an indicator for diagnosis of physical ability of workers. This study aimed to assess the cardiorespiratory system and its related factors in firefighters.
Methods:
This study was conducted on 110 firefighters from various stations. An self-administered questionnaire (respiratory disorders questionnaire, Tuxworth-Shahnavaz step test, and pulmonary function test) was used to collection of required data. Average of humidity and temperature was 52% and 17°C, respectively. Background average noise levels were between 55 and 65 dB. Data were analyzed using SPSS software (version 19).
Results:
The mean age of the study participants was 32 ± 6.2 years. The means of forced vital capacity (FVC), forced expiratory volume in 1 s (FEV1), and FEV1/FVC were 92% ±9.4%, 87% ±9.2%, and 80% ±6.1%, respectively. The participants’ mean VO2-max was 2.79 ± 0.29 L/min or 37.34 ± 4.27 ml/kg body weight per minute. The results revealed that weight has a direct association with vital capacity (VC), FVC, and peak expiratory flow. In addition, height was directly associated with VC, FVC, and VO2-max (P < 0.05). However, there was an inverse and significant association between height and FEV1/FVC (r = −0.23, P < 0.05). Height, weight, body mass index, and waist circumference were directly associated with VO2-max.
Conclusions:
The findings of this study showed that the amount of maximum oxygen consumption is close with the proposed range of this parameter among firefighters in other studies. Furthermore, the results of the study revealed that individuals had normal amounts of lung volume index. This issue can be attributed to the appropriate usage of respiratory masks.
Keywords: Firefighter, maximal oxygen consumption, respiratory volume
Introduction
Firefighters and aid workers are considered to be victims of heat stress in physiological activities.[1] Moving and lifting heavy objects or saving people under stressful conditions are such activates done by firefighters while wearing protective clothes and a compressed air breathing apparatus.[2] Accordingly, they need to have appropriate physical structure to perform their duties properly.[3,4] Numerous studies indicated that individuals’ appropriate physical performance depends on VO2-max, which is defined as the maximum amount of oxygen that can be absorbed by the respiratory system and be sent to operating muscles.[5,6,7] Previous studies showed that VO2-max ranged from 33.5 to 45 ml/kg body weight per minute among firefighters.[8,9] Based on Kiss et al.'s study conducted in Belgium, the rate of VO2-max was estimated to be 46.5 ml/kg body weight per minute among firefighters.[10]
Moreover, pulmonary function test or spirometry is identified as another method to assess cardiorespiratory system's health. Spirometry is the most common pulmonary function test, giving the rate, volume, speed, or flow of an individual's inhalation and exhalation. The test consists of three main parameters, namely, forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC), and FEV1/FVC. FVC refers to the amount of air an individual exhales from one's lung after a deep inhalation. FEV1 is also defined as the amount of air an individual forcefully exhales from one's lung in the first second of exhalation. Finally, FEV1/FVC is the ratio of the second to the first parameter and indicates the percentage of FVC exhaled from lung in the first second of exhalation.[11]
In comparison with the society, firefighters have better pulmonary function, particularly in FVC and FEV1 parameters.[12,13] However, due to the increase in utilization of chemical materials in buildings in the recent decades, concerns have risen about this group's health.[14] Regarding the results of some studies, exposure to smoke and fumes[15,16] including acrolein, carbon monoxide, hydrogen chloride, hydrogen cyanide, nitrogen oxides, sulfur dioxide, particles, aldehydes, and carcinogens led to chronic pulmonary damages followed by reduction of pulmonary function.[13,15,16,17,18,19] Numerous studies revealed the acute effects of exposure to smoke on firefighters’ health, particularly pulmonary function. For instance, according to a study conducted on 28 firefighters, a considerable obstructive pulmonary disease within few hours after exposure to smoke was found.[20] In addition, the findings of Musk et al. revealed that occurs a significant reduction in FEV1 among smoker peoples.[15]
Considering what was mentioned above and firefighters’ heavy physical requirements, it is essential to assess their cardiorespiratory function accurately. Hence, this study aimed to investigate respiratory complications and assess of VO2-max, lung volumes, and their associated factors among firefighters in one of the central cities of Fars province, Iran.
Methods
This is a cross-sectional study on firefighters who were participating in fire suppression and rescue operations in one of the central cities of Fars province, Iran. Using a systematic random sampling approach and based on a priori sample size calculation, 110 firefighters were selected from various stations among which 104 participants agreed to participate in all the stages of the research. All participants with at least 1 year of working experience were interviewed and those with any history of cardiovascular or respiratory disorders and smoking were excluded from the study.
An self-administered questionnaire was used to collect information on the participant's demographic and respiratorystatus. This questionnaire used in several studies and its reliability and validity have been approved. It also employed in several studies in Iran.[12,21,22,23,24,25]
Procedure
Pulmonary function tests were measured based on ATS’ guidelines using a spirometer (Vitalograph Compact II, England). Given device was calibrated each day and after per 10 tests. Three acceptable spirometry maneuvers, therefore, were obtained from each participant and the best one was recorded. VO2-max was evaluated using the protocol developed by Tuxworth-Shahnavaz on an Iranian society in 1977.[26] In this protocol, individuals go up and down step (height: 40 cm) with a cadence of 25 times in a minute for 5 min. Then, they sit on a chair, their heart rate is measured in three 30 s stages (M1: 30–60 s, M2: 90–120 s, and M3: 150–180 s [Figure 1]), and VO2-max is computed using the following equations.
Figure 1.
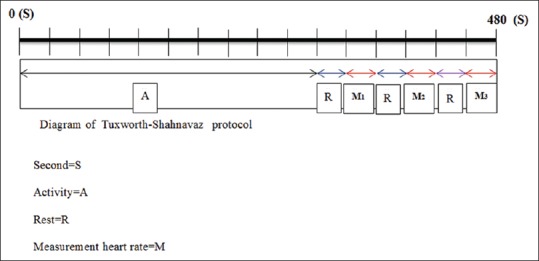
Diagram of Tuxworth-Shahnavaz Protocol
Index 
Index b → Y = −0.378X + 4.67
At the end of the interview, anthropometric indexes (weight and height) were measured. Participants with minimal clothing and no wearing shoes were weighed with a calibrated digital platform Balance Scale (Imperial BS 412, US) and the numbers were rounded to the nearest 100 g. Height was measured while the participants were in standing position with the shoulders in a normal resting and also 3 regions of their body (buttocks, heel, and head) touching the wall, without wearing shoes. In addition, temperature and relative humidity were measured using thermometer, spinning thermometer (Casella, England), and psychrometric chart. Environmental measurements indicated that the mean humidity was 52 and the mean temperature was 17°C. Moreover, the noise of environment was measured using sound level meter (model TES-1351) manufactured by Taiwan.
Statistical analysis
The sample size was calculated to detect at least 2.3 kg change in weight with alpha value of 0.05 and a power of 80%. Data were analyzed using Statistical Package for Social Sciences 19 (SPSS Inc, Chicago, IL, USA). The main study variables included both quantitative (age, height, weight, waist circumference, body mass index [BMI], and job tenure in firefighting) and qualitative measures (marital status, level of education, second job, and job satisfaction). Pearson's correlation coefficient was used to assess the association between demographic and anthropometric variables with respiratory volume and maximal oxygen consumption.
Results
The demographic and environmental characteristics of participants are shown in Table 1. Environmental measurements indicated that the mean humidity was 52 and the mean temperature was 17°C. Based on Table 2, more than 80% of the participants had no respiratory disorders. The lung volumes and VO2-max of the study participants are shown in Table 3. Accordingly, the means of FVC, FEV1, and FEV1/FVC were 92% ±9.4%, 87% ±9.2%, and 80% ±6.1%, respectively. The mean of VO2-max was 2.79% ±0.29 L/min or 37.34 ± 4.27 ml/kg body weight per minute.
Table 1.
Some demographic characteristics of the studied fire-fighting personnel (n=110)

Table 2.
Distribution of respiratory complications among studied fire-fighting personnel (n=110)

Table 3.
Mean, standard deviation, minimum and maximum lung volumes, and maximal oxygen consumption of studied fire-fighting personnel (n=110)

The results of Table 4 show a significant association between age and peak expiratory flow (PEF) (r = 0.19, P = 0.045). In addition, height was directly associated with vital capacity (VC) (r = 0.23, P = 0.016), FVC (r = 0.26, P = 0.007), and VO2-max (r = 0.39, P = 0.001). However, there was an inverse and significant association between height and FEV1/FVC (r = −0.23, P = 0.017). Moreover, a significant and direct association between weight and FVC (r = 0.20, P = 0.034), PEF (r = 0.24, P = 0.012), and VO2-max (r = 0.53, P = 0.001). In addition, the finding revealed a significant direct association between BMI and VO2-max (r = 0.39, P = 0.001). Finally, waist circumference showed a significant direct association with VO2-max (r = 0.33, P = 0.001).
Table 4.
Association between demographic variables with respiratory volume and maximal oxygen consumption

Discussion
This is a cross-sectional study that examined the relationship between some factors linked to individuals’ capabilities with the cardiorespiratory factors. Moreover, considering the importance of pulmonary function tests in diagnosis and treatment of respiratory disorders, determination of normal lung volumes is essential in different societies.[27] In addition to lung volumes, determination of VO2-max seems to play an important role in occupational ergonomics. However, few studies have been conducted in this area among firefighters. As a result, the effective factors in VO2-max have remained unknown.
The aim of this study was to investigate cardiorespiratory health among firefighters in one of the central cities of Fars province, Iran. Accordingly, the mean of FVC, FEV1, and FEV1/FVC was normal which is in accordance with the report published by Michael et al.[28] Based on the Sharifian's findings, FVC was lower in Iran compared to European and American countries.[29] Based on the results from a study conducted by Alizadeh, height is one of the effective factors in lung volumes.[30] Accordingly, the lower lung volumes in the present study which is not in accordance with the Michael's finding[28] might be attributed to height differences between both societies.
In the current study, the firefighters’ main complaints included shortness of breath followed by phlegm and cough, which is consistent with the findings of the study by Rothman et al.[31] In addition, Rahimi Moghaddam (2014) suggested that the most frequent complaints were phlegm, wheezing, and cough among welders.[32] Aminian also showed that cough is the most common complaint among the individuals working in textile industries.[33]
The results of the present study showed a significant and direct association between age and PEF, whereas other studies could not find such direct associations.[34,35] In contrast, Aldrich et al. (2010) reported a 25 ml decrease in FEV1 each year after exposure.[36] Accordingly, significant reduction of these parameters with age is most probably due to their unprotected exposure to smoke.
In the present study, height was significantly and inversely associated with VC and FVC. Weight, on the other hand, showed direct association with VC, FVC, and PEF which are in accordance with the result of a study conducted by Alizade et al.[30] Mehrabi and Kargarfard on the other hand found an inverse association between weight and lung volumes.[37] It could be attributed to overweight resulting from fat tissues and lack of physical activity among the participants. According to the results of the present study, participants had high BMI due to increase in their muscle mass resulting from regular physical activities. Regarding the findings from the Spathopoulos et al.,[38] Gundogdu and Eryilmaz,[39] and Furutate et al. (2011),[40] excess fat tissues hinder appropriate pulmonary function that can, in turn, affect cardiovascular function. Sothmann et al. suggested that VO2-max ranges should be from 33.5 to 42 ml/kg body weight per minute among firefighters.[41] However, the previous studies raised some controversial issues over the VO2-max values and suggested that certain circumstance including physical, mental, environmental, and physiological factors[42,43] of different individuals might be significantly different.[44] Role of the protocol utilized in the current study should be taken into account as well. In this study, the researchers made use of Tuxworth-Shahnavaz protocol that has been proposed for Iranian communities. Furthermore, the difference between the results of our study and the one performed by Kianmehr and Nazem[45] might be attributed to the participants’ mean age because VO2-max decreases with increase in age[46,47,48] and the highest amount of VO2-max has been observed in the age range of 18–25 years.[42]
Results of the present study indicate a significant and direct association between height, weight, BMI, and waist circumference with VO2-max. These results are not fully in accordance with a report published by Daneshmandi et al. detected a direct but not significant association between height and VO2-max.,[49] The authors suggested that reduction in VO2-max decrease height due to change in muscles’ structure[50,51,52,53,54] and faded the relationship between height and VO2-max.
Although the present study findings demonstrated a descending trend in VO2-max with increase in age, the association was not significant. Previous studies indicated a considerable decrease in VO2-max with increase in age.[46,47,48] The nonsignificant association observed in the current study might be attributed to the participants’ small age range, which might have faded the effect of age. Furthermore, VO2-max was significantly lower in the individuals with normal BMI compared to those with high BMI. However, the results of the study conducted by Daneshmandi et al. (2013) revealed an inverse linear relationship between VO2-max and BMI (r = −0.158). What's more, VO2-max was higher in the individuals with normal BMI in comparison to overweight and obese ones.[49]
Conclusions
The ability of people to do their job is influenced by the person's capabilities, the job demand, and the condition under which the person is carrying out the job. The findings of this study showed that the amount of maximum oxygen consumption is close with the proposed range of this parameter among firefighters in other studies. Furthermore, the results of the study revealed that participants had normal amounts of lung volume index. This issue can be attributed to the appropriate usage of respiratory masks.
Financial support and sponsorship
The present study was financially supported by Shiraz University of Medical Sciences, Shiraz, Iran.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
The present study is a part of MSc thesis: “Evaluation cardiorespiratory fitness and some related factors in fire-fighting personnel, 2015” written by Touraj Khazraee under supervision of Dr. Zahra Zamanian. The present study was financially supported by Shiraz University of Medical Sciences, Shiraz, Iran. (Design No.: 7414).
References
- 1.Bishop P, Ray P, Reneau P. A review of the ergonomics of work in the US military chemical protective clothing. Int J Ind Ergon. 1995;15:271–83. [Google Scholar]
- 2.Baker SJ, Grice J, Roby L, Matthews C. Cardiorespiratory and thermoregulatory response of working in fire-fighter protective clothing in a temperate environment. Ergonomics. 2000;43:1350–8. doi: 10.1080/001401300421798. [DOI] [PubMed] [Google Scholar]
- 3.Holloszy JO, Schultz J, Kusnierkiewicz J, Hagberg JM, Ehsani AA. Effects of exercise on glucose tolerance and insulin resistance. Brief review and some preliminary results. Acta Med Scand Suppl. 1986;711:55–65. doi: 10.1111/j.0954-6820.1986.tb08932.x. [DOI] [PubMed] [Google Scholar]
- 4.Manning JE, Griggs TR. Heart rates in fire fighters using light and heavy breathing equipment: Similar near-maximal exertion in response to multiple work load conditions. J Occup Environ Med. 1983;25:215–8. doi: 10.1097/00043764-198303000-00016. [DOI] [PubMed] [Google Scholar]
- 5.Wilson JR, Sharples S. Evaluation of Human Work. Florida: CRC Press; 2015. [Google Scholar]
- 6.Mououdi M, Choobineh A. Ergonomics in practice: Selected ergonomics topics. Tehran: Nashr-e-Markaz; 1999. pp. 81–94. [Google Scholar]
- 7.Zou AV, Marvi N, Ahmadi Behzad MS, Houspian V. Vo2 max estimation for pupils by aerobic octal test (AOT) Olympic. 2010;4:7–17. [Google Scholar]
- 8.Bilzon JL, Scarpello EG, Smith CV, Ravenhill NA, Rayson MP. Characterization of the metabolic demands of simulated shipboard Royal Navy fire-fighting tasks. Ergonomics. 2001;44:766–80. doi: 10.1080/00140130118253. [DOI] [PubMed] [Google Scholar]
- 9.Lee JY, Bakri I, Kim JH, Son SY, Tochihara Y. The impact of firefighter personal protective equipment and treadmill protocol on maximal oxygen uptake. J Occup Environ Hyg. 2013;10:397–407. doi: 10.1080/15459624.2013.792681. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kiss P, De Meester M, Maes C, De Vriese S, Kruse A, Braeckman L. Cardiorespiratory fitness in a representative sample of Belgian firefighters. Occup Med (Lond) 2014;64:589–94. doi: 10.1093/occmed/kqu138. [DOI] [PubMed] [Google Scholar]
- 11.Arefnasab Z, Ghanei M, Noorbala AA, Alipour A, Babamahmoodi A. Correlation of spirometry and health-related quality of life with mental health in respiratory chemical damaged veterans. J Mazandaran Univ Med Sci. 2013;23:49–56. [Google Scholar]
- 12.Sidor R, Peters JM. Fire fighting and pulmonary function. An epidemiologic study. Am Rev Respir Dis. 1974;109:249–54. doi: 10.1164/arrd.1974.109.2.249. [DOI] [PubMed] [Google Scholar]
- 13.Douglas DB, Douglas RB, Oakes D, Scott G. Pulmonary function of London firemen. Br J Ind Med. 1985;42:55–8. doi: 10.1136/oem.42.1.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Brandt-Rauf PW, Cosman B, Fallon LF, Jr, Tarantini T, Idema C. Health hazards of firefighters: Acute pulmonary effects after toxic exposures. Br J Ind Med. 1989;46:209–11. doi: 10.1136/oem.46.3.209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Musk AW, Smith TJ, Peters JM, McLaughlin E. Pulmonary function in firefighters: Acute changes in ventilatory capacity and their correlates. Br J Ind Med. 1979;36:29–34. doi: 10.1136/oem.36.1.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Unger KM, Snow RM, Mestas JM, Miller WC. Smoke inhalation in firemen. Thorax. 1980;35:838–42. doi: 10.1136/thx.35.11.838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Chia KS, Jeyaratnam J, Chan TB, Lim TK. Airway responsiveness of firefighters after smoke exposure. Br J Ind Med. 1990;47:524–7. doi: 10.1136/oem.47.8.524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Axford AT, McKerrow CB, Jones AP, Le Quesne PM. Accidental exposure to isocyanate fumes in a group of firemen. Br J Ind Med. 1976;33:65–71. doi: 10.1136/oem.33.2.65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Loke J, Farmer W, Matthay RA, Putman CE, Smith GJ. Acute and chronic effects of fire fighting on pulmonary function. Chest. 1980;77:369–73. doi: 10.1378/chest.77.3.369. [DOI] [PubMed] [Google Scholar]
- 20.Whitener DR, Whitener LM, Robertson KJ, Baxter CR, Pierce AK. Pulmonary function measurements in patients with thermal injury and smoke inhalation. Am Rev Respir Dis. 1980;122:731–9. doi: 10.1164/arrd.1980.122.5.731. [DOI] [PubMed] [Google Scholar]
- 21.Surag MK, Sudhir U. A study of pulmonary function abnormalities in patients with type 2 diabetes mellitus. IOSR-JDMS. 2016;15:46–54. [Google Scholar]
- 22.Sidor R, Peters JM. Prevalence rates of chronic non-specific respiratory disease in fire fighters. Am Rev Respir Dis. 1974;109:255–61. doi: 10.1164/arrd.1974.109.2.255. [DOI] [PubMed] [Google Scholar]
- 23.Ferris BG. Epidemiology standardization project (American Thoracic Society) Am Rev Respir Dis. 1978;118(6 Pt 2):1. [PubMed] [Google Scholar]
- 24.Neghab M, Soltanzade A, Alipor A. Evaluation of spirometry and respiratory complaints in workers exposed to flour. Iran Occup Health. 2010;1:2–7. [Google Scholar]
- 25.Neghab M, Chobine A. The relationship between occupational exposure to cement dust and prevalence of respiratory symptoms and disorders. J Kermanshah Univ Med Sci. 2007;11:215–26. [Google Scholar]
- 26.Tuxworth W, Shahnawaz H. The design and evaluation of a step test for the rapid prediction of physical work capacity in an unsophisticated industrial work force. Ergonomics. 1977;20:181–91. doi: 10.1080/00140137708931616. [DOI] [PubMed] [Google Scholar]
- 27.Zoladz JA, Szkutnik Z, Majerczak J, Duda K, Pedersen PK. Non-linear relationship between oxygen uptake and power output in the Astrand nomogram-old data revisited. J Physiol Pharmacol. 2007;58:265–73. [PubMed] [Google Scholar]
- 28.Weiden MD, Ferrier N, Nolan A, Rom WN, Comfort A, Gustave J, et al. Obstructive airways disease with air trapping among firefighters exposed to World Trade Center dust. Chest. 2010;137:566–74. doi: 10.1378/chest.09-1580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sharifian A, Sigari N, Rahimi E, Yazdanpanah K. Evaluation of normal pulmonary function test (spirometry) people of Kurdistan. Kurdistan Univ Med Sci. 2007;12:1–8. [Google Scholar]
- 30.Alizade A, Etemadinejad S, Mohamadpor R. Comparison of spirometry measurements in healthy individuals older than 18 years with global standards of residents in Sari, 2001. Mazandaran Univ Med Sci. 2006;55:65–71. [Google Scholar]
- 31.Rothman N, Ford DP, Baser ME, Hansen JA, O’Toole T, Tockman MS, et al. Pulmonary function and respiratory symptoms in wildland firefighters. J Occup Environ Med. 1991;33:1163–7. doi: 10.1097/00043764-199111000-00013. [DOI] [PubMed] [Google Scholar]
- 32.Rahimi Moghaddam S. Changes in spirometricindices among welders of a water heater making factory in Neyshabur, Iran after four years. J Health Dev. 2014;3:38–47. [Google Scholar]
- 33.Aminian O, Mozafari SA, Sharifian SA, Rokni M, Ahmadzade F, Heidarian H. Evaluation of respiratory symptoms and spirometric indicators in the ghaem shahr city of textile workers. Occup Med. 2011;3:46–51. [Google Scholar]
- 34.Horsfield K, Guyatt AR, Cooper FM, Buckman MP, Cumming G. Lung function in West Sussex firemen: A four year study. Br J Ind Med. 1988;45:116–21. doi: 10.1136/oem.45.2.116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Burgess JL, Brodkin CA, Daniell WE, Pappas GP, Keifer MC, Stover BD, et al. Longitudinal decline in measured firefighter single-breath diffusing capacity of carbon monoxide values. A respiratory surveillance dilemma. Am J Respir Crit Care Med. 1999;159:119–24. doi: 10.1164/ajrccm.159.1.9804153. [DOI] [PubMed] [Google Scholar]
- 36.Aldrich TK, Gustave J, Hall CB, Cohen HW, Webber MP, Zeig-Owens R, et al. Lung function in rescue workers at the World Trade Center after 7 years. N Engl J Med. 2010;362:1263–72. doi: 10.1056/NEJMoa0910087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Mehrabi E, Kargarfard M. Compare spirometric parameters compared to of normal weight to obese female middle school students. Ahvaz Univ Med Sci. 2013;12:541–5. [Google Scholar]
- 38.Spathopoulos D, Paraskakis E, Trypsianis G, Tsalkidis A, Arvanitidou V, Emporiadou M, et al. The effect of obesity on pulmonary lung function of school aged children in Greece. Pediatr Pulmonol. 2009;44:273–80. doi: 10.1002/ppul.20995. [DOI] [PubMed] [Google Scholar]
- 39.Gundogdu Z, Eryilmaz N. Correlation between peak flow and body mass index in obese and non-obese children in Kocaeli, Turkey. Prim Care Respir J. 2011;20:403–6. doi: 10.4104/pcrj.2011.00061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Furutate R, Ishii T, Wakabayashi R, Motegi T, Yamada K, Gemma A, et al. Excessive visceral fat accumulation in advanced chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2011;6:423–30. doi: 10.2147/COPD.S22885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Sothmann MS, Saupe K, Jasenof D, Blaney J. Heart rate response of firefighters to actual emergencies: Implications for cardiorespiratory fitness. J Occup Environ Med. 1992;34:797–800. doi: 10.1097/00043764-199208000-00014. [DOI] [PubMed] [Google Scholar]
- 42.Tayyari F, Smith JL. Occupational Ergonomics: Principles and Applications. London: Chapman & Hall; 1997. [Google Scholar]
- 43.Wilmore JH, Costill DL, Gleim GW. Physiology of sport and exercise. Med Sci Sports Exerc. 1995;27:792. [Google Scholar]
- 44.von Heimburg E, Medbø JI. Energy cost of the Trondheim firefighter test for experienced firefighters. Int J Occup Saf Ergon. 2013;19:211–25. doi: 10.1080/10803548.2013.11076980. [DOI] [PubMed] [Google Scholar]
- 45.Kianmehr P, Nazem F. Evaluation of validity and capability of professional function test of Iranian firemen. J Mil Med. 2011;13:147–53. [Google Scholar]
- 46.Huggett DL, Connelly DM, Overend TJ. Maximal aerobic capacity testing of older adults: A critical review. J Gerontol Ser A Biol Sci Med Sci. 2005;60:57–66. doi: 10.1093/gerona/60.1.57. [DOI] [PubMed] [Google Scholar]
- 47.Yoopat P, Toicharoen P, Boontong S, Glinsukon T, Vanwonterghem K, Louhevaara V. Cardiorespiratory capacity of Thai workers in different age and job categories. J Physiol Anthropol Appl Human Sci. 2002;21:121–8. doi: 10.2114/jpa.21.121. [DOI] [PubMed] [Google Scholar]
- 48.Rodahl K. Physiology of Work. New York: CRC Press; 2003. [Google Scholar]
- 49.Daneshmandi H, Fard AR, Choobineh A. Estimation of aerobic capacity and determination of its associated factors among male workers of industrial sector of Iran. Int J Occup Saf Ergon. 2013;19:667–73. doi: 10.1080/10803548.2013.11077014. [DOI] [PubMed] [Google Scholar]
- 50.Goldspink G. Age-related muscle loss and progressive dysfunction in mechanosensitive growth factor signaling. Ann N Y Acad Sci. 2004;1019:294–8. doi: 10.1196/annals.1297.050. [DOI] [PubMed] [Google Scholar]
- 51.Janssen I, Heymsfield SB, Wang ZM, Ross R. Skeletal muscle mass and distribution in 468 men and women aged 18-88 yr. J Appl Physiol. 2000;89:81–8. doi: 10.1152/jappl.2000.89.1.81. [DOI] [PubMed] [Google Scholar]
- 52.Larsson L, Yu F, Höök P, Ramamurthy B, Marx JO, Pircher P. Effects of aging on regulation of muscle contraction at the motor unit, muscle cell, and molecular levels. Int J Sport Nutr Exerc Metab. 2001;11:S28–43. doi: 10.1123/ijsnem.11.s1.s28. [DOI] [PubMed] [Google Scholar]
- 53.Owino V, Yang SY, Goldspink G. Age-related loss of skeletal muscle function and the inability to express the autocrine form of insulin-like growth factor-1 (MGF) in response to mechanical overload. FEBS Lett. 2001;505:259–63. doi: 10.1016/s0014-5793(01)02825-3. [DOI] [PubMed] [Google Scholar]
- 54.Pahor M, Kritchevsky S. Research hypotheses on muscle wasting, aging, loss of function and disability. J Nutr Health Aging. 1998;2:97–100. [PubMed] [Google Scholar]