

Abstract
Background
The elevated vacuum suspension system has demonstrated unique health benefits for amputees, but the effect of vacuum pressure values on gait characteristics is still unclear. The purpose of this study was to investigate the effects of elevated vacuum levels on temporal parameters, kinematics and kinetics for unilateral transtibial amputees.
Methods
Three-dimensional gait analysis was conducted in 9 unilateral transtibial amputees walking at a controlled speed with five vacuum levels ranging from 0–20 inHg, and also in 9 able-bodied subjects walking at self-preferred speed. Repeated ANOVA and Dunnett’s t-test were performed to determine the effect of vacuum level and limb for within subject and between groups.
Findings
The effect of vacuum level significantly affected peak hip external rotation and external knee adduction moment. Maximum braking and propulsive ground reaction forces generally increased for the residual limb and decreased for the intact limb with increasing vacuum. Additionally, the intact limb experienced an increased loading due to gait asymmetry for several variables.
Interpretation
There was no systematic vacuum level effect on gait. Higher vacuum levels, such as 15 and 20 inHg, were more comfortable and provided some relief to the intact limb, but may also increase the risk of osteoarthritis of the residual limb due to the increased peak external hip and knee adduction moments. Very low vacuum should be avoided because of the negative effects on gait symmetry. A moderate vacuum level at 15 inHg is suggested for unilateral transtibial amputees with elevated vacuum suspension.
Keywords: amputees, prosthesis, vacuum level, biomechanics, gait, comfort
Introduction
There are an estimated 1.5 million people with amputations living in the United States [1]. Of these, approximately 400,000 have unilateral lower-limb amputations who are at a substantially higher risk to develop osteoarthritis (OA) in the hip and knee of the intact limb than in the able-bodied population [2–4]. Previous studies have shown that improper prosthetic fit and alignment were associated with secondary physical conditions, including knee OA in the intact limb, osteoporosis in the amputated limb and back pain [2,4,5]. Additionally, gait asymmetries are common in persons with unilateral amputations, which is often demonstrated by a relatively longer stance time, a greater peak adduction moment for the hip and knee, and a larger first peak of vertical ground reaction force (GRF) on the intact limb [4–7]. A well-fitting prosthesis provides more comfortable control of the residual limb. This suggested a benefit from improved prosthesis design that includes socket comfort and could also reduce the loading burden of the intact limb and the risk of degenerative joint OA [6, 8].
The elevated vacuum suspension system (EVSS) has been cited as providing a better fitting socket and a superior prosthetic linkage compared to other suspension systems [9–12]. This system creates a strong coupling between the residual limb and prosthesis by drawing out air between the socket and liner. Previous studies have reported that the EVSS could effectively reduce vertical pistoning in the socket [9, 10], increase the rotational stability of residual limb [13] and prevent volume loss and even promote slight volume gain of the residual limb [11, 12]. In addition to a stable socket volume, the EVSS showed a lower positive pressure impulse during stance and greater negative pressure impulse during swing duration compared with the pin suspension and suction suspension system [14, 15]. This is important to amputees since positive pressure rather than negative pressure causes skin irritation and breakdown. Additionally, gait symmetry was found to improve at high vacuum conditions in contrast to no vacuum for step length and stance duration [9]. All of these effects of EVSS positively affect limb function and benefit the wearer with improved mobility and quality of life.
Although the number of amputees using the EVSS is growing quickly, a paucity of research has focused on the effect of different vacuum pressure settings including what should be considered a sufficient or preferred vacuum level. Questions about performance changes with vacuum level differences remain unanswered. One previous study investigated the effect of two intermediate vacuum levels (10 and 15 inHg) and a suction condition on the residual limb volume with a single K2 transtibial amputee [16]. A significantly lower volume fluctuation with vacuum than suction condition was found and the two tested vacuum levels had similar absolute percent changes in volume. Another study evaluated the amputees’ outcome from 8 to 20 inHg using amputee feedback and vacuum pressure data [17]. The results suggested that most amputees preferred vacuum setting greater than 14 inHg and vacuum pressure fluctuations decreased with an increase vacuum setting.
So far, the effects of EVSS on gait parameters at different vacuum levels have not been well quantified. What has been published only discusses two temporal gait parameters at one elevated vacuum [9]. Therefore, the purpose of this research was to address this gap and reveal the effect of vacuum levels on gait characteristics for unilateral transtibial amputees (TTA), including temporal parameters, kinematics and kinetics. The knowledge gained may benefit amputees, clinicians and prosthetic designers to better understand the effect of vacuum level on amputee gait.
Methods
Subjects
Eighteen adult male subjects participated in this study. Nine unilateral TTA currently using the EVSS comprised the sample of interest, with a mean (SD) age of 51.1 (16.1) years, height of 183.3 (6.0) cm, body mass of 94.8 (12.1) kg, and BMI of 28.3 (4.0) kg/m2. These amputees were recruited from regional prosthetic clinics and were free from musculoskeletal disorders and leg pain, and did not require assistive devices for walking. Of these unilateral TTA, five amputations occurred due to trauma, one was vascular, and three resulted from other causes. All amputees had dynamic response prosthetic feet and mechanical vacuum pumps. Self-assessed K-activity levels were used to describe the activity and capability of the amputee. K1 is classified as the most limited category and K4 the most active [18]. Seven unilateral TTA were K3 and two were K4 in this assessment, implying that all of the TTA in this study were capable of ambulating with variable cadence. The nine adult male control subjects were recruited from University of Utah and had a mean (SD) age of 27.8 (3.7) years, height of 180.1 (5.3) cm, body mass of 82.9 (17.7) kg, and BMI of 25.5 (4.8) kg/m2. Each control subject was free from limb injuries or other disorders which would affect their gait. Institutional review board approval was obtained and all participants signed an informed consent document before participating in the study.
Procedures
Prior to the gait analysis, the Trinity Amputation and Prosthesis Experience Scales (TAPES) questionnaire was completed by amputees to assess various aspects of having an artificial limb including psychosocial adjustment issues, activity restriction and prosthesis satisfaction [19]. The portion of TAPES regarding activity restriction was also completed by the control group.
For the gait data collection, 14 mm reflective markers were attached bilaterally to the participants using a standard lower extremity and trunk modeling protocol common for clinical gait assessment [20]. A static trial was performed for each subject to calibrate the marker set for that individual. A knee alignment device was placed on the knee in the static trial to assist in defining the frontal plane of the thigh segment. Subjects wore shoes during trials. For amputees, ankle markers on the prosthetic side were placed over the center of rotation of the prosthetic ankle joint and the markers on the prosthetic shank were placed to approximate the same location as the intact limb. All markers were placed by the same researcher to limit marker placement variability. Amputees wore their own personal socket and prosthesis during both static and dynamic trials. Three-dimensional motion data were captured with a ten-camera motion capture system (Vicon Motion Systems Ltd, Oxford, UK) at 100 Hz and GRFs were measured using four force plates (Advanced Mechanical Technology, Inc. Watertown, USA) at 1000 Hz.
A pressure measurement system (Fig. 1) was developed to measure vacuum pressure inside the socket. The gauge has a scale ranging from 0 to 30 inHg with increments of 1 inHg (Item no. VG150-18PBM, Anver Corporation, Hudson, USA). The gauge has an accuracy of 0.75 inches Hg, according to the manufacturer. One length of hose (Tygon R-3603, Saint Gobain Performance Plastics, Akron, USA) connects the gauge to a brass tee having three barbs. Stemming from one side of the tee is another length of hose leading to a one-way check valve. One side of the one-way valve was connected to the vacuum socket of the prosthetic limb via a hose which is part of the prosthetic limb. As a result, pressure in the socket was directly measurable. A hand-held vacuum pump (Model MV8500, MityVac Corporation, St. Louis, USA) was connected to the third barb of the brass tee for pulling elevated vacuum levels in the vacuum socket.
Fig. 1.
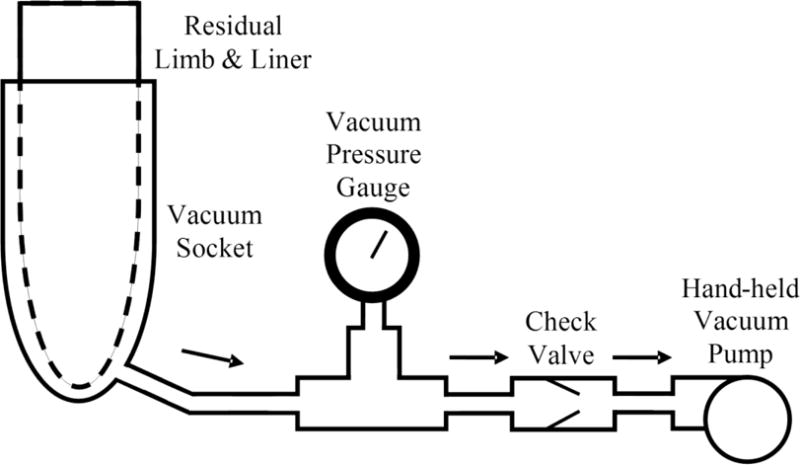
Diagram of vacuum pressure measurement system
Vacuum levels of 0, 5, 10, 15, and 20 inHg were assigned in random order to unilateral TTA in a static standing position. Five trials with clean force plate strikes were collected for each limb at each vacuum level. Vacuum was monitored for every trial with the gauge attached to the prosthesis. If vacuum changed by more than 2 inHg from the target value, the pump was reconnected and vacuum was pulled to the target level before continuing with more trials. After each set of trials, amputees were questioned to assess the prosthesis comfort level based on a scale from 1–10, with 10 being the highest level of comfort. Walking speed for amputees was controlled to be within the range of 1.20 to 1.40 m/s with a target of 1.30 m/s, which was similar to the adult preferred walking speed published in the literature [21, 22]. This process was achieved by the instructions from a custom walking speed timing system described elsewhere [23]. Control subjects walked at their typical walking speed for five successful trials with each limb.
Data analysis
The variables of interest were temporal, kinematic and kinetic parameters. The temporal variables included speed, cadence, step length, step time, stance phase, single and double supports. Kinematic variables included the range of motion (RoM) between the hip and knee in three body planes and ankle in the sagittal plane. Additionally, the peak value of hip extension and ankle dorsiflexion during stance phase, and also peak value of knee flexion, ankle plantarflexion, hip abduction and external rotation during swing phase. Kinetic variables included the peak value of hip and knee adduction moments, and also GRF in the vertical and anteroposterior directions.
The experimental data were firstly processed using Vicon Nexus software (Vicon Motion Systems Ltd, Oxford, UK). Marker trajectories and analog data were filtered, prior to running plug-in gait model, with a cut-off frequency of 6 Hz and 300 Hz respectively. The model parameters for residual limb were considered to be the same as for the intact limb. The kinematic and kinetic data were filtered using a fourth order zerolag Butterworth filter with a cut-off frequency of 6 Hz. Then, Visual 3D software (C-Motion; Germantown, USA) was used to calculate the temporal variables and determine the peak value and RoM of kinematic and kinetic variables. All the variables were normalized to 101 points for each gait cycle. Kinetic and GRF were finally normalized to body weight and mass of each subject, respectively. For the amputees, all the temporal, kinematic and kinetic quantities were averaged across trials for each amputee at each vacuum level, then averaged across amputees for both intact and residual limbs. For the control group, the variables were firstly averaged across five within-subject trials and then across subjects to obtain group-averaged data.
Statistical analysis
Statistics were performed using SPSS 20.0 (IBM Corporation, Armonk, USA). Descriptive statistics were calculated for sample and gait variables. Dunnett’s t-test was used to compare the limb effect (residual with control, intact with control) at each vacuum level with the control group. Two-factor (vacuum level and limb), repeated measures analysis of variance (RANOVA) was used to determine the effects of vacuum level and limb within the amputee group. If the assumption of sphericity was violated, the Greenhouse-Geisser correction was used. Post-hoc tests were performed using the Bonferroni adjustment to correct for multiple comparisons. A significance level of 0.05 was used for all statistical comparisons.
Results
Although the amputee group was older than the control group (P = 0.010), they were not significantly different in height, body mass and BMI. In terms of activity restriction, amputee group showed similar activity and functional abilities with control group as assessed by TAPES. The self-assessed comfort levels were statistically different by vacuum level (P = 0.001). Averaged comfort levels were 7.6, 8.3, 8.9 and 8.6 at the 5, 10, 15, and 20 inHg vacuum levels, respectively, and other than the 5 inHg were all significantly higher than the mean of 5.6 for no vacuum (0 inHg).
Temporal Parameters
The vacuum level had no statistically significant effect on temporal parameters, but a significant limb effect was found for the step length (P = 0.005), limb speed (P = 0.023), stance phase (P = 0.019) and single support (P = 0.008) (Table 1). Furthermore, the step time showed a significant limb by vacuum level interaction effect (P = 0.034), with the residual limb step time longer than intact limb for all vacuum levels except for 0 inHg.
Table 1.
Mean (SD) temporal parameters for amputee group and controls
| Vacuum Level | 0 in Hg | 5 in Hg | 10 in Hg | 15 in Hg | 20 in Hg | Control | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intact | Residual | Intact | Residual | Intact | Residual | Intact | Residual | Intact | Residual | ||
| Step length (m) * | 0.792 (0.05)‡ |
0.723 (0.04) |
0.791 (0.04)‡ |
0.718 (0.04) |
0.783 (0.04)‡ |
0.718 (0.03) |
0.781 (0.05)‡ |
0.720 (0.03) |
0.797 (0.05)‡ |
0.723 (0.04) |
0.721 (0.06) |
| Limb speed (m/s) * | 1.41 (0.08) |
1.27 (0.06) |
1.42 (0.09) |
1.27 (0.08) |
1.40 (0.10) |
1.25 (0.07) |
1.40 (0.10) |
1.26 (0.07) |
1.44 (0.10) |
1.27 (0.07) |
1.26 (0.17) |
| Step time (s) | 0.564 (0.03) |
0.565 (0.03) |
0.550 (0.03) |
0.567 (0.04) |
0.560 (0.03) |
0.574 (0.04) |
0.558 (0.03) |
0.573 (0.04) |
0.554 (0.03) |
0.570 (0.03) |
0.571 (0.03) |
| Cadence (step/s) | 0.891 (0.04) |
0.890 (0.05) |
0.897 (0.05) |
0.886 (0.05) |
0.894 (0.05) |
0.885 (0.05) |
0.894 (0.05) |
0.885 (0.05) |
0.894 (0.05) |
0.886 (0.04) |
0.873 (0.05) |
| Stance phase (% cycle)* | 64.8 (1.5) |
63.0 (1.5) |
65.1 (1.5)‡ |
63.0 (1.5) |
64.9 (1.3) |
63.2 (1.3) |
64.9 (1.5) |
62.8 (16) |
64.8 (1.3) |
62.7 (16) |
63.1 (2.0) |
| Single support (% cycle)* | 36.8 (18) |
34.5 (1.7)† |
37.3 (1.7) |
34.8 (1.6)† |
36.7 (16) |
35.0 (1.4)† |
37.1 (18) |
34.6 (2.1)† |
37.1 (1.7) |
34.5 (1.5)† |
37.2 (2.1) |
| Double support (% cycle) | 28.0 (2.7) |
28.5 (2.3) |
27.7 (2.0) |
28.2 (2.2) |
28.2 (2.4) |
28.2 (2.3) |
27.9 (2.7) |
28.3 (2.4) |
27.7 (2.2) |
28.2 (2.6) |
25.9 (3.8) |
Significant limb effect in amputee group (P < 0.05)
Significant difference between the residual limb and controls (P < 0.05)
Significant difference between the intact limb and controls (P < 0.05)
In all five vacuum level conditions, amputees displayed a shorter single support for the residual limb and a longer step length for the intact limb when compared with the control group (Table 1). Additionally, the stance phase was longer (P = 0.037) for the intact limb at 5 inHg than the controls. But the step time, cadence and double support were comparable among intact, residual and control limbs at all vacuum levels.
Gait Kinematics
A significant effect of vacuum level was found for the peak hip external rotation during swing phase (P = 0.023) (Table 2, Fig. 2). Post-hoc tests revealed that peak hip external rotation during swing phase was smaller for vacuum level at 10 inHg (= 0.020) and 15 inHg (P = 0.025) compared with no vacuum (0 inHg). In addition, the limb effect was significant for ankle RoM (P = 0.021) and ankle plantarflexion during swing phase (P = 0.019) for amputees (Table 2, Fig. 2).
Table 2.
Mean (SD) peak kinematic values and joint RoM in degree
| Vacuum Level | 0 in Hg | 5 in Hg | 10 in Hg | 15 in Hg | 20 in Hg | Control | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Intact | Residual | Intact | Residual | Intact | Residual | Intact | Residual | Intact | Residual | |||
| Hip stance | extension | 12.3 (4.9) |
8.1 (6.5) | 12.3 (6.5) |
9.6 (8.1) | 12.3 (6.4) |
8.9 (7.2) | 11.8 (7.1) |
9.0 (7.1) | 12.2 (6.8) |
9.0 (7.2) | 10.3 (4.0) |
| Hip swing | abduction | 9.1 (4.9) |
11.8 (6.3) |
8.7 (4.9) |
12.0 (6.3) |
10.5 (5.8) |
11.7 (6.2) |
9.0 (5.1) |
11.8 (6.0) |
8.6 (5.4) |
11.6 (5.9) |
11.4 (2.8) |
| Hip rotation swing †† | external | −3.3 (4.7) |
8.5 (12.9)† |
−3.1 (4.6) |
5.9 (11.3)† |
−3.6 (4.7) |
5.6 (11.5)† |
−2.9 (4.8) |
4.3 (11.1)† |
−2.9 (3.8) |
7.2 (13.6)† |
−0.6 (6.9) |
| Hip (sagittal) | RoM | 52.4 (4.2)‡ |
53.6 (5.9)† |
54.1 (3.9)‡ |
53.6 (7.2)† |
53.3 (3.1)‡ |
53.2 (5.7)† |
52.0 (3.8)‡ |
53.3 (5.5)† |
52.8 (3.9)‡ |
53.3 (5.6)† |
47.2 (4.2) |
| Hip (frontal) | RoM | 14.9 (7.8) |
15.3 (5.3) |
16.7 (5.9) |
17.3 (7.0) |
19.1 (7.3) |
15.8 (5.4) |
17.1 (5.5) |
15.3 (5.1) |
16.7 (5.0) |
14.8 (5.2) |
17.0 (3.2) |
| Hip (horizontal) | RoM | 17.2 (3.2)‡ |
27.0 (20.0)† |
18.4 (5.0)‡ |
22.4 (18.9)† |
17.1 (3.9)‡ |
22.5 (18.6)† |
17.1 (3.2)‡ |
21.4 (19.4)† |
17.3 (3.2)‡ |
24.1 (20.5)† |
13.4 (3.1) |
| Knee swing | flexion | 64.0 (3.8) |
68.0 (5.0) |
63.8 (3.1) |
67.2 (4.0) |
63.3 (3.3) |
66.5 (4.4) |
64.2 (3.6) |
66.5 (4.5) |
63.4 (3.6) |
66.3 (5.0) |
62.2 (5.8) |
| Knee (sagittal) | RoM | 65.9 (5.7) |
73.5 (7.6)† |
65.8 (4.4) |
73.6 (7.8)† |
66.1 (4.5) |
72.1 (8.0)† |
66.4 (5.8) |
72.2 (9.0)† |
65.9 (4.4) |
72.2 (9.3)† |
64.0 (3.8) |
| Knee (frontal) | RoM | 10.3 (3.8) |
18.0 (13.0)† |
10.7 (4.3) |
15.2 (10.2)† |
10.8 (5.2) |
15.7 (9.9)† |
10.0 (6.4) |
15.3 (9.1)† |
10.4 (4.4) |
15.4 (9.6)† |
8.9 (3.9) |
| Knee (horizontal) | RoM | 18.6 (3.4) |
10.9 (4.7)† |
17.4 (2.3) |
11.4 (3.7)† |
17.7 (2.4) |
10.3 (4.6)† |
18.1 (3.0) |
10.9 (5.8)† |
18.3 (2.6) |
9.2 (3.1)† |
16.7 (3.4) |
| Ankle dorsiflexion stance | 16.1 (19) |
17.7 (3.3)† |
15.2 (2.5) |
17.4 (3.3)† |
15.3 (2.0) |
17.6 (3.5)† |
16.1 (2.0) |
17.5 (3.7)† |
15.1 (3.0) |
17.5 (3.7)† |
15.5 (18) |
|
| Ankle plantarflexion swing* | 15.9 (6.2) |
−4.2 (4.6)† |
16.5 (6.9) |
−4.8 (5.1)† |
16.3 (6.6) |
−4.5 (5.0)† |
16.0 (5.2) |
−4.5 (5.1)† |
16.9 (6.9) |
−5.3 (4.5)† |
13.8 (8.2) |
|
| Ankle (sagittal)* | RoM | 32.0 (6.3) |
21.9 (4.5)† |
31.8 (6.2) |
22.2 (5.0)† |
31.6 (6.0) |
22.1 (4.6)† |
32.0 (4.5) |
21.9 (5.3)† |
32.0 (6.3) |
22.8 (5.1)† |
29.3 (3.9) |
Significant limb effect in amputee group (P < 0.05)
Significant vacuum level effect in amputee group (P < 0.05)
Significant difference between the residual limb and controls (P < 0.05)
Significant difference between the intact limb and controls (P < 0.05)
Fig. 2.
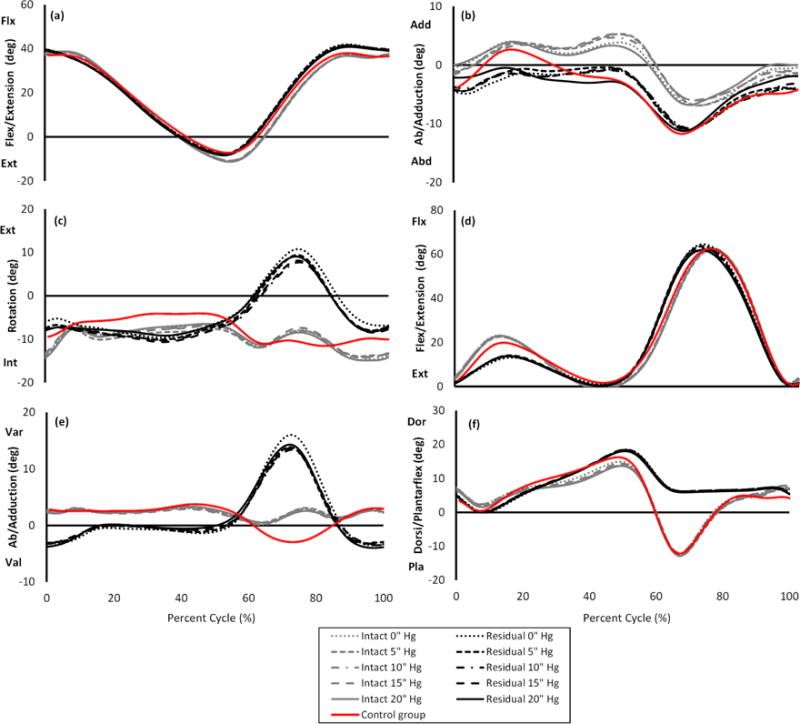
Lower limb joint kinematics by vacuum level and limb. (a) Hip flexion/extension (b) Hip adduction/abduction (c) Hip external/internal rotation (d) Knee flexion/extension (e) Knee varus/valgus (f) Ankle dorsiflexion/plantarflexion
In all five vacuum level conditions, significant differences were found for hip sagittal and horizontal RoMs between the amputees (both intact and residual limbs) and controls. The residual limb also displayed a larger hip external rotation during swing phase, ankle dorsiflexion during stance phase and knee sagittal RoM, but a smaller knee horizontal RoM and ankle sagittal RoM when compared with controls (Table 2).
Gait Kinetics
The effect of vacuum level was significant for the peak external knee adduction moment (KAM) (P = 0.009), which was larger for vacuum level at 5 inHg (P = 0.005) and 20 inHg (P = 0.039) compared with no vacuum (Table 3). There were several statistically significant differences between the intact and residual limbs (Table 3, Fig. 3), including peak external hip adduction moment (HAM) (= 0.004), second peak vertical GRF (P = 0.007) and maximum propulsive GRF (P = 0.001). Additionally, first peak vertical GRF (P = 0.035), maximum braking (P = 0.020) and propulsive GRF (P = 0.019) were found to have significant limb by vacuum level interaction effect within the amputee group.
Table 3.
Mean (SD) peak kinetic values and GRF
| Vacuum Level | 0 in Hg | 5 in Hg | 10 in Hg | 15 in Hg | 20 in Hg | Control | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Intact | Residual | Intact | Residual | Intact | Residual | Intact | Residual | Intact | Residual | ||
| External HAM (Nm/kg) * | 0.846 (0.04) |
0.546 (0.17) |
0.849 (0.04) |
0.585 (0.17) |
0.844 (0.05) |
0.554 (0.18) |
0.852 (0.06) |
0.574 (0.17) |
0.863 (0.05) |
0.592 (0.17) |
0.698 (0.16) |
| External KAM (Nm/kg)†† | 0.526 (0.20) |
0.340 (0.16) |
0.535 (0.21) |
0.386 (0.19) |
0.524 (0.20) |
0.359 (0.18) |
0.538 (0.19) |
0.374 (0.19) |
0.553 (0.20) |
0.396 (0.20) |
0.581 (0.18) |
| First vertical GRF (%BW) | 1.14 (0.09) |
1.05 (0.06) |
1.12 (0.08) |
1.06 (0.08) |
1.13 (0.07) |
1.05 (0.06) |
1.12 (0.08) |
1.04 (0.07) |
1.13 (0.07) |
1.06 (0.08) |
1.08 (0.09) |
| Second Vertical GRF (%BW) * | 1.13 (0.09) |
0.98 (0.06)† |
1.13 (0.09) |
0.99 (0.07)† |
1.13 (0.08) |
0.99 (0.07)† |
1.13 (0.08) |
0.99 (0.07)† |
1.14 (0.08) |
0.99 (0.07)† |
1.08 (0.08) |
| Posterior braking GRF (%BW) | 0.194 (0.03) |
0.148 (0.02) |
0.184 (0.02) |
0.157 (0.02) |
0.185 (0.02) |
0.158 (0.03) |
0.178 (0.03) |
0.162 (0.03) |
0.176 (0.02) |
0.163 (0.03) |
0.192 (0.03) |
| Anterior propulsion GRF (%BW) * | 0.224 (0.03) |
0.137 (0.02)† |
0.220 (0.03) |
0.140 (0.02)† |
0.218 (0.03) |
0.142 (0.02)† |
0.214 (0.03) |
0.142 (0.02)† |
0.215 (0.03) |
0.144 (0.02)† |
0.204 (0.03) |
Significant limb effect in amputee group (P < 0.05)
Significant vacuum level effect in amputee group (P < 0.05)
Significant difference between the residual limb and controls (P < 0.05)
Fig. 3.
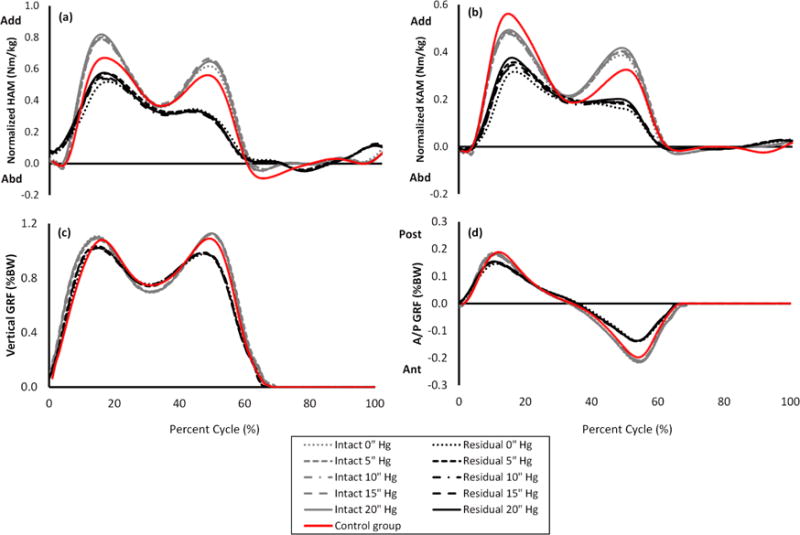
Joint kinematics and GRF by vacuum level and limb. (a) External hip adduction/abduction moment (b) External Knee adduction/abduction moment (c) Vertical GRF (d) anterior/posterior GRF
When compared with the controls, amputees showed a significantly smaller second vertical force and propulsive force on the residual limb at all vacuum levels (Table 3). No significant differences were found for the peak of first vertical GRF, braking force, external HAM and KAM between the controls and amputees (both intact and residual limbs) at any vacuum levels (Table 3).
Discussion
The purpose of this study was to investigate the effects of EVSS on gait parameters at different vacuum levels. Comfort in the EVSS generally increased with an elevated vacuum, indicating a preference for higher levels of vacuum, and notably the mean comfort value was greatest at 15 inHg. These findings support reported results that over 70% of amputees have self-preferred vacuum levels of 14 inHg or greater [17].
The limb effect was a significant factor for many temporal parameters, rather than different vacuum levels. This was confirmed by the longer step length, greater stance phase and shorter single support duration for the intact limb than residual limb. These results suggest that the amputees rely on intact limb to a greater extent than residual limb to move forward, which aligned well with previous research relative to amputee gait [5, 7, 24]. The intact limb showed a faster limb speed than residual limb, based on step length and step time, which had implications for kinetics and GRF. Amputees displayed shorter single support duration for the residual limb than controls, which suggests that amputee gait is less stable than able-bodied gait.
Step time was found to have a significant interaction effect. The residual limb showed the same longer step time (about 0.015s) than the intact limb with vacuum (5–20 inHg), but similar step time was observed for both limbs without vacuum. These results indicated that amputees spent a greater proportion of time on the residual limb compared to the intact limb at vacuum conditions [9], which was also in agreement with the significantly higher comfort levels with vacuum than without vacuum.
The effect of vacuum level significantly influenced peak hip external rotation during swing phase, and the value at 15 inHg was smaller than no vacuum and was most comparable to the control group. This finding agreed with the self-reported comfort level results and the typical daily vacuum level setting with a mean (SD) 16 (2) inHg [17]. Further analysis showed that the difference between without vacuum and 15 inHg was mainly due to the residual limb (4.3 and 8.5 degree, Table 2) and the change was nearly 20% since the average hip rotation RoM was 21.4 degree at 15 inHg for residual limb.
The peak hip extension in stance phase was about three degrees higher, on average, for the intact limb than the residual limb and controls. This at least partially contributes to greater step length observed for the intact limb. The peak knee flexion during swing phase in the residual limb trended toward smaller for higher vacuum level (Table 2, knee flexion swing), which was likely due to the effect of increased pistoning at lower vacuum levels [9, 16], where slightly more knee flexion would be required to produce the same amount of toe clearance during swing compared with higher vacuum levels. Additionally, the minimum difference of peak knee flexion between the intact and residual limbs was found at 15 inHg, which suggests that reduced pistoning in the socket may improve the gait symmetry [9].
Not surprisingly, the passive prosthetic foot did not generate plantarflexion at the end of the stance phase, while the intact limb did. This explains the findings that peak ankle plantarflexion and ankle RoM were significantly different between intact and residual limbs. The ankle kinematics have clinically significant asymmetry between limbs and lack of residual limb plantarflexion affects ipsilateral ankle joint power production and induces compensation mechanisms [5]. This may partly contribute to the significant difference of hip and knee RoMs of the residual limb when compared with controls. Somewhat surprisingly, hip and knee RoMs were comparable between intact and residual limbs for the amputees with EVSS at all the vacuum levels, which contrasts with previous reports that hip and knee sagittal RoMs were significantly different between limbs for unilateral TTA [7]. These results indicate that the EVSS has the ability to provide a well-fitting socket and partially compensates for asymmetry during gait.
The effect of vacuum level was significant for peak external KAM and a higher value was found at 20 inHg than with no vacuum. Additionally, peak external HAM and KAM tended to increase with increasing vacuum level from 10 inHg to 20 inHg for both the intact and residual limbs although there was not statistically different (Table 3). These findings suggest that it may not be recommended to use higher vacuum levels for the EVSS if a lower level of vacuum will suffice. Additional research is needed to confirm these results and verify that a higher adduction moment occurs with increased vacuum. An increase in adduction moment has been thought to increase the rate of OA progression, especially in the knee joint and should be avoided [6, 25, 26].
Although vacuum level significantly contributes to the external KAM value, the vacuum level alone cannot completely mitigate the between-limb effect. In the current study, intact limb showed a 50% and 44% greater peak external HAM and KAM than the residual limb, respectively, which indicated probability of higher joint OA incidence in the intact limb than residual limb of amputees [2, 6, 25].
The residual limb had a diminished second peak of vertical GRF and peak propulsive GRF compared to intact limb. This is likely due to the lower limb speeds and the compliance of the prosthesis, including the displacement of the mechanical pump and decreased vertical deceleration of the residual limb. Additionally, lack of plantar flexors and limited energy storage capacity of the prosthesis also contributed to the smaller propulsive force peak for the residual limb, as was expected.
The peak braking and propulsive GRFs were significantly affected by the limb by vacuum level interaction effects, which generally increased for the residual limb and decreased for the intact limb with increasing vacuum. This result suggests that amputees had less dependence on intact limb at higher vacuum levels. Additionally, the largest differences between limbs happened at 0 inHg which implies more gait asymmetry. This, in addition to the adverse effects on comfort, make it inadvisable to operate the EVSS without vacuum.
Some limitations existed in the current study. The unilateral TTA group was older than the control group. Several studies showed that the gait characteristics changed with age, which was most explained by a reduced walking speed [27, 28]. Since walking speed was controlled across groups, age is unlikely to be a main contributor to the findings between amputee and control groups. The current gait model assumed the prosthetic limb had the same value as for the intact limb. However, prosthetic and intact limb mass differences exist, as well as disparities in the center of mass and moments of inertia, which may result in miscalculation of the hip and knee joint moment. Previous research suggested that mass differences have a greater effect on kinetics during swing phase than stance phase for amputees [29] and no significant difference between peak hip and knee moment calculation between direct measurement and cadaver-estimated anthropometry during prosthetic gait [30]. Since this study examined the peak external HAM and KAM in early stance, we believe that the model provides reasonable estimates of these values. Finally, all the pumps were mechanical which likely reduces the influence of pump effects, but it may also prevent the ability to generalize the findings to other pump types. Future studies focused on the combined effects of pump design and vacuum levels is needed to extend the current findings.
Conclusions
In summary, the gait characteristics of unilateral TTA using EVSS at multiple vacuum levels were studied. It was found that vacuum level had a significant effect on the comfort level, peak hip external rotation and maximum external KAM. Vacuum level by limb interaction effect was significant for maximum braking and propulsive ground reaction forces, which generally increased for the residual limb and decreased for the intact limb with increasing vacuum. These result indicate that amputees had less dependence on their intact limb at higher vacuum levels, which generally led to greater comfort. Additionally, the intact limb of the amputee showed a greater burden than the residual limbs for many parameters including step length, stance phase, single support duration, peak ankle plantarflexion, ankle sagittal ROM, maximum external HAM, maximum propulsive and second vertical GRFs. Many of these differences could be thought of as compensation mechanisms, some of which resulted from the different speed among limbs and the lack of plantar flexors in the prosthesis.
While the current study does not reveal a specific ideal vacuum level for all gait variables, there are trade-offs associated with increasing the vacuum level. Higher vacuum levels, such as 15 and 20 inHg, have been shown to be more comfortable and provide some relief to the burden of the intact limb, but also increase the risk of OA due to a greater peak external HAM and KAM for the residual limb. Very low levels of vacuum should be avoided because they exacerbate gait asymmetry on GRFs. Therefore, several factors should be taken into account when recommending a vacuum level including limb comfort, patient preference and also gait characteristics. We suggest that a moderate vacuum level at 15 inHg is a good choice and should be considered in the design and fitting of EVSS for unilateral TTA.
Highlights.
Comfort level improved with increasing vacuum and provided relief to the intact limb
Vacuum effect was significant on peak hip external rotation and knee adduction moment
The intact limb showed an increased loading than residual limb due to gait asymmetry
Very low vacuum should be avoided because of the negative effects on gait symmetry
Vacuum level at 15 inHg is suggested for amputees with elevated vacuum suspension
Acknowledgments
This work was supported by National Natural Science Foundation of China (81601635), Natural Science Foundation of JiangSu (BK20150223), University Science Research Project of Jiangsu Province (14KJB310022), Scientific Research Foundation for Excellent Talents of Xuzhou Medical College (D2014018) and NIOSH Education and Research Center training grant T42/CCT810426-10.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.McGimpsey G, Bradford TC. Limb prosthetics services and devices. Bioengineering Institute Center for Neuroprosthetics Worcester Polytechnic Institution. 2008 [Google Scholar]
- 2.Struyf PA, van Heugten CM, Hitters MW, Smeets RJ. The prevalence of osteoarthritis of the intact hip and knee among traumatic leg amputees. Archives of physical medicine and rehabilitation. 2009;90:440–446. doi: 10.1016/j.apmr.2008.08.220. [DOI] [PubMed] [Google Scholar]
- 3.Lemaire ED, Fisher FR. Osteoarthritis and elderly amputee gait. Archives of physical medicine and rehabilitation. 1994;75:1094–1099. doi: 10.1016/0003-9993(94)90084-1. [DOI] [PubMed] [Google Scholar]
- 4.Gailey R, Allen K, Castles J, Kucharik J, Roeder M. Review of secondary physical conditions associated with lower-limb amputation and long-term prosthesis use. Journal of rehabilitation research and development. 2008;45:15–29. doi: 10.1682/jrrd.2006.11.0147. [DOI] [PubMed] [Google Scholar]
- 5.Sagawa Y, Turcot K, Armand S, Thevenon A, Vuillerme N, Watelain E. Biomechanics and physiological parameters during gait in lower-limb amputees: a systematic review. Gait & posture. 2011;33:511–526. doi: 10.1016/j.gaitpost.2011.02.003. [DOI] [PubMed] [Google Scholar]
- 6.Royer TD, Wasilewski CA. Hip and knee frontal plane moments in persons with unilateral, trans-tibial amputation. Gait & posture. 2006;23:303–306. doi: 10.1016/j.gaitpost.2005.04.003. [DOI] [PubMed] [Google Scholar]
- 7.Bateni H, Olney SJ. Kinematic and kinetic variations of below-knee amputee gait. JPO: Journal of Prosthetics and Orthotics. 2002;14:2–10. [Google Scholar]
- 8.Nolan L, Lees A. The functional demands on the intact limb during walking for active transfemoral and trans-tibial amputees. Prosthetics and orthotics international. 2000;24:117–125. doi: 10.1080/03093640008726534. [DOI] [PubMed] [Google Scholar]
- 9.Board W, Street G, Caspers C. A comparison of trans-tibial amputee suction and vacuum socket conditions. Prosthetics and orthotics international. 2001;25:202–209. doi: 10.1080/03093640108726603. [DOI] [PubMed] [Google Scholar]
- 10.Klute GK, Berge JS, Biggs W, Pongnumkul S, Popovic Z, Curless B. Vacuum-assisted socket suspension compared with pin suspension for lower extremity amputees: effect on fit, activity, and limb volume. Archives of physical medicine and rehabilitation. 2011;92:1570–1575. doi: 10.1016/j.apmr.2011.05.019. [DOI] [PubMed] [Google Scholar]
- 11.Goswami J, Lynn R, Street G, Harlander M. Walking in a vacuum-assisted socket shifts the stump fluid balance. Prosthetics and orthotics international. 2003;27:107–113. doi: 10.1080/03093640308726666. [DOI] [PubMed] [Google Scholar]
- 12.Street G. Vacuum suspension and its effects on the limb. Orthopadie Technik. 2006;4:1–7. [Google Scholar]
- 13.Papaioannou G, Mitrogiannis C, Nianios G, Fiedler G. Assessment of vacuum-assisted trans-tibial amputee socket dynamics. 9th International Conference on Information Technology and Applications in Biomedicine. 2009:1–4. [Google Scholar]
- 14.Beil TL, Street GM. Comparison of interface pressures with pin and suction suspension systems. Journal of rehabilitation research and development. 2004;41:821–828. doi: 10.1682/jrrd.2003.09.0146. [DOI] [PubMed] [Google Scholar]
- 15.Beil TL, Street GM, Covey SJ. Interface pressures during ambulation using suction and vacuum-assisted prosthetic sockets. Journal of rehabilitation research and development. 2002;39:693–700. [PubMed] [Google Scholar]
- 16.Gerschutz MJ, Denune JA, Colvin JM, Schober G. Elevated vacuum suspension influence on lower limb amputee’s residual limb volume at different vacuum pressure settings. JPO: Journal of Prosthetics and Orthotics. 2010;22:252–256. [Google Scholar]
- 17.Gerschutz MJ, Denune JA, Colvin JM, Schober G, Haynes ML, Nixon D. Technical notes on elevated vacuum suspension: Amputee patient outcomes evaluating patient verbal opinion and pressure data. 2011 Available: http://www.willowwoodco.com/files/products-and-services/suspension/vacuum/2170-c-technical-notes-on-elevated-vacuum-suspension-amp-patient-outcomes.pdf.
- 18.Medicare CF, Services M. Medicare region C durable medical equipment prosthetics orthotic supplier (DMEPOS) manual. Washington (DC): US Department of Health and Human Services; 2005. [Google Scholar]
- 19.Gallagher P, MacLachlan M. The Trinity Amputation and Prosthesis Experience Scales and quality of life in people with lower-limb amputation. Archives of physical medicine and rehabilitation. 2004;85:730–736. doi: 10.1016/j.apmr.2003.07.009. [DOI] [PubMed] [Google Scholar]
- 20.Davis RB, Ounpuu S, Tyburski D, Gage JR. A gait analysis data collection and reduction technique. Human movement science. 1991;10:575–587. [Google Scholar]
- 21.Kirtley C, Whittle MW, Jefferson R. Influence of walking speed on gait parameters. Journal of biomedical engineering. 1985;7:282–288. doi: 10.1016/0141-5425(85)90055-x. [DOI] [PubMed] [Google Scholar]
- 22.Öberg T, Karsznia A, Öberg K. Basic gait parameters: reference data for normal subjects, 10–79 years of age. Journal of rehabilitation research and development. 1993;30:210–223. [PubMed] [Google Scholar]
- 23.Greenland KO. Effects of elevated vacuum socket suspension and vacuum level on unilateral trans-tibial amputee gait. The University of Utah. 2012 [Google Scholar]
- 24.Kovač I, Medved V, Ostojić L. Spatial, temporal and kinematic characteristics of traumatic transtibial amputees’ gait. Collegium antropologicum. 2010;34:205–213. [PubMed] [Google Scholar]
- 25.Foroughi N, Smith R, Vanwanseele B. The association of external knee adduction moment with biomechanical variables in osteoarthritis: a systematic review. The Knee. 2009;16:303–309. doi: 10.1016/j.knee.2008.12.007. [DOI] [PubMed] [Google Scholar]
- 26.Tanamas S, Hanna FS, Cicuttini FM, Wluka AE, Berry P, Urquhart DM. Does knee malalignment increase the risk of development and progression of knee osteoarthritis? A systematic review. Arthritis care & research. 2009;61:459–467. doi: 10.1002/art.24336. [DOI] [PubMed] [Google Scholar]
- 27.Callisaya ML, Blizzard L, Schmidt MD, McGinley JL, Srikanth VK. Sex modifies the relationship between age and gait: a population-based study of older adults. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2008;63:165–170. doi: 10.1093/gerona/63.2.165. [DOI] [PubMed] [Google Scholar]
- 28.Laufer Y. Effect of age on characteristics of forward and backward gait at preferred and accelerated walking speed. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2005;60:627–632. doi: 10.1093/gerona/60.5.627. [DOI] [PubMed] [Google Scholar]
- 29.Miller DI. Resultant lower extremity joint moments in below-knee amputees during running stance. Journal of biomechanics. 1987;20:529–541. doi: 10.1016/0021-9290(87)90253-3. [DOI] [PubMed] [Google Scholar]
- 30.Goldberg EJ, Requejo PS, Fowler EG. The effect of direct measurement versus cadaver estimates of anthropometry in the calculation of joint moments during above-knee prosthetic gait in pediatrics. Journal of biomechanics. 2008;41:695–700. doi: 10.1016/j.jbiomech.2007.10.002. [DOI] [PubMed] [Google Scholar]