

Abstract
Background
Many transgender college students struggle with identity formation and other emotional, social, and developmental challenges associated with emerging adulthood. A potential maladaptive coping strategy employed by such students is heavy drinking. Prior literature has suggested greater consumption and negative alcohol-related consequences (ARCs) in transgender students compared with their cisgender peers, but little is known about their differing experiences with alcohol-related blackouts (ARBs). We examined the level of alcohol consumption, the frequency of ARBs and other ARCs, and motivations for drinking reported by the largest sample of transgender college students to date.
Methods
A Web survey from an alcohol-prevention program, AlcoholEdu for College™, assessed student demographics and drinking-related behaviors, experiences, and motivations of newly matriculating first-year college students. A self-reported drinking calendar was used to examine each of the following measures over the previous 14 days: number of drinking days, total number of drinks, and maximum number of drinks on any single day. A 7-point Likert scale was used to measure ARCs, ARBs, and drinking motivations. Transgender students of both sexes were compared with their cisgender peers.
Results
989 of 422,906 students (0.2%) identified as transgender. Over a 14-day period, transgender compared with cisgender students were more likely to consume alcohol over more days, more total drinks, and a greater number of maximum drinks on a single day. Transgender students (36%) were more likely to report an ARB than cisgender students (25%) as well as more negative academic, confrontation-related, social, and sexual ARCs. Transgender respondents more often cited stress reduction, social anxiety, self-esteem issues, and the inherent properties of alcohol as motivations for drinking. For nearly all measures, higher values were yielded by male-to-female than female-to-male transgender students.
Conclusions
Transgender compared with cisgender first-year students engage in higher-risk drinking patterns and experience more ARBs and other negative ARCs. Broad institutional efforts are required to address the unique circumstances of transgender men and women and to reduce negative ARCs in college students, regardless of their sex or gender identity.
Keywords: Blackouts, Transgender, Alcohol, College
INTRODUCTION
Transgender men and women are frequently stigmatized, resulting in discrimination, physical and sexual assault, emotional trauma, and exclusion from scientific research or medical care (Bith-Melander et al., 2010; Bradford et al., 2013; Coulter et al., 2014, 2015; Keuroghlian et al., 2015; Reisner et al, 2015a; Roberts and Fantz, 2014; Shirers and Jaffe, 2015; Stotzer, 2009). Such struggles were highlighted by the March 23, 2016 passage in North Carolina (NC) of Session Law 2016-3/House Bill 2 (HB2) outlawing individuals from using public bathrooms discordant with their biological sex (Kopan and Scott, 2016; Scherer, 2016). In response, the U.S. Department of Justice filed a Title VII/Title IX civil-rights law suit against the governor and State of NC, and the Obama Administration issued an executive order directing all publically funded schools to allow students restroom access in accordance with their gender identity (Graham, 2016; Grinberg, 2016; Lichtblau and Fausset, 2016; Shuster et al., 2016). HB2 remains controversial at present but illustrates the conflicts, stressors, and concerns regarding diminished safety historically experienced by the transgender community (Landers, 2015; Lichtblau and Fausset, 2016; Miller and Grollman, 2015; Reisner et al, 2015a; Roberts and Fantz, 2014).
The stressors surrounding stigma versus social acceptance are likely to affect transgender college students in particular. College students in emerging adulthood must navigate the developmental tasks of transitioning from parental dependence to becoming functional, independent adults who establish intimate relationships and sustain employment. Transgender students must additionally brave the uncertainties of identifying themselves as a minority in a heteronormative society (Cruz, 2014; Hendricks and Testa, 2012; Miller and Grollman, 2015; Toomey et al., 2012). Stigma and its associated psychological consequences may complicate these developmental and individuation tasks, fostering maladaptive coping mechanisms. Furthermore, secondary schools often constitute milieus where transphobia, harassment, and bullying have previously transpired (Bradford et al. 2013; Snapp et al., 2016; Toomey et al., 2012), curtailing fundamental enthusiasm for college matriculation (Case and Meier, 2014). Many colleges are ill-equipped to accommodate the needs of this newly visible cohort (Rankin and Beemyn, 2012).
A maladaptive coping mechanism potentially employed by many transgender students in response to such challenges is excessive alcohol consumption (Coulter et al., 2015; Miller and Grollman, 2015). Proposed dynamics fueling hazardous drinking include self-medication and restriction to venues that often incorporate alcohol, such as bar settings, to gain social affirmation and communal support (Cochran and Cauce, 2006; Peacock et al., 2015; Rowe et al., 2015). The college milieu in particular is notable for pervasive alcohol consumption (Perkins, 2002; White et al., 2003, 2006), which can increase perceived normative pressures to drink (DeJong et al., 2006). For first-year students, an additional challenge lies in winning peer approval within a novel environment, which could exacerbate the struggles of transgender students who may be grappling with their identities.
Heavy drinking can result in alcohol-related blackouts (ARBs) and other adverse alcohol-related consequences (ARCs), such as physical-health problems (e.g., liver damage), riskier sexual practices that can lead to sexually transmitted infections, assault victimization, and unintentional injuries (Cooper, 2002; Hingson et al., 2016; Rehm et al., 2003). Additionally, mental-health consequences can include anxiety, depression, self-harm, and long-term neurocognitive impairment (Brown et al., 2009; Lamis et al., 2016; Reisner et al., 2015b; Spear and Swartzwelder, 2014; Swartzwelder et al., 2015).
In a report drawn from the American College Health Association–National College Health Assessment (ACHA-NCHA) survey of 120 institutions (N = 75,192), Coulter et al. (2015) found that transgender students reported heavy episodic drinking more frequently than their cisgender peers, whose biological sex and gender identity are in congruence. Furthermore, transgender students manifested increased suicidal ideation while drinking and a higher likelihood of encountering physical, sexual, and/or verbal assault over the previous year than cisgender students. However, male cisgender students were more likely to report ARBs compared with both transgender and female cisgender students. No differences were observed between transgender and cisgender students with respect to actions they later regretted, encounters with law enforcement, unprotected sex, or physical injuries. Differences between male and female transgender students were not described. In contrast, a study by the Center for Collegiate Mental Health (CCMH; 2016), which analyzed data from 139 college and university counseling centers (N = 100,736), reported that transgender students less frequently engaged in heavy episodic drinking than their cisgender peers. Neither transgender sex differences nor the frequency of ARBs was reported. ARBs constitute a neuropsychological insult and thus are particularly important to understand in college students, who are expected to perform at their peak mental capacity.
Presently, a dearth of literature addresses the issue of ARBs in the college setting, particularly among transgender students. We therefore conducted an investigation of self-reported alcohol consumption in a large sample of newly matriculating transgender collegians and compared them with their cisgender peers. Consistent with Coulter et al. (2015), we hypothesized that transgender students would drink large quantities of alcohol more often than cisgender students. With increasing consumption, we expected these students, in turn, to report a greater frequency of negative ARCs, particularly ARBs. Considering the putative stressors encountered by transgender students, we also hypothesized that they would more often cite stress reduction and social anxiety as motivations for drinking compared with their cisgender peers. In order to investigate the relative influence of biological sex compared with gender, we separately examined male-to-female (MTF) and female-to-male (FTM) transgender students and compared each of these subgroups with cisgender students of the same biological sex or the same gender identity.
MATERIALS AND METHODS
Study Sample and Survey Methods
This study was approved as exempt research by the Duke University Health System Institutional Review Board. Data are reported from a survey administered to first-year students during the fall semester of 2015 as part of AlcoholEdu for College™, an interactive Web-based alcohol-prevention program for college students (Lovecchio et al, 2010; Nguyen et al., 2011, 2013; Wyatt et al., 2013). This survey, which included demographic questions, was administered before students began the course. For the vast majority of schools, students completed the survey before they matriculated on campus for the fall semester. Students were asked about their biological sex to determine blood alcohol concentration (BAC) levels, as well as their gender identity, which included the options of man, woman, transgender, and other. In subsequent text, we use the term “sex,” “males,” and “females” to refer to biological attributes such as those manifested in chromosomal genotypes and the terms “gender,” “men,” and “women” to refer to the culturally defined constructs of gender identity that encompass roles, behaviors, and self-concepts (Erol and Karpyak, 2015; Steensma et al., 2013).
Frequency and Quantity of Alcohol Consumption
In the survey, students were asked: During the past year, have you consumed alcohol (i.e., had more than a few sips of beer, wine, or liquor)? If they responded affirmatively or skipped the question, students were then asked: During the past two weeks, have you consumed alcohol (i.e., had more than a few sips of beer, wine, or liquor)? If students again responded affirmatively, they were asked to complete a retrospective 14-day calendar, from which several measures could be derived, including the number of days on which they consumed at least one drink, the total number of drinks they consumed over the two weeks, and the maximum number of drinks they consumed on any single day.
ARBs and other ARCs
ARCs were examined using an approach based on the Rutgers Alcohol Problem Index (RAPI), a self-administered screening tool for assessment of adolescent drinking problems (White and Labouvie, 1989). Most items from the RAPI were retained, but adaptations were implemented so that the scale better matched the college context. A prior investigation reported an internal-consistency reliability coefficient (Cronbach’s alpha) for the total scale of .91, with subscale reliability coefficients ranging from .79 to .95 (Nguyen et al. 2011). Construct validity has been established in a series of studies (Nguyen et al., 2011, 2013), including a randomized control trial to evaluate AlcoholEdu for College™ (Lovecchio et al., 2010). Students who had consumed alcohol in the past two weeks were asked: During the past two weeks, to what degree did the following happen to you when drinking or as a result of your drinking? Don’t count things that have happened to you but were not because of drinking. Students completed a 7-point Likert scale with 1 = Never and 7 = Always. A response of 2 or greater can be considered an indication of that ARC as a result of drinking. One such ARC was, forgot where you were or what you did, which we report as our operational measure of ARBs.
Motivations for Drinking
Motivations for drinking were assessed using an adaptation of the Drinking Motives Questionnaire–Revised, which has established internal-consistency and test-retest reliability and a well-established factor structure (Arterberry et al., 2012; Cooper, 1994; Kuntsche et al. 2006). Respondents who drank in the past two weeks were asked about their reasons for drinking alcohol: How important to you is each of the following reasons for drinking alcoholic beverages? They completed a 7-point Likert scale, with 1 = Not at all important, 4 = Neutral, and 7 = Very important. A response of 5 or greater can be considered a positive endorsement.
Data Analyses
Analyses were performed using SPSS 22 statistical software. Univariate statistics were computed for the description of demographic variables. Chi-square tests were performed for bivariate analyses of categorical variables (e.g., alcohol consumption during the past year). Results are presented comparing the following groups: a) total male and total female students, b) total cisgender and total transgender students, c) cisgender male and cisgender female students, d) MTF transgender and FTM transgender students, e) cisgender male and MTF transgender students, f) cisgender female and FTM transgender students, g) cisgender male and FTM transgender students, and h) cisgender female and MTF transgender students.
For continuous measures (e.g., number of days of alcohol consumption over the past two weeks), analyses of covariance (ANCOVAs) were computed with biological sex (male, female) and sex-gender congruence (cisgender, transgender) entered as class variables. The interaction between biological sex and sex-gender congruence was also examined. Age and race/ethnicity (dummy coded as 0 = Caucasian/white, 1 = non-Caucasian/white) were entered as covariates. Post-hoc analyses using Tukey’s range test examined the same eight comparisons described above.
For examination of ARCs and motivations for drinking, odds ratios and their 95% confidence intervals (CIs) were computed for cisgender males compared with cisgender females, cisgender compared with transgender students, and MTF compared with FTM transgender students. Analyses were also repeated adjusting for age and race/ethnicity (dummy coded as 0 = Caucasian/white, 1 = non-Caucasian/white). ARCs were dichotomized into present versus absent based on a cut point of 2 or greater on the Likert scale, indicating at least some experience of that ARC while drinking during the past two weeks. Motivations for drinking were dichotomized into agreement or disagreement based on a cut point of 5 or higher, indicating at least minimal agreement.
All responses were voluntary, and students were allowed to skip any questions that they did not wish to address. Thus, specific answers and non-responses influenced the students’ pathway through the survey and created minor discrepancies in sample sizes for specific questions.
RESULTS
Participant Characteristics
Data were collected from 370 colleges and universities. A total of 422,906 newly matriculating students self-reported their biological sex, with 54.9% selecting female. Whereas 99.8% selected man or woman as their gender and the vast majority were congruent with their biological sex, 989 students (0.2%) self-identified as transgender. Classifying students by their biological sex and gender identity for subsequent analyses yielded four distinct groups for comparison: 1) 190,428 cisgender males, 2) 231,500 cisgender females, 3) 395 transgender males identifying as women (MTF), and 4) 583 transgender females identifying as men (FTM). Eleven students identified as transgender but did not provide a biological sex, precluding assignment as MTF or FTM. Most students were 18 years old (79.8%), followed by 17 years old (9.2%) and 19 years old (8.4%). The majority of students self-identified as Caucasian/white (64.4%), followed by Asian/Pacific Islander (11.4%), African American (9.6%), Hispanic/Latino (9.0%), and Native American (0.5%).
Alcohol Consumption in the Past Year
Out of 423,315 students who were asked whether they had consumed an alcoholic beverage in the previous year, 272,738 (64.4%) responded affirmatively, whereas 150,162 (35.5%) responded negatively, and 415 did not answer the question. Bivariate analyses revealed the following: a) male students (64.9%) more often reported drinking than female students (64.2%), χ2 (1, N = 422580) = 20.99, p < .0001; b) cisgender students (64.5%) were statistically equivalent to transgender students (63.6%), χ2 (1, N = 422589) = 0.30, p =.30; c) cisgender males (64.9%) had higher percentages than cisgender females (64.2%), χ2 (1, N = 421604) = 20.16, p < .0001; and d) MTF transgender (67.4%) exceeded FTM transgender students (61.1%), χ2 (1, N = 976) = 3.90, p < .05. No significant difference was observed between e) male cisgender (64.9%) and MTF transgender students (67.4%), χ2 (1, N = 190665) = 1.14, p = .32, or between f) female cisgender (64.2%) and FTM transgender students (61.1%), χ2 (1, N = 231915) = 2.22, p = .14. A significant difference was observed between g) male cisgender and FTM transgender students, χ2 (1, N = 190855) = 3.35, p < .05, but not between h) female cisgender and MTF transgender students, χ2 (1, N = 231725) = 1.78, p =.10.
Alcohol Consumption in the Past Two Weeks
Table 1 presents percentages of students reporting alcohol consumption in the past two weeks a) for the full sample and b) partitioned by biological sex and sex-gender congruence. Of the 273,054 students who had a drink in the past year (or did not answer the question), 159,271 (58.3%) had consumed a drink in the past two weeks, whereas 113,783 responded negatively. Another 150,261 students had missing data for this question either because they did not respond or because they had not had a drink in the past year. Bivariate analyses revealed: a) male students (62.3%) more frequently reported alcohol consumption than female students (55.0%), χ2 (1, N = 272828) = 1459.94, p < .0001; b) transgender students (62.0%) yielded higher percentages than cisgender students (58.3%), χ2 (1, N = 272834) = 3.50, p < .05; c) cisgender males (62.3%) exceeded cisgender females (55.0%), χ2 (1, N = 272205) = 1455.47, p < .0001; and d) MTF transgender students (66.7%) reported higher percentages than FTM transgender students (57.9%), χ2 (1, 623) = 5.00, p < .05. No significant difference was noted between e) male cisgender and MTF transgender students, χ2 (1, N = 123818) = 2.19, p = .15, or between f) female cisgender and FTM transgender students, χ2 (1, N = 149010) = 1.15, p = .29. A significant difference was observed between g) male cisgender and FTM transgender students, χ2 (1, N = 123907) = 2.94, p < .05, and between h) female cisgender and MTF transgender students, χ2 (1, N = 148921) = 14.58, p < .0001.
Table 1.
Self-reported Drinking Frequencies and Quantities in the Past Two Weeks for the Full Sample and by Sex and Sex-Gender Congruence Among Students Who Had an Alcoholic Drink in the Past Year
| Group | Biological Sex | Sample Size | Drank in the Past Two Weeksa,b,c,d,f,g | Total Daysa,b,c,d,e,g | Total Drinksa,b,c,d,e,g | Maximum Drinksa,b,c,d,g |
|---|---|---|---|---|---|---|
| N | % | M ± SD | M ± SD | M ± SD | ||
| Full Sample | 273,054 | 58.3% | 0.29 ± 1.24 | 1.15 ± 6.48 | 1.47 ± 3.16 | |
| Sex-Gender Congruence | ||||||
| Cisgender | Total | 272,217 | 58.3% | 0.29 ± 1.23 | 1.15 ± 6.46 | 1.47 ± 3.16 |
| Male | 123,551 | 62.3% | 0.34 ± 1.43 | 1.57 ± 8.28 | 1.85 ± 3.72 | |
| Female | 148,654 | 55.0% | 0.24 ± 1.06 | 0.82 ± 4.57 | 1.16 ± 2.57 | |
| Transgender | Total | 623 | 62.0% | 0.52 ± 2.18 | 2.28 ± 12.63 | 1.77 ± 4.14 |
| Male (MTF) | 267 | 66.7% | 0.92 ± 3.07 | 4.15 ± 17.28 | 2.22 ± 4.92 | |
| Female (FTM) | 356 | 57.9% | 0.28 ± 1.36 | 1.16 ± 8.59 | 1.44 ± 3.47 |
MTF, male-to-female transgender; FTM, female-to-male transgender. Sex-gender congruence refers to the concordance between biological sex and gender identity. Thus, MTF are biologically male and identify as women; FTM are biologically female and identify as men. Chi-square analyses were computed for reported drinking in the past two weeks; ANCOVAs were applied to mean drinking occasions (total days consuming at least one drink) and quantities (total drinks in the past two weeks and maximum number of drinks on any single day in the past two weeks) using age and race/ethnicity as covariates. Significant mean differences between groups are footnoted as follows:
total males - total females,
cisgender - transgender,
cisgender males - cisgender females,
transgender MTFs - transgender FTMs,
cisgender males - transgender MTFs,
cisgender males - transgender FTMs,
cisgender females - transgender MTFs.
Frequency and Quantity of Alcohol Consumption
Table 1 also presents means and standard deviations for total days students consumed at least one drink, total drinks consumed, and maximum number of drinks consumed on any single day in the past two weeks.
Total Days Students Consumed at Least One Drink
An ANCOVA examining the total number of days that students consumed at least one drink in the past two weeks revealed a) a main effect of sex, with males reporting more total days than females, F(1,287514) = 51.97, p < .0001, and b) a main effect of sex-gender congruence, with transgender students reporting more total days than cisgender students, F(1,287514) = 38.02, p < .0001. A significant Sex × Sex-Gender Congruence interaction was also observed, F(1,287514) = 28.93, p < .0001. Planned pairwise comparisons revealed that more total drinking days were reported by c) cisgender males than cisgender females (p < .0001), d) MTF transgender than FTM transgender students (p < .0001), and e) MTF transgender than male cisgender students (p < .0001). No difference was observed between f) female cisgender and FTM transgender students (p =.93) or between g) male cisgender and FTM transgender students (p =.74), but h) MTF transgender students had higher means than female cisgender students (p < .0001).
Total Drinks Consumed
An ANCOVA examining total drinks consumed during the past two weeks revealed a) a main effect of sex, with males reporting more drinks than females, F(1,287526) = 49.79, p < .0001, and b) a main effect of sex-gender congruence, with transgender students reporting more drinks than cisgender students, F(1,287526) = 32.55, p < .0001. A significant interaction was also observed for Sex × Sex-Gender Congruence, F(1,287526) = 18.92, p < .0001. Mirroring the results for total drinking days, more drinks were consumed by c) cisgender males than cisgender females (p < .0001), d) MTF transgender than FTM transgender students (p < .0001), and e) MTF transgender than male cisgender students (p < .0001). No differences were observed between f) female cisgender and FTM transgender students (p =.71) or between g) male cisgender and FTM transgender students (p =.59), but h) MTF transgender students had higher means than female cisgender students (p < .0001).
Maximum Number of Drinks Consumed on Any Single Day
An ANCOVA examining the maximum number of drinks reported for any single day in the past two weeks revealed a) a main effect of sex, F(1,404939) = 53.97, p < .0001, with males exceeding females, and b) a main effect of sex-gender congruence, F(1,404939) = 17.12, p < .0001, with transgender students exceeding cisgender students. The Sex × Sex-Gender Congruence interaction term was not significant, F(1,404939) = 1.03, p = .31.
For all three ANCOVAs, age and race/ethnicity extracted significant variance as covariates (all p’s < .0001). Younger students and Caucasian/white students reported more days of consumption, total drinks, and maximum number of drinks consumed on any single day in the past two weeks than their older and non-Caucasian/white peers.
ARBs
Table 2 presents ARB results for the full sample and as a function of age and race/ethnicity partitioned by biological sex and sex-gender congruence. In general, the reported frequency of ARBs declined with age, with 18- and 19-year-old students reporting higher values on the Likert scale (1 = Never, 7 = Always). Further, Caucasian/white students reported higher ratings of ARBs than non-Caucasian/white students.
Table 2.
Frequency Ratings of Self-reported Alcohol-Related Blackouts (ARBs) During the Past Two Weeks (1 = Never, 7 = Always) for the Full Sample and for Age and Race/Ethnicity Partitioned by Sex and Sex-Gender Congruence Among Students Who Had an Alcoholic Drink During the Past Two Weeks
| Sex-Gender Congruence
|
||||||||
|---|---|---|---|---|---|---|---|---|
| Cisgender
|
Transgender
|
|||||||
| Group | Statistic | Male | Female | Total | MTF | FTM | Total | |
| Full Sample | N | 158,889 | 76,676 | 81,668 | 158,344 | 177 | 205 | 387 |
| M ± SD | 1.57±1.19 | 1.56±1.71 | 1.57±1.21 | 1.57±1.19 | 2.53±2.17 | 1.77±1.54 | 2.14±1.90 | |
| Age | ||||||||
| 17 | N | 11,985 | 4,470 | 7,462 | 11,932 | 17 | 20 | 38 |
| M ± SD | 1.53±1.17 | 1.51±1.14 | 1.54±1.17 | 1.53±1.16 | 2.12±1.87 | 1.75±1.77 | 1.97±1.81 | |
| 18 | N | 128,767 | 60,771 | 67,621 | 128,392 | 111 | 150 | 264 |
| M ± SD | 1.57±1.20 | 1.57±1.17 | 1.58±1.22 | 1.57±1.19 | 2.45±2.14 | 1.70±1.48 | 2.03±1.83 | |
| 19 | N | 13,716 | 8,816 | 4,848 | 13,664 | 20 | 16 | 36 |
| M ± SD | 1.60±1.23 | 1.60±1.22 | 1.58±1.25 | 1.59±1.23 | 3.45±2.33 | 2.00±1.37 | 2.81±2.07 | |
| 20 | N | 1,375 | 875 | 487 | 1,362 | 7 | 3 | 10 |
| M ± SD | 1.52±1.16 | 1.56±1.17 | 1.44±1.12 | 1.52±1.16 | 1.57±1.13 | 2.33±1.53 | 1.80±1.23 | |
| 21 | N | 753 | 483 | 264 | 747 | 3 | 3 | 6 |
| M ± SD | 1.41±1.05 | 1.44±1.09 | 1.33±0.97 | 1.40±1.05 | 2.00±1.73 | 1.67±0.58 | 1.83±1.17 | |
| 22 | N | 393 | 246 | 144 | 390 | 2 | 1 | 3 |
| M ± SD | 1.45±1.12 | 1.48±1.16 | 1.30±0.83 | 1.42±1.06 | 4.50±3.54 | 7.00±0.00 | 5.33±2.89 | |
| 23 | N | 321 | 203 | 114 | 317 | 1 | 2 | 3 |
| M ± SD | 1.22±0.74 | 1.27±0.81 | 1.11±0.47 | 1.21±0.71 | 7.00±0.00 | 1.00±0.00 | 3.00±3.46 | |
| 24+ | N | 1,484 | 774 | 681 | 1,455 | 16 | 10 | 27 |
| M ± SD | 1.26±0.91 | 1.29±0.96 | 1.18±0.72 | 1.24±0.86 | 2.38±2.42 | 1.90±1.91 | 2.33±2.29 | |
| Race | ||||||||
| Non-Caucasian/White | N | 38,877 | 18,232 | 20,432 | 38,665 | 95 | 68 | 163 |
| M ± SD | 1.52±1.19 | 1.53±1.19 | 1.51±1.18 | 1.52±1.19 | 2.96±2.47 | 1.94±1.76 | 2.53±2.25 | |
| Caucasian/White | N | 119,536 | 58,196 | 61,024 | 119,220 | 80 | 137 | 222 |
| M ± SD | 1.58±1.19 | 1.57±1.17 | 1.59±1.22 | 1.58±1.19 | 2.05±1.67 | 1.68±1.41 | 1.86±1.55 | |
MTF, male-to-female transgender; FTM, female-to-male transgender. Respondents were asked: During the past two weeks, to what degree did the following happen to you when drinking or as a result of your drinking? Don’t count things that have happened to you but were not because of drinking (1 = Never, 7 = Always). Item: Forgot where you were or what you did?
An ANCOVA examining ARB values revealed a) a significant main effect of sex, F(1,158185) = 42.09, p < .0001, with males experiencing ARBs more frequently than females, and b) a main effect of sex-gender congruence, F(1,158185) = 99.86, p < .0001, with ARBs reported more frequently by transgender than cisgender students. The Sex × Sex-Gender Congruence interaction was also significant, F(1,158185) = 42.66, p < .0001. Pairwise comparisons revealed the following: c) no difference was observed between cisgender males and cisgender females (p = .75); d) MTF transgender students provided higher ratings than FTM transgender students (p < .001); e) MTF transgender students exceeded male cisgender students (p < .001); f) no difference was observed between female cisgender and FTM transgender students (p =.09); g) no difference was found between male cisgender and FTM transgender students (p =.07); and h) MTF transgender students exceeded female cisgender students (p < .0001). In this ANCOVA, the covariates age and race/ethnicity extracted significant variance (both p’s < .0001). ARB means and standard deviations for the four groups representing variations in sex-gender congruence are depicted in Figure 1.
Fig. 1.
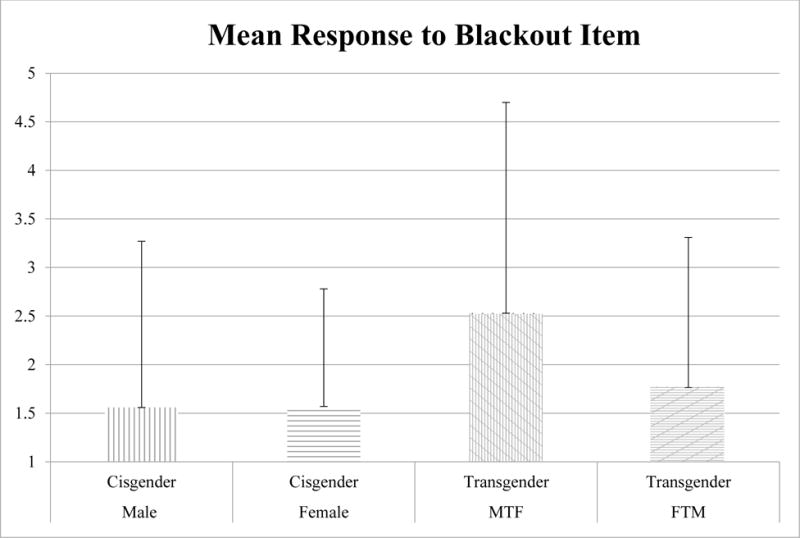
Mean and standard deviation of self-reported alcohol-related blackouts (ARBs) during the past two weeks on a Likert rating scale (1 = Never, 7 = Always) by sex and sex-gender congruence among students who had an alcoholic drink in the past two weeks. MTF, male-to-female; FTM, female-to-male.
ARCs
Table 3 presents the percentage of students reporting any experience of negative ARCs, including ARBs, as a result of drinking during the previous two weeks. Odds ratios and 95% CIs compare ARCs for cisgender males to cisgender females, MTF transgender to FTM transgender students, and cisgender students to transgender students. In general, transgender students were more likely than cisgender students to report a negative consequence. Cisgender males were more likely to report negative ARCs than cisgender females, and MTF transgender students were more likely to experience negative ARCs than FTM transgender students.
Table 3.
Percentages of Students Self-reporting Negative Alcohol-Related Consequences by Sex and Sex-Gender Congruence for Students Who Had an Alcoholic Drink During the Past Two Weeks
| Sex-Gender Congruence
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|
| Cisgender
|
Transgender
|
Cisgender vs. Transgender | |||||||
| Negative Alcohol-Related Consequence | Total % |
Male % |
Female % |
Odds Ratio (95% CI) |
Total % |
MTF % |
FTM % |
Odds Ratio (95% CI) |
Odds Ratio (95% CI) |
| Forgot where you were or what you did | 25% | 26% | 25% | 1.1 (1.0–1.1) | 36% | 46% | 27% | 2.3 (1.5–3.6) | 1.7 (1.4–2.1) |
| Got a hangover | 44% | 44% | 44% | 1.0 (0.9–1.0) | 43% | 44% | 40% | 1.2 (0.8–1.8) | 1.0 (0.8–1.2) |
| Passed out | 13% | 15% | 11% | 1.5 (1.4–1.5) | 26% | 34% | 16% | 2.6 (1.6–4.2) | 2.3 (1.9–2.9) |
| Did something you regretted | 24% | 24% | 24% | 1.0 (0.9–1.0) | 32% | 39% | 25% | 2.0 (1.3–3.0) | 1.5 (1.2–1.8) |
| Felt sick to your stomach | 41% | 39% | 43% | 0.9 (0.9–0.9) | 46% | 47% | 44% | 1.1 (0.7–1.7) | 1.2 (1.0–1.5) |
| Performed poorly on an assignment/test or got behind in school work | 6% | 7% | 5% | 1.5 (1.4–1.5) | 22% | 28% | 16% | 2.1 (1.2–3.4) | 4.2 (3.3–5.3) |
| Missed a class | 4% | 5% | 4% | 1.5 (1.4–1.6) | 20% | 27% | 13% | 2.4 (1.4–4.1) | 5.3 (4.1–6.8) |
| Missed going to work | 4% | 5% | 4% | 1.5 (1.5–1.6) | 20% | 28% | 13% | 2.6 (1.6–4.5) | 5.3 (4.1–6.8) |
| Injured yourself | 13% | 13% | 13% | 1.0 (0.9–1.0) | 25% | 34% | 16% | 2.6 (1.6–4.3) | 2.2 (1.8–2.8) |
| Got involved in a physical fight or injured another person | 5% | 8% | 3% | 2.8 (2.7–3.1) | 22% | 32% | 13% | 3.3 (1.9–5.5) | 5.1 (4.0–6.4) |
| Damaged property | 6% | 9% | 4% | 2.7 (2.5–2.8) | 22% | 31% | 13% | 3.0 (1.8–5.2) | 4.0 (3.1–5.1) |
| Drove after drinking 4 or more drinks | 6% | 8% | 5% | 1.8 (1.7–1.9) | 22% | 29% | 15% | 2.3 (1.4–3.8) | 4.2 (3.3–5.4) |
| Drove after drinking 5 or more drinks | 4% | 6% | 3% | 2.3 (2.2–2.4) | 21% | 28% | 14% | 2.5 (1.5–4.2) | 5.6 (4.4–7.2) |
| Rode with a driver who had been drinking | 13% | 13% | 13% | 1.0 (0.9–1.0) | 27% | 33% | 21% | 1.8 (1.1–2.8) | 2.4 (2.0–3.1) |
| Strained a relationship with a friend | 11% | 11% | 11% | 1.0 (1.0–1.0) | 24% | 30% | 19% | 1.8 (1.1–2.9) | 2.5 (2.0–3.2) |
| Was argumentative | 19% | 20% | 18% | 1.1 (1.1–1.2) | 32% | 39% | 26% | 1.8 (1.2–2.8) | 2.1 (1.7–2.5) |
| Got into trouble with the authorities | 4% | 5% | 3% | 1.7 (1.7–1.8) | 19% | 23% | 12% | 2.7 (1.6–4.6) | 5.3 (4.1–6.8) |
| Deliberately vomited to continue drinking | 5% | 7% | 4% | 1.7 (1.6–1.8) | 21% | 30% | 14% | 2.7 (1.6–4.5) | 4.9 (3.8–6.3) |
| Embarrassed yourself | 29% | 26% | 31% | 0.8 (0.7–0.8) | 40% | 45% | 35% | 1.5 (1.0–2.2) | 1.6 (1.3–2.0) |
| Been taken advantage of sexually | 8% | 5% | 10% | 0.5 (0.5–0.5) | 19% | 23% | 15% | 1.7 (1.1–2.7) | 2.6 (2.1–3.3) |
| Taken advantage of someone sexually | 3% | 4% | 2% | 2.3 (2.2–2.4) | 13% | 18% | 8% | 2.4 (1.4–4.0) | 4.8 (3.7–6.1) |
MTF, male-to-female transgender; FTM, female-to-male transgender; CI, confidence interval. Respondents were asked: During the past two weeks, to what degree did the following happen to you when drinking or as a result of your drinking? Don’t count things that have happened to you but were not because of drinking (1 = Never, 7 = Always). Reported percentages are for students who responded with a value ≥ 2.
Whereas transgender students were only slightly more likely to report any physical consequences (e.g., felt sick to your stomach), they were substantially more likely to acknowledge negative academic (e.g., missed a class), confrontational (e.g., got involved in a physical fight, got into trouble with the authorities), social (e.g., strained a relationship with a friend, embarrassed yourself), and sexual consequences (e.g., been taken advantage of sexually). The differences between cisgender and transgender students were significant at p <.0001 with the exception of only one type of negative ARC: got a hangover. All significant differences remained so after covarying for age and race/ethnicity (p < .0001). Younger and Caucasian/white students were more likely to report ARCs than their older and non-Caucasian/white peers. The differences between cisgender and transgender students were also significant after controlling for ARBs statistically (p < .001).
Motivations for Drinking
Motivations for drinking are presented in Table 4 together with odds ratios and 95% CIs comparing groups partitioned by sex and sex-gender congruence. Students who identified as transgender were more likely to endorse most of the assessed reasons for drinking compared with their cisgender peers. MTF transgender students yielded higher percentages than FTM transgender students, whereas this difference in magnitude was not as large or consistent when comparing cisgender males with cisgender females.
Table 4.
Percentage of Students Endorsing Motivations for Drinking Alcohol by Sex and Sex-Gender Congruence Among Students Who Had an Alcoholic Drink in the Past Two Weeks
| Sex-Gender Congruence
|
|||||||||
|---|---|---|---|---|---|---|---|---|---|
| Cisgender
|
Transgender
|
Cisgender vs. Transgender | |||||||
| Motivation for Drinking | Total % |
Male % |
Female % |
Odds Ratio (95% CI) |
Total % |
MTF % |
FTM % |
Odds Ratio (95% CI) |
Odds Ratio (95% CI) |
| To get drunk | 29% | 31% | 27% | 1.2 (1.2–1.2) | 31% | 38% | 27% | 1.7 (1.2–2.4) | 1.1 (1.0–1.3) |
| To relieve stress | 16% | 15% | 17% | 0.9 (0.9–0.9) | 22% | 25% | 19% | 1.4 (0.9–2.0) | 1.4 (1.2–1.7) |
| Because you like the taste | 22% | 24% | 21% | 1.2 (1.2–1.2) | 26% | 30% | 24% | 1.4 (1.0–2.0) | 1.2 (1.0–1.5) |
| To have a good time with your friends | 60% | 65% | 55% | 1.6 (1.5–1.6) | 50% | 58% | 45% | 1.7 (1.2–2.3) | 0.7 (0.6–0.8) |
| To celebrate | 58% | 62% | 56% | 1.3 (1.2–1.3) | 48% | 55% | 44% | 1.5 (1.1–2.1) | 0.7 (0.6–0.8) |
| To experiment | 20% | 19% | 21% | 0.9 (0.9–0.9) | 23% | 27% | 20% | 1.5 (1.1–2.2) | 1.2 (1.0–1.4) |
| To decrease inhibitions | 9% | 10% | 9% | 1.2 (1.1–1.2) | 15% | 22% | 10% | 2.7 (1.7–4.3) | 1.7 (1.3–2.1) |
| Feel happy | 26% | 25% | 27% | 1.0 (0.9–1.0) | 29% | 38% | 23% | 2.1 (1.5–2.9) | 1.2 (1.0–1.4) |
| Feel more attractive | 10% | 9% | 11% | 0.7 (0.7–0.8) | 16% | 21% | 12% | 1.9 (1.2–2.9) | 1.7 (1.4–2.1) |
| Feel more confident or sure of yourself | 19% | 18% | 19% | 0.9 (0.9–1.0) | 22% | 28% | 17% | 1.8 (1.2–2.7) | 1.2 (1.0–1.5) |
| Feel comfortable pursuing an opportunity to have sex | 9% | 12% | 6% | 2.2 (2.1–2.3) | 15% | 24% | 9% | 3.3 (2.0–5.2) | 1.8 (1.5–2.3) |
| Feel connected with the people around you | 31% | 35% | 28% | 1.4 (1.4–1.4) | 30% | 36% | 25% | 1.6 (1.2–2.3) | 0.9 (0.8–1.1) |
MTF, male-to-female transgender; FTM, female-to-male transgender; CI, confidence interval. Respondents were asked to rate the importance of each potential reason for drinking (1 = Not at All Important, 4 = Neutral, 7 = Very Important). Reported percentages are for students who responded with a value ≥ 5.
Among the motivations assessed, cisgender students were more likely to drink for positive social reasons, including to have a good time with your friends and to celebrate, whereas transgender respondents were more likely to identify negative reasons related to stressful experiences, social anxiety, and self-esteem, including to relieve stress, decrease inhibitions, feel more attractive, and feel more comfortable pursuing an opportunity to have sex. Transgender students were also motivated by a greater affinity for the properties of alcohol itself, e.g., to get drunk, because you like the taste, to experiment, and to feel happy.
We examined the preceding effects with age and race/ethnicity entered as covariates and found that younger and Caucasian/white students were generally more likely to endorse all reasons for drinking alcohol than older and non-Caucasian/white students. All motivations for drinking remained significant at p < .01 when these covariates were included in the analyses with the exception of to get drunk and to feel connected with the people around you, both of which were non-significant.
DISCUSSION
Few studies have examined motivations for drinking, level of alcohol consumption, ARB rates, and other adverse ARCs among transgender college students. To our knowledge, the present report utilizes the largest dataset to examine these important issues. All three of our hypotheses were supported. Specifically, our results were consistent with prior literature reporting that transgender college students drink more frequently and in greater quantities per drinking episode than their cisgender peers. Notably, transgender students also cited a greater frequency of ARBs as well as a variety of other harmful ARCs, consistent with their consumption patterns. Transgender students cited stress reduction and interpersonal concerns more often as motivations for drinking compared with their cisgender peers.
Our reported percentage of 0.2% transgender first-year students was close to the figure for all class years of 0.3% reported by the CCMH (Center for Collegiate Mental Health, 2016), Coulter et al.’s (2015) figure of 0.23% from the ACHA-NCHA survey (2011 – 2013), and Diemer et al.’s (2015) report of 0.17% from an earlier ACHA-NCHA survey (2008 – 2011) of 289,024 students from 223 colleges and universities. However, the CCMH investigation reported lower rates of heavy episodic (“binge”) drinking (defined as five or more drinks in a row for males, four or more in a row for females) for transgender students, in contrast to the higher drinking levels found in the present survey. This difference between the two results could partially derive from divergent sampling (counseling-center clients versus the general student population) or different MTF:FTM ratios, data not reported in the CCMH study. In addition, the present survey used a set of continuous alcohol-consumption measures, which were likely more sensitive than the dichotomous classification adopted by the CCMH. Our findings were furthermore consistent with those of Coulter et al. (2015), who reported a greater frequency of days of heavy episodic drinking (defined as five or more drinks at a sitting) for transgender compared with cisgender students. While greater quantities of alcohol use enhance the odds of an ARB episode, other factors can additionally come into play. We speculate that some other unexamined determinant—perhaps body mass index (BMI) or rapidity of intake—may contribute to greater vulnerability to ARBs in transgender students in the presence of lower alcohol consumption.
Evidence suggests that college students may experience ARBs with previously unrecognized prevalence (White et al., 2002, 2004). Such events represent substantive neuropsychological insults, the sequelae of which convey considerable immediate personal risk in addition to their associations with both short- and long-term damaging health and psychological outcomes (Goodwin, 1995; White, 2003). ARB experiences are also strongly associated with other immediate negative ARCs, especially driving after drinking, damaging property, conflicts with authorities, sexual exploitation of others, and experiencing sexual assault (White et al., 2002, 2004). In fact, we observed that transgender students cited a wide variety of harmful ARCs, in addition to ARBs, compared with cisgender students. Particular differences were observed for negative academic, confrontation-related, social, and sexual consequences. Differences of lesser magnitude were observed for physical consequences. The findings remained significant after controlling for ARBs statistically, indicating that these ARCs were not confined to pharmacologically induced dissociation.
Our findings raise an additional concern, as BAC levels below those typically associated with full ARBs have been shown to impair learning and memory with greater efficacy in college-aged individuals than in persons several years older (Acheson et al., 1998). This outcome could arise from a greater suppression of memory-related circuit and synaptic function in the hippocampal formation in younger individuals as has been demonstrated in animal models of adolescent alcohol exposure (Fleming et al., 2007; Markwiese et al., 1998; Swartzwelder et al., 1995). In addition to these differences in acute alcohol sensitivity between late adolescence and adulthood, repeated exposure to high doses of alcohol during adolescence has been shown to cause persistent changes in neural function in adulthood (Spear and Swartzwelder, 2014). Whether these long-term changes are the result of neurotoxic effects, epigenetic modulations, or alterations of the late developmental trajectory of neural circuits is an area of active investigation at present. However, given such findings, the higher BAC levels typically required to induce ARBs raise additional alarm over the potentially adverse neuropsychological implications for these students.
Examination of biological-sex versus gender-identity contributions to alcohol consumption reflected influences of both. For all continuous measures of frequency and quantity of drinking, a statistically significant main effect was observed showing males to exceed females within the cisgender group, the transgender group, and collapsed across sex-gender congruence. However, no differences were observed comparing female cisgender to FTM transgender students. Such results suggest a dominance of biological over gender-related influences on drinking presentations. Findings for the measures of drinking quantity were not surprising given typically higher BMIs in men, smaller volume of distribution in females, and other sex differences impacting pharmacokinetics and requiring greater intake over time for males to achieve BAC levels equivalent to females (Erol and Karpyak, 2015). However, measures of drinking frequency are more reflective of psychological influences and therefore potentially more tied to masculine gender identity combined with greater normative acceptance of drinking for men (Erol and Karpyak, 2015; Nolen-Hoeksema, 2004). The findings indicating a lack of significant differences between male cisgender and FTM transgender students may reflect such psychosocial influences manifested in the adoption of more prototypically masculine behaviors by this transgender subgroup. In short, both biological and sociocultural contributions likely come into play in accounting for alcohol-consumption patterns.
Significant main effects for all continuous measures of frequency and quantity of alcohol consumption were also observed for sex-gender congruence. These results may reflect psychosocial influences of a different origin than those governing masculine behavioral norms, viz., those pertinent to gender non-conformity. In this regard, structural stigma and discrimination in a heteronormative society have been hypothesized to represent key contributors to adverse health and psychological outcomes in transgender men and women, both by inducing stress and by restricting access to needed healthcare resources (Cruz, 2014; Hughto et al., 2015; Klein and Golub, 2016; Miller and Grollman, 2015). Transgender students in emerging adulthood may be particularly vulnerable to these sociocultural forces and their psychological impacts upon entry into college. In addition to coping with any hostility they experienced within their family and in secondary school (Case and Meier, 2014; Grossman et al., 2005; Klein and Golub, 2016), these students must prepare for and then navigate a new set of interpersonal and institutional challenges upon college matriculation. Whereas all respondents were most likely to drink for social reasons such as celebration and convivial interactions with friends, transgender students were significantly more likely than their cisgender peers to drink for reasons relating to stress, social anxiety, and self-esteem, confirming our hypothesis. These students also endorsed drinking for reasons related to the inherent characteristics of alcohol, such as its gustatory and euphoria-inducing properties. To date, little other research has examined these students’ motivations for drinking. The results of the present study suggest that regulating negative affect and enhancing confidence may be particularly salient motives among transgender students. Understanding the varying drinking-related motivations of students who experience ARBs is likely to be important and useful in intervening with these at-risk collegians regardless of their sex or gender identity.
In addition to the main effects of biological sex and sex-gender congruence, a Sex × Sex-Gender Congruence interaction was observed. Specifically, the most extreme results across frequency and quantity of alcohol consumption, ARBs, other ARCs, and motivations for drinking were consistently noted for the MTF transgender group compared with cisgender males, FTM transgender students, and cisgender females. These results represented a robust driver of the findings for the transgender group as a whole. Beyond the previously described contributions of natal sex, a number of additional biological factors may govern transgender presentations, such as genetic, intrauterine, endocrine, immunological, and neurogenic determinants (Bao and Swaab, 2011; Smith et al., 2015; Saraswat et al., 2015; Steensma et al., 2013). For example, genital differentiation occurs earlier in fetal development than sexually dimorphic brain organization, which may account for gender identity divergent from biological sex, as well as contrasting features of MTF and FTM transgender expression (Bao and Swaab, 2011; Smith et al., 2015). Postmortem examination and magnetic resonance imaging have suggested transgender-specific differences in hypothalamic-nuclei volume and neuronal number, white-matter microstructure and connectivity, gray-matter morphometry, cortical thickness, and neural-activation responses to specific sensory inputs (Bao and Swaab, 2011; Smith et al., 2015; Saraswat et al., 2015; Steensma et al., 2013).
Prior literature has also observed that differences between MTF and FTM transgender children and adults exist with respect to their experiences of social expectations (Hughto et al., 2015; Rankin and Beemyn, 2012). In many societies, greater normative acceptance is accorded for opposite-gender behavior in girls, who are permitted to be “tomboys.” Title IX legislation has fostered greater sports participation by women—a formerly male-dominated collegiate activity—promoting greater acceptance of nontraditional gender behaviors for coeds. Conversely, boys who engage in culturally defined feminine behavior tend to be swiftly censured and redirected by their parents, teachers, and peers, often by means of aggression to the point of verbal, physical, or sexual abuse (Grossman et al., 2005; Rankin and Beemyn, 2012; Toomey et al., 2012). Overall, transgender men (FTM) are less likely to be perceived as gender nonconforming and face less discrimination than transgender women (MTF; Hughto et al., 2015; Miller and Grollman, 2015). The greater transphobia encountered by transgender women may contribute to a greater observed prevalence of psychiatric disorders (Hoshiai et al., 2010; Smith et al., 2015) and render them more susceptible to alcohol and other substance misuse (Cochran and Cauce, 2006; Keuroghlian et al., 2015; Rowe et al., 2015).
Interactions between biological and psychological contributions may also exert effects. For example, following high levels of alcohol consumption in men, testosterone levels decrease and blood estradiol levels increase, whereas for women levels of both hormones increase (Erol and Karpyak, 2015). These differential neuroendocrine influences might result in a male garnering a sense of femininity but have minimal impact on a female. Thus, increased levels of alcohol may be positively reinforcing for a MTF transgender student seeking to experience a feminine gender identity, resulting in a higher level of alcohol consumption and more negative ARCs. This phenomenon could underlie motivations for drinking tied to the intrinsic properties of alcohol. In contrast, a FTM transgender student might not find alcohol as reinforcing as a MTF transgender student. In short, results for the MTF subgroup may reflect a synergy between alcohol effects and male biology, transgender-specific alterations in brain structure and function, and sociocultural influences specific to gender-identity phenomenology and sex-gender congruence impacting psychosocial adjustment and leading to maladaptive drinking.
The interplay of biological and gender-related influences on drinking behavior is complex and calls for further study. If our work is replicated, particular efforts are required to refine understanding of the unique biopsychosocial characteristics specific to MTF transgender students, who appear to be at particular risk for hazardous drinking, ARBs, and other adverse ARCs. Further empirical work is also indicated to more definitively characterize sex differences in transgender presentations, as some of our findings were discrepant from prior literature. For example, Conron et al. (2012) found no differences in self-reported heavy episodic (“binge”) drinking in the past 30 days between MTF transgender and either FTM transgender or cisgender participants in a population-based household survey of Massachusetts residents 18 to 64 years old. Smalley et al. (2016), using a measure of drinking over five drinks at a time assessed with an online convenience sample averaging 28.9 ± 11.4 years old, reported that non-heterosexual cisgender males drank more than MTF but not FTM transgender participants, and no differences were observed between MTF and FTM transgender respondents. Likewise, no differences were observed between the two transgender subgroups in relation to each other or to cisgender participants in self-reported driving while intoxicated, and non-heterosexual cisgender females reported more frequent sex under the influence than MTF transgender respondents (Smalley et al., 2016). Discrepancies from the present findings may stem from smaller samples with differing compositions, particularly with respect to age and college-matriculation status, as well as the somewhat differing content of the survey questions.
Limitations and Implications
Limitations of our study must be acknowledged in relation to sampling procedures, operational measures, and statistical inferences. The data collected by AlcholEdu for College™ do not reflect a random sample of colleges and universities but rather a subset of institutions that elected to introduce the curriculum as a requirement for their first-year class. The data reflect one cross-sectional examination of newly matriculating students and do not address the impact of drinking culture or the wider college-related experience per se. We only surveyed students that were predominantly young adults and thus cannot generalize to non-collegians or to an older transgender cohort. The status of AlcholEdu for College™ as a requirement rather than a voluntary activity may have affected response characteristics. Some students may have been reluctant to embrace a transgender label despite the anonymity of the Web-based assessment, thus effectively reducing our sample.
Furthermore, our data were based on self-reported measures of alcohol consumption rather than direct determinations of BACs. Likewise, we relied on retrospective self-report rather than direct observations of ARBs, which by definition influence memory recall and cognitive integrity and could diminish response accuracy. Moreover, ARBs were defined by a single-item Likert scale labeled from Never to Always at its endpoints and referred to a single two-week period without factoring in the number of drinking episodes during that time interval. We speculate that many of our transgender respondents encountered stigma, discrimination, and other stressors, but we did not acquire direct measures of these constructs. More comprehensive, observational, and biologically based measures are indicated for future work.
Finally, multiple items assessing ARCs and motivations for drinking were analyzed individually rather than incorporating them as unitary scales, although adapted from psychometric instruments previously validated in a series of studies examining college students (Lovecchio et al., 2010; Nguyen et al., 2011, 2013). While a robustly powered sample size can be considered a strength of our study, the resulting significance levels should not be over-interpreted. As an example, we observed statistical significance indicating that 64.9% of males drank in the past year compared with 64.2% of females, which was significant at p < .0001. However, these differences cannot be considered clinically significant.
Clinical significance that clearly follows from our findings includes the importance of attending to negative motivations for drinking that can fuel hazardous consumption. For example, addressing the needs of transgender students through educational offerings may serve to promote their mental health and diminish the impulse to drink to bolster self-esteem or address social anxiety. Imparting protective-drinking strategies may be particularly useful (Nguyen et al., 2013). A collegiate milieu that fosters acceptance of the transgender student population is also indicated to address the issue. Conversely, structural or institutional discrimination may increase the prevalence of heavy drinking and the risk of ARBs and other pernicious ARCs. Thus, broad administrative efforts are required to reduce alcohol-related risk factors among transgender men and women. Attention to the special circumstances of these vulnerable students is warranted with respect to bathrooms, locker rooms, housing, medical services, healthcare documentation, names as displayed on college directories, and counseling services (Rankin and Beemyn, 2012).
Acknowledgments
We dedicate this paper to the memory of Todd M. Wyatt, Ph.D., who passed away all too soon for a young man of such talent, humor, and warmth. We gratefully acknowledge his many contributions to the Duke Consortium for the Study of the American College Student (CSACS). We thank EverFi, Inc. for the gift of the AlcoholEdu for College™ dataset to the CSACS. Dr. Zapp receives financial support from EverFi, Inc. of Washington, D.C., as the company’s Director of Research. Additionally, Dr. DeJong is an independent consultant for EverFi, Inc. We also thank Dr. Philip Meilman, Dr. Scott Compton, and Ambika Menon for their feedback in the development of this manuscript.
SOURCE OF SUPPORT: H. Scott Swartzwelder was supported by a Senior Research Career Scientist award from the U.S. Department of Veterans Affairs and by NIH grant 2U01AA019925 (NADIA). Drs. Zapp and DeJong receive support from EverFi, Inc.
References
- Acheson SK, Stein RM, Swartzwelder HS. Impairment of semantic and figural memory by acute ethanol: age-dependent effects. Alcohol Clin Exp Res. 1998;22:1437–1442. doi: 10.1111/j.1530-0277.1998.tb03932.x. [DOI] [PubMed] [Google Scholar]
- Arterberry BJ, Martens MP, Cadigan JM, Smith AE. Assessing the dependability of drinking motives via generalizability theory. Addict Res Theory. 2012;45:292–302. doi: 10.1177/0748175612449744. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bao A-M, Swaab DF. Sexual differentiation of the human brain: relation to gender identity, sexual orientation and neuropsychiatric disorders. Front Neuroendocrinol. 2011;32:214–226. doi: 10.1016/j.yfrne.2011.02.007. [DOI] [PubMed] [Google Scholar]
- Bith-Melander P, Sheoran B, Sheth L, Bermudez C, Drone J, Wood W, Schroeder K. Understanding sociocultural and psychological factors affecting transgender people of color in San Francisco. J Assoc Nurses AIDS Care. 2010;21:207–220. doi: 10.1016/j.jana.2010.01.008. [DOI] [PubMed] [Google Scholar]
- Bradford J, Reisner SL, Honnold JA, Xavier J. Experiences of transgender-related discrimination and implications for health: results from the Virginia Transgender Health Initiative Study. Am J Public Health. 2013;103:1820–1829. doi: 10.2105/AJPH.2012.300796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown SA, McGue M, Maggs J, Schulenberg J, Hingson R, Swartzwelder S, Martin C, Chung T, Tapert SF, Sher K, Winters KC, Lowman C, Murphy S. Underage alcohol use: summary of developmental processes and mechanisms: ages 16–20. Alcohol Res Health. 2009;32:41–52. [PMC free article] [PubMed] [Google Scholar]
- Case KA, Meier SC. Developing allies to transgender and gender-nonconforming youth: training for counselors and educators. J LGBT Youth. 2014;11:62–82. [Google Scholar]
- Center for Collegiate Mental Health. (Publication No. STA 15-108).2015 Annual Report. 2016 Available at: http://ccmh.psu.edu/wp-content/uploads/sites/3058/2016/01/2015_CCMH_Report_1-18-2015.pdf. Accessed 6/4/2016.
- Cochran BN, Cauce AM. Characteristics of lesbian, gay, bisexual, and transgender individuals entering substance abuse treatment. J Subst Abuse Treat. 2006;30:135–146. doi: 10.1016/j.jsat.2005.11.009. Available at : http://ccmh.psu.edu/wp-content/uploads/sites/3058/2016/01/2015_CCMH_Report_1-18-2015.pdf. Accessed 6/4/2016. [DOI] [PubMed] [Google Scholar]
- Conron KJ, Scott G, Stowell GS, Landers SJ. Transgender health in Massachusetts: results from a household probability sample of adults. Am J Public Health. 2012;102:118–122. doi: 10.2105/AJPH.2011.300315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cooper ML. Motivations for alcohol use among adolescents: development and validation of a four-factor model. Psychol Assess. 1994;6:117–128. [Google Scholar]
- Cooper ML. Alcohol use and risky sexual behavior among college students and youth: evaluating the evidence. J Stud Alcohol Suppl. 2002;14:101–117. doi: 10.15288/jsas.2002.s14.101. [DOI] [PubMed] [Google Scholar]
- Coulter RWS, Blosnich JR, Bukowski LA, Herrick AL, Siconolfi DE, Stall RD. Differences in alcohol use and alcohol-related problems between transgender- and nontransgender-identified young adults. Drug Alcohol Depend. 2015;154:251–259. doi: 10.1016/j.drugalcdep.2015.07.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Coulter RWS, Kenst KS, Bowen DJ, Scout Research funded by the National Institutes of Health on the health of lesbian, gay, bisexual, and transgender populations. Am J Public Health. 2014;104:e105–e112. doi: 10.2105/AJPH.2013.301501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cruz TM. Assessing access to care for transgender and gender nonconforming people: a consideration of diversity in combating discrimination. Soc Sci Med. 2014;110:65–73. doi: 10.1016/j.socscimed.2014.03.032. [DOI] [PubMed] [Google Scholar]
- DeJong W, Schneider SK, Towvim LG, Murphy MJ, Doerr EE, Simonsen NR, Mason KE, Scribner RA. A multisite randomized trial of social norms marketing campaigns to reduce college student drinking. J Stud Alcohol. 2006;67:868–879. doi: 10.15288/jsa.2006.67.868. [DOI] [PubMed] [Google Scholar]
- Diemer EW, Grant JD, Munn-Chernoff MA, Patterson DA, Duncan AE. Gender identity, sexual orientation, and eating-related pathology in a national sample of college students. J Adolesc Health. 2015;57:144–149. doi: 10.1016/j.jadohealth.2015.03.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erol A, Karpyak VM. Sex and gender-related differences in alcohol use and its consequences: contemporary knowledge and future research considerations. Drug Alcohol Depend. 2015;156:1–13. doi: 10.1016/j.drugalcdep.2015.08.023. [DOI] [PubMed] [Google Scholar]
- Fleming RL, Wilson WA, Swartzwelder HS. Magnitude and ethanol sensitivity of tonic GABAA receptor-mediated inhibition in dentate gyrus changes from adolescence to adulthood. J Neurophysiol. 2007;97:3806–3811. doi: 10.1152/jn.00101.2007. [DOI] [PubMed] [Google Scholar]
- Goodwin DW. Alcohol amnesia. Addiction. 1995;90:315–317. doi: 10.1111/j.1360-0443.1995.tb03779.x. [DOI] [PubMed] [Google Scholar]
- Graham D. ‘State-sponsored discrimination’: Loretta Lynch takes on North Carolina’s bathroom bill. 2016 Available at: http://www.theatlantic.com/politics/archive/2016/05/state-sponsored-discrimination-loretta-lynch-takes-on-north-carolinas-hb2/481986/. Accessed 6/16/2016.
- Grinberg E. Feds issue guidance on transgender access to school bathrooms. 2016 Available at: http://www.cnn.com/2016/05/12/politics/transgender-bathrooms-obama-administration/. Accessed 6/4/2016.
- Grossman AH, D’Augelli AR, Howell TJ, Hubbard S. Parents’ reactions to transgender youths’ gender nonconforming expression and identity. J Gay Lesbian Soc Serv. 2005;18:3–16. [Google Scholar]
- Hendricks ML, Testa RJ. A conceptual framework for clinical work with transgender and gender nonconforming clients: an adaptation of the Minority Stress Model. Prof Psychol: Res Pr. 2012;43:460–467. [Google Scholar]
- Hingson R, Zha W, Simons-Morton B, White A. Alcohol-induced blackouts as predictors of other drinking related harms among emerging young adults. Alcohol Clin Exp Res. 2016;40:776–784. doi: 10.1111/acer.13010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoshiai M, Matsumoto Y, Sato T, Ohnishi M, Okabe N, Kishimoto Y, Terada S, Kuroda S. Psychiatric comorbidity among patients with gender identity disorder. Psychiatry Clin Neurosci. 2010;64:514–519. doi: 10.1111/j.1440-1819.2010.02118.x. [DOI] [PubMed] [Google Scholar]
- Hughto JMW, Reisner SL, Pachankis JE. Transgender stigma and health: a critical review of stigma determinants, mechanisms, and interventions. Soc Sci Med. 2015;147:222–231. doi: 10.1016/j.socscimed.2015.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keuroghlian AS, Reisner SL, White JM, Weiss RD. Substance use and treatment of substance use disorders in a community sample of transgender adults. Drug Alcohol Depend. 2015;152:139–146. doi: 10.1016/j.drugalcdep.2015.04.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein A, Golub SA. Family rejection as a predictor of suicide attempts and substance misuse among transgender and gender nonconforming adults. LGBT Health. 2016;3:193–199. doi: 10.1089/lgbt.2015.0111. [DOI] [PubMed] [Google Scholar]
- Kopan T, Scott E. North Carolina governor signs controversial transgender bill. 2016 Available at: http://www.cnn.com/2016/03/23/politics/north-carolina-gender-bathrooms-bill/. Accessed 6/4/2016.
- Kuntsche E, Knibbe R, Gmel G, Engels R. Replication and validation of the Drinking Motive Questionnaire Revised (DMQ-R, Cooper, 1994) among adolescents in Switzerland. Eur Addict Res. 2006;12:161–168. doi: 10.1159/000092118. [DOI] [PubMed] [Google Scholar]
- Landers S. Civil rights and health–beyond same-sex marriage. New Engl J Med. 2015;373:1092–1093. doi: 10.1056/NEJMp1508488. [DOI] [PubMed] [Google Scholar]
- Lamis DA, Ballard ED, May AM, Dvorak RD. Depressive symptoms and suicidal ideation in college students: the mediating and moderating roles of hopelessness, alcohol problems, and social support. J Clin Psychol. 2016;72:919–932. doi: 10.1002/jclp.22295. [DOI] [PubMed] [Google Scholar]
- Lichtblau E, Fausset R. U.S. warns North Carolina that transgender bill violates civil rights laws. 2016 Available at: http://www.nytimes.com/2016/05/05/us/north-carolina-transgender-bathroom-bill.html?_r=0. Accessed 6/4/2016.
- Lovecchio CP, Wyatt TM, DeJong W. Reductions in drinking and alcohol-related harms reported by first-year college students taking an online alcohol education course: a randomized trial. J Health Commun. 2010;15:805–819. doi: 10.1080/10810730.2010.514032. [DOI] [PubMed] [Google Scholar]
- Markwiese BJ, Acheson SK, Levin ED, Wilson WA, Swartzwelder HS. Differential effects of ethanol on memory in adolescent and adult rats. Alcohol Clin Exp Res. 1998;22:416–421. [PubMed] [Google Scholar]
- Miller LR, Grollman EA. The social costs of gender nonconformity for transgender adults: implications for discrimination and health. Sociol Forum. 2015;30:809–831. doi: 10.1111/socf.12193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nolen-Hoeksema S. Gender differences in risk factors and consequences for alcohol use and problems. Clin Psychol Rev. 2004;24:981–1010. doi: 10.1016/j.cpr.2004.08.003. [DOI] [PubMed] [Google Scholar]
- Nguyen N, Walters ST, Rinker DV, Wyatt TM, DeJong W. Fake ID ownership in a US sample of incoming first-year college students. Addict Behav. 2011;36:759–761. doi: 10.1016/j.addbeh.2011.01.035. [DOI] [PubMed] [Google Scholar]
- Nguyen N, Walters ST, Wyatt TM, DeJong W. Do college drinkers learn from their mistakes? Effects of recent alcohol-related consequences on planned protective drinking strategies among college freshmen. Subst Use Misuse. 2013;48:1463–1468. doi: 10.3109/10826084.2013.778278. [DOI] [PubMed] [Google Scholar]
- Peacock E, Andrinopoulos K, Hembling J. Binge drinking among men who have sex with men and transgender women in San Salvador: correlates and sexual health implications. J Urban Health. 2015;92:701–716. doi: 10.1007/s11524-014-9930-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perkins HW. Surveying the damage: a review of research on consequences of alcohol misuse in college populations. (Supplement No 14).J Stud Alcohol. 2002:91–100. doi: 10.15288/jsas.2002.s14.91. [DOI] [PubMed] [Google Scholar]
- Rankin S, Beemyn G. Beyond a binary: the lives of gender-nonconforming youth. About Campus. 2012;17:2–10. [Google Scholar]
- Rehm J, Gmel G, Sempos CT, Trevisan M. Alcohol-related morbidity and mortality. Alcohol Res Health. 2002;27:39–51. [PMC free article] [PubMed] [Google Scholar]
- Reisner SL, Hughto JMW, Dunham EE, Heflin KJ, Begenyi JBG, Coffey-Esquivel J, Cahill S. Legal protections in public accommodations settings: a critical public health issue for transgender and gender-nonconforming people. Milbank Q. 2015a;93:484–515. doi: 10.1111/1468-0009.12127. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reisner SL, Vetters R, Leclerc M, Zaslow S, Wolfrum S, Shumer D, Mimiaga MJ. Mental health of transgender youth in care at an adolescent urban community health center: a matched retrospective cohort study. J Adolesc Health. 2015b;56:274–279. doi: 10.1016/j.jadohealth.2014.10.264. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Roberts TK, Fantz CR. Barriers to quality health care for the transgender population. Clin Biochem. 2014;47:983–987. doi: 10.1016/j.clinbiochem.2014.02.009. [DOI] [PubMed] [Google Scholar]
- Rowe C, Santos G-M, McFarland W, Wilson EC. Prevalence and correlates of substance use among trans*female youth ages 16–24 years in the San Francisco Bay Area. Drug Alcohol Depend. 2015;147:160–166. doi: 10.1016/j.drugalcdep.2014.11.023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Saraswat A, Weinand JD, Safer JD. Evidence supporting the biologic nature of gender identity. Endocr Pract. 2015;21:199–204. doi: 10.4158/EP14351.RA. [DOI] [PubMed] [Google Scholar]
- Scherer M. Battle of the bathroom. TIME Magazine. 2016;187:30–37. [Google Scholar]
- Schuster MA, Reisner SL, Onorato SE. Beyond bathrooms–Meeting the health needs of transgender people. New Engl J Med. 2016;375:101–103. doi: 10.1056/NEJMp1605912. [DOI] [PubMed] [Google Scholar]
- Shires DA, Jaffee K. Factors associated with health care discrimination experiences among a national sample of female-to-male transgender individuals. Health Soc Work. 2015;40:134–141. doi: 10.1093/hsw/hlv025. [DOI] [PubMed] [Google Scholar]
- Smalley KB, Warren JC, Barefoot KN. Differences in health risk behaviors across understudied LGBT subgroups. Health Psychol. 2016;35:103–114. doi: 10.1037/hea0000231. [DOI] [PubMed] [Google Scholar]
- Smith ES, Junger J, Derntl B, Habel U. The transsexual brain–-a review of findings on the neural basis of transsexualism. Neurosci Biobehav Rev. 2015;59:251–266. doi: 10.1016/j.neubiorev.2015.09.008. [DOI] [PubMed] [Google Scholar]
- Snapp SD, Russell ST, Arredondo M, Skiba R. A right to disclose: LGBTQ youth representation in data, science, and policy. Adv Child Dev Behav. 2016;50:135–159. doi: 10.1016/bs.acdb.2015.11.005. [DOI] [PubMed] [Google Scholar]
- Spear LP, Swartzwelder HS. Adolescent alcohol exposure and persistence of adolescent-typical phenotypes into adulthood: a mini-review. Neurosci Biobehav Rev. 2014;45:1–8. doi: 10.1016/j.neubiorev.2014.04.012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steensma TD, Kreukels BPC, de Vries ALC, Cohen-Kettenis PT. Gender identity development in adolescence. Horm Behav. 2013;64:288–297. doi: 10.1016/j.yhbeh.2013.02.020. [DOI] [PubMed] [Google Scholar]
- Stotzer RL. Violence against transgender people: a review of United States data. Aggr Violent Behav. 2009;14:170–179. [Google Scholar]
- Swartzwelder HS, Acheson SK, Miller KM, Sexton HG, Liu W, Crews FT, Risher M-L. Adolescent intermittent alcohol exposure: deficits in object recognition memory and forebrain cholinergic markers. PLOS ONE. 2015;10:e0140042. doi: 10.1371/journal.pone.0140042. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swartzwelder HS, Wilson WA, Tayyeb MI. Age-dependent inhibition of long-term potentiation by ethanol in immature versus mature hippocampus. Alcohol Clin Exp Res. 1995;19:1480–1485. doi: 10.1111/j.1530-0277.1995.tb01011.x. [DOI] [PubMed] [Google Scholar]
- Toomey RB, McGuire JK, Russell ST. Heteronormativity, school climates, and perceived safety for gender nonconforming peers. J Adolesc. 2012;35:187–196. doi: 10.1016/j.adolescence.2011.03.001. [DOI] [PubMed] [Google Scholar]
- White AM. What happened? Alcohol, memory blackouts, and the brain. Alcohol Res Health. 2003;27:186–196. [PMC free article] [PubMed] [Google Scholar]
- White AM, Jamieson-Drake DW, Swartzwelder HS. Prevalence and correlates of alcohol-induced blackouts among college students: results of an e-mail survey. J Am Coll Health. 2002;51:117–119. 122–131. doi: 10.1080/07448480209596339. [DOI] [PubMed] [Google Scholar]
- White AM, Kraus CL, McCracken LA, Swartzwelder HS. Do college students drink more than they think? Use of a free-pour paradigm to determine how college students define standard drinks. Alcohol Clin Exp Res. 2003;27:1750–1756. doi: 10.1097/01.ALC.0000095866.17973.AF. [DOI] [PubMed] [Google Scholar]
- White AM, Kraus CL, Swartzwelder H. Many college freshmen drink at levels far beyond the binge threshold. Alcohol Clin Exp Res. 2006;30:1006–1010. doi: 10.1111/j.1530-0277.2006.00122.x. [DOI] [PubMed] [Google Scholar]
- White AM, Signer ML, Kraus CL, Swartzwelder HS. Experiential aspects of alcohol-induced blackouts among college students. Am J Drug Alcohol Abuse. 2004;30:205–224. doi: 10.1081/ada-120029874. [DOI] [PubMed] [Google Scholar]
- White HR, Labouvie EW. Towards the assessment of adolescent problem drinking. J Stud Alcohol. 1989;50:30–37. doi: 10.15288/jsa.1989.50.30. [DOI] [PubMed] [Google Scholar]
- Wyatt TM, DeJong W, Dixon E. Population-level administration of AlcoholEdu for College: an ARIMA time-series analysis. J Health Commun. 2013;18:898–912. doi: 10.1080/10810730.2011.626501. [DOI] [PubMed] [Google Scholar]