

Abstract
Background:
Shaving the donor area is one of the major deterrents preventing hair transplant patients from selecting follicular unit extraction (FUE). A minimal shaved donor area is possible in strip surgery, but the strip method is not applicable if the patient wishes to avoid a linear donor scar, wishes to minimize postoperative pain, or has insufficient scalp laxity. In these cases, nonshaven FUE (NS-FUE) is potentially a very good choice.
Methods:
A total of 42 patients were enrolled. Both pretrimmed and direct NS-FUE were performed during a single session in each patient. The 2 methods were compared regarding the time taken to punch 50 grafts, transection rate, and calculated density (number of hairs per graft).
Results:
The mean time taken to punch 50 grafts was significantly longer in the pretrimmed method than the direct method (3.4 minutes versus 2.6 minutes; P < 0.001). The mean transection rate was similar in both methods (8.8% for the pretrimmed method and 7.5% for the direct method; P > 0.05). The mean calculated density was significantly higher in the pretrimmed method than the direct method (2.23 hairs per graft versus 2.15 hairs per graft; P < 0.05). The length of the harvested hair was 1–4 mm in the pretrimmed method, compared with 0.4–0.8 mm in the direct method.
Conclusion:
Depending on the proficiency and preference of doctors and the case indications, pretrimmed and direct NS-FUE are both useful techniques for hair transplantation.
INTRODUCTION
Follicular unit extraction (FUE) was introduced by Rassman and Bernstein1 in 2002, and the technique has considerably progressed since then. FUE is becoming increasingly popular. The worldwide census for hair transplantation estimated that there were 397,048 hair transplantation procedures conducted in 2014 (a 28% increase from 2012), and 48.5% of these procedures were FUE surgeries.2
FUE is associated with advantages and disadvantages. FUE does not create a linear donor scar and causes minimal postoperative pain. In addition, a lot of hair can be transplanted, even if the donor scalp is rigid; hence, FUE is the chosen method when the donor scalp has minimal laxity. However, in FUE, the donor area must be shaved, which is a major deterrent preventing people from selecting FUE hair transplantation. Only a thin line of the donor head is shaved in strip surgery, but the strip method creates a linear donor scar and more postoperative pain. To avoid a linear donor scar and minimize postoperative pain while still avoiding shaving, nonshaven FUE (NS-FUE) can be a very good choice.
The 2 methods of NS-FUE are the pretrimmed method and the direct method.3,4 In the pretrimmed method, the hair that is to be transplanted is selectively trimmed using iris scissors before the hair follicle is removed by punching. In the direct method, the spinning tip of the motorized punch trims the hair so that the trimming and punching are performed simultaneously.
The present study compared the outcomes of NS-FUE via the pretrimmed versus the direct method to determine the advantages and disadvantages of each. This information will help surgeons choose the most appropriate method for each individual case.
MATERIALS AND METHODS
A total of 42 patients were enrolled, with a mean age of 34.4 years (range, 22–58 years). There were 32 cases of male pattern baldness, 2 cases of female pattern hair loss, and 8 cases of female hairline correction. All patients were Asians with black hair.
To enable comparison under the same conditions, a vertical line was drawn from 1 external acoustic meatus to the other external acoustic meatus in each patient, and the area was divided into 8 zones of 3.5 cm × 5 cm (4 zones on each side). The zones were numbered from 1 to 8 from left to right (Fig. 1). The 8 zones were drawn in the donor area using a marker pen during a preoperative consultation. The zone designated as the pretrimmed zone was randomly selected from either the fourth or the fifth zone. Trimming was performed with iris scissors with a narrow and sharp tip using a ×5.5 magnifying loupe. Among the thick anagen hairs, we mainly trimmed multifollicular units. The patient was then sterilely draped while in a sitting position. After injection of local anesthesia(1:100,000 epinephrine mixed lidocaine), a tumescent solution was injected into the punching site.
Fig. 1.
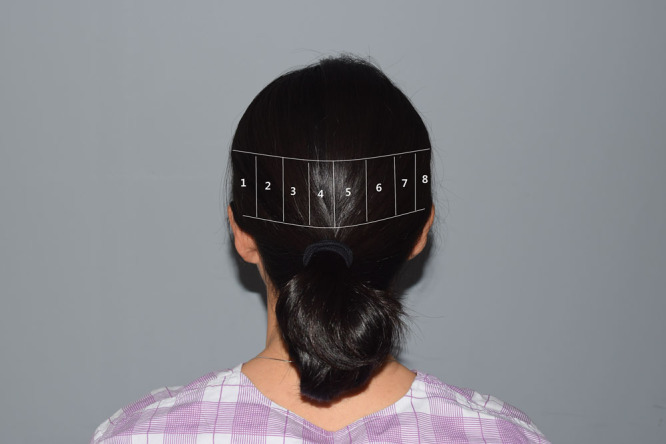
The back of a patient’s head showing the 8 zones used for NS-FUE.
Initially, hair in zones other than the fourth and fifth zones was harvested using the direct method and the pretrimmed method by punching 100 to 200 grafts. This was done to accustom the surgeon’s eye to both methods and remove the bias related to the order in which the 2 methods were performed. This also allowed determination of adequate punching depth for extraction.
The pretrimmed and the direct method were each performed in the fourth or the fifth zone. We harvested 50 follicles from each zone with a Folligraft (Lead M, Seoul, Korea) motorized FUE machine with a 1-mm-sharp punch. A ×5.5 magnifying loupe was used intraoperatively. Punching and extraction were performed with the patient in a sitting position.
Direct NS-FUE
In patients with long hair, 0.7- to 1.0-cm sections of long hair were fixed using multiple clips to ensure a better visual field. In patients with relatively short hair, the surgery was performed by grasping fine jeweler’s forceps with the left hand and the motorized punch handpiece with the right hand. The hair was moved aside with the forceps while direct punching was performed; an assistant helped move the hair aside using a narrow sterile stick or upward traction (Fig. 2). The target hairs that were to be harvested were selected, and then the punch tip was moved over those hairs. Rotation of the punch was started by stepping on the foot pedal. As the punch rotated, it cut the hair and simultaneously entered the skin to rapidly punch out the graft.
Fig. 2.

Intraoperative photograph of the direct method of NS-FUE. As the hair was moved aside with the forceps in the left hand, direct punching was performed with the punch in the right hand. An assistant helped move the hair aside using a narrow sterile stick or upward traction.
Pretrimmed NS-FUE
The donor area was selectively trimmed in advance to a length of 1–2 mm using a magnifying loupe (Fig. 3).
Fig. 3.
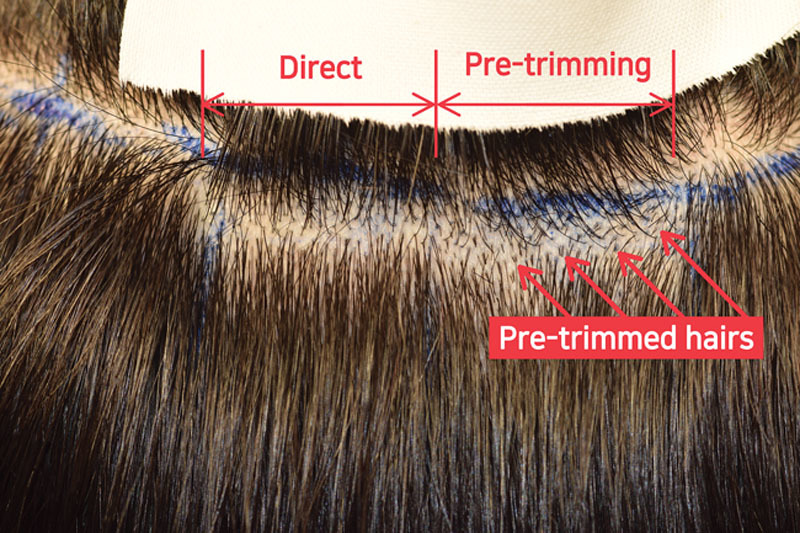
Photograph showing a zone used for direct NS-FUE and a zone used for pretrimmed NS-FUE. In the direct method, the hair angle and direction of the target hair and neighboring hairs are visually similar; this visual guide greatly aids in accurate punching. In contrast, in the pretrimmed method, the pretrimmed target hair exists separately without any visual guidance from the neighboring hairs; each time punching is to be performed on a new target hair, the surgeon’s eyes must readjust.
In both methods, aid to extraction forceps were used for extraction. The extracted follicles were analyzed by a well-experienced hair surgeon using a ×10 microscope. We compared the 2 methods regarding the average time taken to conduct 50 punches, transection rate (TR), and calculated density (CD).
Statistical Analysis
An independent sample t test was conducted to determine the statistical significance of differences between the 2 groups. Differences were considered statistically significant at P < 0.05.
RESULTS
The mean time taken to harvest 50 grafts was significantly longer using the pretrimmed method (3.4 minutes) compared with the direct method (2.6 minutes; t = −6.761, P < 0.001). The mean TR was similar for both methods (8.8% for the pretrimmed method and 7.5% for the direct method; t = −2.454, P > 0.05). The mean CD was significantly greater in the pretrimmed method (2.23 hairs per graft) compared with the direct method (2.15 hairs per graft; t = −2.454, P < 0.05).
In the pretrimmed method, the length of the harvested hair was 1–3 mm according to the pretrimmed length. In contrast, the length of the hair harvested via the direct method was very short (0.4–0.8 mm; Fig. 4).
Fig. 4.

Magnified view of harvested hair obtained via the direct versus the pretrimmed method of NS-FUE. The length of the hair harvested via the pretrimmed method was 1–2 mm or 3–4 mm according to the pretrimmed length. In the direct method, the length of the harvested hair was relatively short (0.4–0.8 mm).
DISCUSSION
Shaving of the donor area is one of the main deterrents that prevents people from choosing to undergo FUE hair transplantation. There are some potential solutions for performing FUE without creating obvious shaved areas. Partial shaving can be a solution when the patient’s own hair is long enough to hide the shaven areas. Microstrip shaving is another potential solution, as FUE can be performed after shaving only 1–3 linear lines of hair. However, using the partial shaving or microstrip shaving techniques makes it difficult to do large areas and it is impossible to collect follicles randomly from a wide donor area. Furthermore, the partial shaving method results in a hypopigmented dot scar concentrated in a small-sized shaven donor site, whereas the microstrip method can potentially cause the appearance of multiple linear scars if 400–600 grafts are collected.3,4
The direct method of NS-FUE does not involve a preoperative hair trimming process, and it takes less time to identify the next target hair after punching. In the present study, the direct method took 24% less time compared with the pretrimmed method; this converts to 1,169 punches per hour using the direct method and 891 punches per hour using the pretrimmed method. However, these are only calculations, whereas in actual practice, it is likely that a lesser number of punches would be possible over the entire hour owing to operator muscle fatigue and time spent moving between punching sites. In clinical practice, we usually perform 700–900 punches per hour via the direct method. Onda et al.5 reported that the direct method took 6 minutes to harvest 100 grafts (which converts to 1,000 punches per hour), and TR was 5.4% using a powered sharp punch. Harris6 reported a TR of 6.14%.
According to our study result, the direct method had a significantly lower CD and similar TR with a significantly faster punching speed. This indicates that there was a slightly lower tendency to target higher follicular units in direct method. Notably, once the operators were skilled in both the pretrimmed and the direct method, there was no difference in TR. This was surprising, as the direct method was expected to have a longer learning curve and a higher TR. This is potentially because in the pretrimmed method, the next target near long hairs must be located by moving aside existing hairs once the punching is completed; because the target hair is hidden by sparsely placed nearby longer hairs, each time a punched hair is targeted, the surgeon’s eyes must adjust to the hair exit angle and direction near the punched hair. The punch must also be moved a further distance to the next target hair in the pretrimmed method than the direct method. In addition, more existing hairs have to be moved aside in the pretrimmed method than the direct method. In the direct method, the hair exit angle and direction of neighboring hairs are the same or similar to target hairs and the extent of bending by gravity is similar when the hair is over a certain length; thus, when punching the target hair, the neighboring hairs could be used as a visual guide.
As the hair harvested by the direct method is very short, we recommend the pretrimmed method when the fine angle of the hair curl has to be adjusted, even though the duration of surgery is extended; examples are side hairline correction and eyebrow or eyelash transplantation.7–10 The pretrimmed method is also preferred in case of transplantation into a hairless area of obese patients, as excessively short hair can cause severe folliculitis by getting buried under the skin folds in areas of the abdomen,7 and transplant survival decreases.11
CONCLUSIONS
The pretrimmed and direct NS-FUE methods are both useful techniques for hair transplantation. The direct method is fast but harvested hairs are very short. The pretrimmed method is slower but harvested hairs are longer, which is better to see the fine angle of the hair curl. The most appropriate method should be selected based on the individual features of the case, the indication, and the availability of suitable operative techniques and skills.
Footnotes
Disclosure: The authors have no financial interest to declare in relation to the content of this article. The Article Processing Charge was paid for by the authors.
REFERENCES
- 1.Rassman WR, Bernstein RM, McClellan R, et al. Follicular unit extraction: minimally invasive surgery for hair transplantation. Dermatol Surg. 2002;28:720–728. [DOI] [PubMed] [Google Scholar]
- 2.Relevant Research, Inc. 2015. International Society of Hair Restoration Surgery: 2015 practice census results. Available at: http://ishrs.org/statistics-research.htm Accessed 2016.
- 3.Park JH. Direct non-shaven FUE technique. Hair Transplant Forum Int’l. 2014;24:103–104.. [Google Scholar]
- 4.Cole JP. State of the art FUE: advanced non-shaven technique. Hair Transplant Forum Int’l 2014;24:161–169.. [Google Scholar]
- 5.Onda M, Igawa HH, Inoue K, et al. Novel technique of follicular unit extraction hair transplantation with a powered punching device. Dermatol Surg. 2008;34:1683–1688.. [DOI] [PubMed] [Google Scholar]
- 6.Harris JA. New methodology and instrumentation for follicular unit extraction: lower follicle transection rates and expanded patient candidacy. Dermatol Surg. 2006;32:56–61.; discussion 61. [DOI] [PubMed] [Google Scholar]
- 7.Tomc CM, Malouf PJ. Eyebrow restoration: the approach, considerations, and technique in follicular unit transplantation. J Cosmet Dermatol. 2015;14:310–314.. [DOI] [PubMed] [Google Scholar]
- 8.Umar S. Eyelash transplantation using leg hair by follicular unit extraction. Plast Reconstr Surg Glob Open. 2015;3:e324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Park JH. Novel principles and techniques to create a natural design in female hairline correction surgery. Plast Reconstr Surg Glob Open. 2015;3:e589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Park JH. Side-hairline correction in Korean female patients. Plast Reconstr Surg Glob Open. 2015;3:e336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Shinmyo LM, Nahas FX, Ferreira LM. Guidelines for pubic hair restoration. Aesthetic Plast Surg. 2006;30:104–107.. [DOI] [PubMed] [Google Scholar]