

Abstract
Background:
Although anti-mullerian hormone (AMH) level is known to predict ovarian reserve, there is conflicting evidence regarding the association between AMH and clinical pregnancy or live birth (LB).
Aim:
Our aim is to establish if there is any association between AMH and LB considering the effects of age and other relevant confounding factors in predicting LB.
Settings and Design:
200 in-vitro fertilisation (IVF) cycles were retrospectively analysed in a tertiary fertility centre.
Materials and Methods:
From the database, data regarding the women’s age, AMH level, IVF/intracytoplasmic sperm injection, the factors of infertility, protocols, median AMH level and live birth rates (LBRs) were compared between the groups with and without LB in four age groups. The influences of age and AMH in predicting LB were analysed. Statistical analysis was performed using the Statistical Package for the Social Sciences version 21 software (SPSS Inc., Chicago, IL, United States).
Results and Conclusion:
There were no significant differences in any of the confounding factors analysed between the groups with and without LB. In the higher two age groups, median AMH levels in the group with LB were higher than that in the group without LB. The odds of having a LB was significantly higher in the younger three age groups, and when AMH level was >20 pmol/l. AMH was not found to be the IVF outcome defining factor in younger women, but was relevant in those above 35 years. Older women with significantly higher AMH level had significantly higher LBR than their peers with low AMH level. Thus AMH does have a role in counselling women when predicting live birth from IVF, although age of women plays a major role in determining success from IVF treatment.
KEYWORDS: Age, AMH, live birth
INTRODUCTION
There are numerous markers of ovarian reserve, which are used to prognosticate the chances of success with assisted reproductive techniques (ART), namely, serum follicle-stimulating hormone, oestradiol, inhibin B, anti-mullerian hormone (AMH), biophysical tests such as ovarian volume and peak stromal blood flow velocity and antral follicle count (AFC); all the markers apart from the AFC provide an indirect measurement of the cohort of antral follicles, which are the resting pool of the follicles ready to be recruited.[1]
AMH, a glycoprotein and a member of the transforming growth factor β family, is produced by the pre-antral and the small antral follicles in the ovary, is involved in folliculogenesis and supposed to reflect the number of primordial follicles[2,3,4] and also has good correlation with female age, AFC and ART outcome.[1,5,6,7] Therefore, it is regarded as the most precise biomarker of ovarian ageing and reserve.[3,8,9]
Current ovarian stimulation protocols during in-vitro fertilisation (IVF) treatments aim to individualise the protocols based on the women’s AMH level.[10,11,12]
There is good evidence regarding the positive correlation of AMH with egg reserve and oocyte yield following ovarian stimulation, both in cases of poor response and hyper-response.[3,9,13,14,15,16,17,18,19,20,21,22,23] However, there are conflicting reports regarding the association between AMH and clinical pregnancy.[24] Certain studies[25,26,27,28,29] have reported a positive association between AMH and clinical pregnancy, whereas other studies have refuted it.[13,30] A meta-analysis from 2013 demonstrated a weak association between AMH and clinical pregnancy.[15] There is conflicting evidence regarding the relationship between AMH, independent of age, and live birth (LB) as well; a few studies showed a positive association,[28,31,32] and others found no association.[33,34,35,36] A recent meta-analysis by Iliodromiti et al.[24] showed that AMH has a weak predictive value for LB in IVF. It is proposed that because AMH value reflects the size of the cohort of antral follicles, and not the quality of the oocytes, its predictive value of LB is weak.[1] The variation in the findings of the aforementioned studies could partly be explained by the diverse methodology of AMH testing and partly by the differences in study design, diverse patient populations and different stimulation protocols, which do not allow featuring the association between AMH and oocyte quality.[9,12]
One of the various technical limitations of comparing AMH levels in the different studies includes the numerous available forms of AMH assays. The original research assays were the Diagnostics Systems Lab (DSL) and Immunotech Beckman Coulter (IBC) assays, which use two different antibodies for AMH, with IBC assays yielding values higher than the other one.[4,37] Currently, Beckman Coulter has purchased the patents for all previous versions and established the AMH generation II assay,[10] which combines the cross-species DSL antibodies to the Immunotech ones,[37] but the AMH levels by the generation II assay were significantly lower than the DSL assay.[9,24] Nonetheless, when results from different laboratories using the same Beckman Gen II assay were compared, there was 40% variation in the AMH results.[12] Recently, a new AMH enzyme-linked immunosorbent assay has been developed, which is utilising different antibodies. In addition, inappropriate storage and sample handling can cause a dramatic rise in the AMH levels.[4,9,37]
In light of the heterogeneity in the results of the studies linking AMH level and the outcome of ART, we aimed to evaluate if AMH level, independent of age, in an unselected population, is a prognostic marker of LB following IVF treatment, wherein standard gonadotrophin-releasing hormone agonist and antagonist protocols are used, preceded by AMH test using a uniform standardised AMH assay.
Materials and Methods
All the fresh IVF/intracytoplasmic sperm injection (ICSI) cycles from January to June 2013 in a tertiary-assisted conception unit were retrospectively analysed and recorded from the electronic database and patient records.
AMH assay in this period was performed using the Beckman Coulter Generation II assay for all women. All the treatments used the down-regulation or antagonist protocols.
The data regarding the women’s age, AMH level, IVF/ICSI treatment, the factors of infertility, treatment protocols and IVF outcomes were compared using Mann–Whitney test or chi-squared test as suitable in the groups with and without LBs. Median AMH levels in the four age groups (group 1: 23–29 years, group 2: 30–34 years, group 3: 35–39 years and group 4: 40–45 years) were compared by Kruskal–Wallis test, and chi-squared test was performed to note any significant differences in the live birth rates (LBRs) across the groups. We also compared the AMH levels of women who had a LB versus that in women who were not successful in the four age groups. At the same time, we also looked at possible differences in IVF versus ICSI, the factors of infertility and treatment protocols in the different groups.
Multinomial logistic regression analysis was performed to evaluate the influence of age and AMH in predicting LB, following age and AMH stratification. AMH levels were categorised into five groups, namely, group 5: 0–5 pmol/l, group 4: >5–10 pmol/l, group 3: >10–20 pmol/l, group 2: >20–30 pmol/l and group 1: >30 pmol/l.
LBRs in women with the lowest AMH level (group 5) were separately analysed across the age groups.
Results
In this period, there were 226 fresh and frozen cycles, out of which 203 were fresh, and 23 were frozen embryo transfer (FET) cycles. Three of the 203 fresh cycles had all embryos frozen for ovarian hyperstimulation syndrome. A total of 151 women went through the 1st IVF cycle, of which 136 cycles were fresh and 15 were FET; 61 women went through the 2nd cycle, of which 53 cycles were fresh and eight were FET and 14 women in this period went through the 3rd IVF cycle, wherein all the cycles were fresh. The FET and the freeze all cycles were excluded from this analysis. Out of the 226 total fresh and frozen cycles, 200 fresh cycles (88.5%) had embryo transfers and were included in this analysis. All the 200 cycles had known outcomes of pregnancy/LB and had recent AMH levels estimated. 200 cycles with known AMH levels that were analysed in this time period resulted in 78 clinical pregnancies with a clinical pregnancy rate (CPR) of 39%, three ectopics, eight miscarriages and 67 LBs, with a LBR of 33.5%.
Table 1 describes the significant differences in median AMH value and LBRs across the age groups. Figure 1 demonstrates the median AMH level in the groups with and without LBs according to age stratification.
Table 1.
Comparison of the median AMH levels and live birth rates across the age groups

Figure 1.
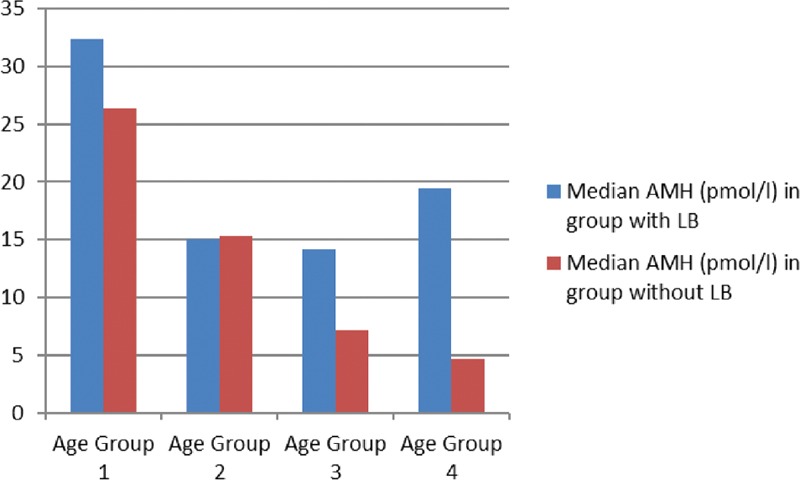
Comparison of AMH levels in women with and without live births in different age groups. The median AMH levels in the groups with and without live births according to age stratification
Table 2 shows that there were no significant differences in median age (35 years versus 37 years) between the groups with (group A) or without (group B) LBs. The median AMH level in group A was significantly higher than that in group B (18.7 versus 9.1 pmol/l). There were also no significant differences in the IVF versus ICSI treatments, factors responsible for infertility (P = 0.06) or in the treatment protocols used (P = 0.43) between the groups. There were 58 cycles using the long down-regulation protocol, 17 of which resulted in LBs, as opposed to 142 cycles using the gonadotrophin-releasing hormone antagonist protocol, of which 50 resulted in LBs. Chi-squared test showed that differences in the protocol did not make any significant differences to the LBRs (P = 0.43).
Table 2.
Comparison of the median age, AMH levels and the types of treatments between the groups with and without live births
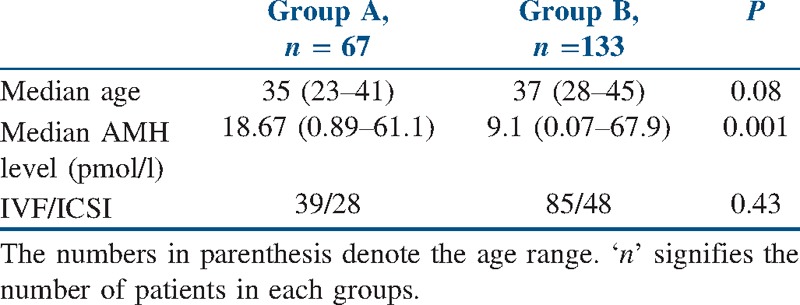
Table 3 shows the comparison of median AMH levels between the groups with and without LBs across the four age groups. When controlling for age, there were no significant differences in the factors of sub-fertility, IVF/ICSI treatment or protocols within the individual age groups and between the groups with and without LB. In the age groups 1 and 2, there was no significant difference in the median AMH level between the groups with or without LB. In the age group 3, the median AMH level in the group with LB was significantly higher than that in the group without LB (14.1 versus 7.2 pmol/l). In the age group 4, the group with LB had a higher median AMH level (19.5 versus 4.7 pmol/l) compared to the group without LB, albeit there was no statistical significance.
Table 3.
Comparison of the median AMH levels in the groups with and without LB, within the age groups

Evaluating the effect of AMH alone on LB, Pearson’s correlation analysis was performed, and it showed a correlation co-efficient of r = 0.23, indicating a modest positive effect of AMH alone on LB. Proceeding to multinomial logistic regression analysis using age and AMH level, the odds of having a LB was found to be significantly higher in the younger three age groups [odds ratio (OR) 22, 95% confidence interval (CI) 2.9–166.8; 3.7, 95% CI 0.96–14.3 and 4.8, 95% CI 1.3–17.5 in the age groups 1, 2 and 3, respectively] when compared to the age group 4. Controlling for age, AMH level >20 pmol/l was significantly associated with increased odds of having a LB (OR 5.1, 95% CI 1.6–16.3 in AMH group 2 and OR 2.9, 95% CI 1.02–8.5 in AMH group 1).
11/18 women in the age group 3 with AMH level >20 pmol/l had LB (LBR 61.1%), and 1/4 of the women in the age group 4 with AMH level >20 pmol/l had LB, that is, LBRs (LBR 25%) way higher than the average LB in those age groups (LBRs 34.3 and 10%, respectively). 55% of these women had ultrasound features of polycystic ovaries (PCO) but were not diagnosed as having polycystic ovarian syndrome (PCOS).
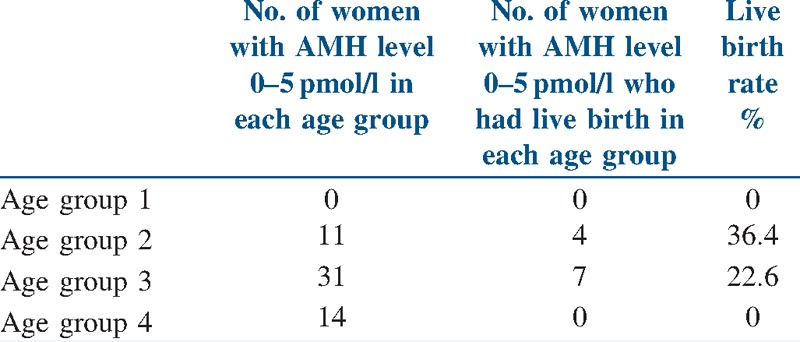
Table 4 shows the LBRs in women in the lowest AMH group (group 5) across all the age groups. It shows that LBR in women with AMH level 0–5 pmol/l in the age group 2 was comparable to the general LBR in this age group (36.4 % versus 35.1%; P = 0.9), and that in the age group 3, LBR was slightly lower than the general LBR in that age group (22.6% versus 34.3%; P = 0.09).
Table 4.
LBRs in women in the lowest AMH group across the age groups
DISCUSSION
This retrospective study aimed to evaluate if AMH level, independent of age, is a predictor of LB following ART, and took into consideration other potential confounders of the outcome of IVF such as factors for infertility, the types of treatment, that is, IVF or ICSI, and the protocols used for IVF. The major limitations identified in a recent meta-analysis, which were also identified in other similar studies evaluating AMH as a predictor of clinical pregnancy and implantation following ART,[9] were publication bias of the studies, different studies using different thresholds of AMH level and, above all, variability of the various AMH assays used in the different studies. The main strength of this analysis is that it was performed using data from an unselected patient population, wherein the current standard protocols of IVF were used along with a uniform validated AMH assay.
This study demonstrates, as expected, that there is a negative correlation between age and LB, as well as between age and AMH. In this analysis, the AMH levels and LBRs diminished remarkably from 40 years onwards. The odds of a LB in the age group of 23–39 years were significantly higher compared to that in the age group of 40–45 years.
Even though there was generally a modest positive correlation between AMH and LB, AMH per se had little influence in predicting LB in younger women under the age of 35 years, as shown in Table 3. This can be explained because younger women have generally oocytes of better quality that are associated with LBs, despite having low AMH level.
Median AMH level was higher in women with LBs in the age group above 35 years, in comparison to their peers without LB, although not reaching statistical significance in the 40–45 years group, because of the small numbers involved. When controlling for age, we found that higher AMH level (>20 pmol/l) was associated with significantly higher LBRs in older women. From our data, it suggests that AMH value over 20 pmol/l (Beckman Coulter Generation II assay) is a predictor of LB in women above the age of 35 years. It is possible that the AMH threshold level of 20 pmol/l predicting LB is related to the larger cohort of antral follicles in these women or higher AMH level being associated with better quality oocytes in comparison to other women in the same age group.
On the other hand, from these data, women under 40 years even with the lowest level of AMH (0–5 pmol/l) had good chances of having a LB, which was comparable to the rest of their peers in the 30–34-year-old group and was slightly diminished than the LBR in the rest of the 35–39-year-old population.
When comparing with previous studies, this study is in keeping with previous studies,[1,24,38] suggesting that LBR in IVF treatment diminishes with advancing age, with a sharp decline from the age of 40 years. AMH levels also negatively correlated with female age, as already known.[1,24,38] This is expected, because AMH represents the pool of oocytes remaining in the ovary,[4] and in a recent American Society of Reproductive Medicine (ASRM) committee opinion, it was concluded that AMH is a useful tool to predict ovarian reserve in the general IVF population, as well as for women at a risk of diminished ovarian reserve.[39] Indeed, AMH is undetectable in assays roughly 5 years prior to menopause,[37,40] and it is strikingly precise in predicting the onset of menopause.[41,42]
Our study showed that AMH on its own, independent of age, has limited predictive value for clinical pregnancy or LB in IVF, which is similar to a few reported studies.[29,43] Wang et al.[29] had shown that AMH and ART outcome are influenced by age, which is markedly different in the margins of reproductive age. We found that AMH level better predicts LB following IVF in older women and has limited predictive value in women <35 years. On the contrary, Brodin et al.[44] have found that AMH following controlling for age and number of oocytes has a strong association with pregnancy and LB. Some have explained the association between AMH and LB by the availability of greater number of oocytes and embryos, that is, the quantitative aspect, and not better egg or embryo quality,[45] whereas others have found a qualitative link between AMH and egg or embryo quality.[46,47] In a recent meta-analysis,[9] it was found that AMH had a weak association with CPRs in ART, but had considerable predictive accuracy in poor ovarian reserve cases. Similarly, Iliodromiti et al.[24] have found in their meta-analysis of 6306 women that AMH has some role in predicting LB after IVF, but the predictive accuracy is poor (OR 2.48), but a better (OR 4.63), still small predictive effect in women with low ovarian reserve.
Previous researchers have propounded that age-dependent predictability of AMH is possibly related to the age-related decline in oocyte quality and quantity.[48] It has been proposed that in younger women, the cohort of oocytes are genetically competent and of good quality, and hence, their ovarian reserve is not the limiting factor in dictating LB in IVF treatment. On the contrary, in older women with diminishing ovarian reserve, good quality eggs constitute a small proportion of their oocytes. Resultantly, a greater ovarian reserve reflected by a higher AMH level would enable a good oocyte yield to select the best eggs and embryos to improve the chances of LB in IVF.
There is robust evidence to confirm that PCOS is associated with a significantly high-serum AMH value, and several studies are suggesting diagnostic values of AMH to be set for PCOS.[12] Women with clinical symptoms of PCOS are known to have adverse outcomes to ART, including compromised oocyte quality, despite having a good number of follicles, poor quality of embryos and higher miscarriage rates.[7] On the contrary, women with morphological features of PCO in ultrasound scan (USS) but no evidence of clinical PCOS are known to have higher number of oocytes, embryos and higher cumulative pregnancy rates, but similar miscarriage rates suggesting comparable oocyte quality in comparison to women with normal ovaries having IVF.[7,49,50] It has been proposed that the higher density of primary follicles in PCO suggests that these women were born with larger ovarian reserve,[7,51] which has an accelerated entry into the early growing stages, followed by a slower growth through the pre-antral stages. In our experience, the women over 35 years of age with an AMH level higher than 20 pmol/l had significantly higher LBRs in comparison to the average LB rates for their age groups. More than half of these women were found to have morphological features of PCO on USS only, but were not diagnosed with PCOS. Recently, a consensus opinion from ASRM and European Society of Human Reproduction and Endocrinology (ESHRE) stated that ‘ovarian reserve testing has moderate accuracy in predicting quantitative responses but low accuracy for qualitative predictions, unless very high thresholds are used’.[39]
Accepting the inherent limitation of a retrospective study, we admit that we have not been able to control for all possible potential confounding factors known to influence LB in IVF such as genetic integrity of sperm and eggs, embryo quality and endometrial receptivity.[52] This study showed that AMH on its own had limited predictive value for determining LB after IVF; it was not found to be the IVF outcome defining factor in younger women, but it was of importance in the population above 35 years. When controlling for age, we found that older women with significantly higher AMH level had significantly higher LBR than the same-aged women with low AMH level. Thus AMH does have a role in counselling women when predicting live birth from IVF, although age of women plays a major role in determining success from IVF treatment.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We acknowledge the help of Dr. Debasis Majumdar for help with the statistical analysis of the data. We are grateful to all our patients without whom this study would not have been possible.
REFERENCES
- 1.Nikolaou D. How old are your eggs? Curr Opin Obstet Gynecol. 2008;20:540–4. doi: 10.1097/GCO.0b013e328317c755. [DOI] [PubMed] [Google Scholar]
- 2.Pellatt L, Rice S, Mason HD. Anti-Mullerian hormone and polycystic ovary syndrome: A mountain too high? Reproduction. 2010;139:825–33. doi: 10.1530/REP-09-0415. [DOI] [PubMed] [Google Scholar]
- 3.Seifer DB, Maclaughlin DT. Mullerian inhibiting substance is an ovarian growth factor of emerging clinical significance. Fertil Steril. 2007;88:539–46. doi: 10.1016/j.fertnstert.2007.02.014. [DOI] [PubMed] [Google Scholar]
- 4.Tobler KJ, Shoham G, Christianson MS, Zhao Y, Leong M, Shoham Z. Use of anti-mullerian hormone for testing ovarian reserve: A survey of 796 infertility clinics worldwide. J Assist Reprod Genet. 2015;32:1441–8. doi: 10.1007/s10815-015-0562-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.De Vet A, Laven J, de Jong F, Themmen A, Fauser B. Antimullerian hormone serum levels: A putative marker for ovarian aging. Fertil Steril. 2002;77:357–62. doi: 10.1016/s0015-0282(01)02993-4. [DOI] [PubMed] [Google Scholar]
- 6.Fanchin R, Schonauer L, Righini C, Guibourdenche J, Frydman R, Taieb J. Serum anti-Mullerian hormone is more strongly related to ovarian follicular status than serum inhibin-B, estradiol, FSH and LH on day 3. Hum Reprod. 2003;18:323–7. doi: 10.1093/humrep/deg042. [DOI] [PubMed] [Google Scholar]
- 7.Nikolaou D, Gilling-Smith C. Early ovarian ageing: Are women with polycystic ovaries protected? Debate − Continued. Hum Reprod. 2004;19:2175–9. doi: 10.1093/humrep/deh419. [DOI] [PubMed] [Google Scholar]
- 8.Nelson SM, Anderson RA, Broekmans FJ, Raine-Fenning N, Fleming R, La Marca A. Anti-Mullerian hormone: Clairvoyance or crystal clear? Hum Reprod. 2012;27:631–6. doi: 10.1093/humrep/der446. [DOI] [PubMed] [Google Scholar]
- 9.Tal R, Tal O, Seifer BJ, Seifer DB. Antimullerian hormone as predictor of implantation and clinical pregnancy after assisted conception: A systematic review and meta-analysis. Fertil Steril. 2015;103:119–30. doi: 10.1016/j.fertnstert.2014.09.041. [DOI] [PubMed] [Google Scholar]
- 10.La Marca A, Sunkara SK. Individualization of controlled ovarian stimulation in IVF using ovarian reserve markers: From theory to practice. Hum Reprod Update. 2014;20:124–40. doi: 10.1093/humupd/dmt037. [DOI] [PubMed] [Google Scholar]
- 11.Lan VT, Linh NK, Tuong HM, Wong PC, Howles CM. Anti-mullerian hormone versus antral follicle count for defining the starting dose of FSH. Reprod Biomed Online. 2013;27:390–9. doi: 10.1016/j.rbmo.2013.07.008. [DOI] [PubMed] [Google Scholar]
- 12.Leader B, Baker VL. Maximizing the clinical utility of antimüllerian hormone testing in women’s health. Curr Opin Obstet Gynecol. 2014;26:226–36. doi: 10.1097/GCO.0000000000000087. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Broekmans FJ, Kwee J, Hendriks DJ, Mol BW, Lambalk CB. A systematic review of tests predicting ovarian reserve and IVF outcome. Hum Reprod Update. 2006;12:685–718. doi: 10.1093/humupd/dml034. [DOI] [PubMed] [Google Scholar]
- 14.Broekmans FJ, Scheffer GJ, Bancsi LF, Dorland M, Blankenstein MA, te Velde ER. Ovarian reserve tests in infertility practice and normal fertile women. Maturitas. 1998;30:205–14. doi: 10.1016/s0378-5122(98)00075-9. [DOI] [PubMed] [Google Scholar]
- 15.Broer SL, van Disseldorp J, Broeze KA, Dolleman M, Opmeer BC, Bossuyt P, et al. IMPORT Study Group. Added value of ovarian reserve testing on patient characteristics in the prediction of ovarian response and ongoing pregnancy: An individual patient data approach. Hum Reprod Update. 2013;19:26–36. doi: 10.1093/humupd/dms041. [DOI] [PubMed] [Google Scholar]
- 16.Broer SL, Dolleman M, Opmeer BC, Fauser BC, Mol BW, Broekmans FJ. AMH and AFC as predictors of excessive response in controlled ovarian hyperstimulation: A meta-analysis. Hum Reprod Update. 2011;17:46–54. doi: 10.1093/humupd/dmq034. [DOI] [PubMed] [Google Scholar]
- 17.Broer SL, Mol BW, Hendriks D, Broekmans FJ. The role of antimullerian hormone in prediction of outcome after IVF: Comparison with the antral follicle count. Fertil Steril. 2009;91:705–14. doi: 10.1016/j.fertnstert.2007.12.013. [DOI] [PubMed] [Google Scholar]
- 18.Coccia ME, Rizzello F. Ovarian reserve. Ann N Y Acad Sci. 2008;1127:27–30. doi: 10.1196/annals.1434.011. [DOI] [PubMed] [Google Scholar]
- 19.Haadema ML, Groen H, Fidler V, Seinen LH, Broekmans FJ, Heineman MJ, et al. The predictive value of ovarian reserve tests for spontaneous pregnancy in subfertile ovulatory women. Hum Reprod. 2008;23:1800–7. doi: 10.1093/humrep/den234. [DOI] [PubMed] [Google Scholar]
- 20.La Marca A, Sighinolfi G, Radi D, Argento C, Baraldi E, Artenisio AC, et al. Anti-Mullerian hormone (AMH) as a predictive marker in assisted reproductive technology (ART) Hum Reprod Update. 2010;16:113–30. doi: 10.1093/humupd/dmp036. [DOI] [PubMed] [Google Scholar]
- 21.Verhagen TE, Hendriks DJ, Bancsi LF, Mol BW, Broekmans FJ. The accuracy of multivariate models predicting ovarian reserve and pregnancy after in vitro fertilization: A meta-analysis. Hum Reprod Update. 2008;14:95–100. doi: 10.1093/humupd/dmn001. [DOI] [PubMed] [Google Scholar]
- 22.Maheshwari A, Bhattacharya S, Johnson NP. Predicting fertility. Hum Fertil. 2008;11:109–17. doi: 10.1080/14647270701832346. [DOI] [PubMed] [Google Scholar]
- 23.Maheshwari A, Fowler P, Bhattacharya S. Assessment of ovarian reserve − Should we perform tests of ovarian reserve routinely? Hum Reprod. 2006;21:2729–35. doi: 10.1093/humrep/del188. [DOI] [PubMed] [Google Scholar]
- 24.Iliodromiti S, Kelsey TW, Wu O, Anderson RA, Nelson SM. The predictive accuracy of anti-Müllerian hormone for live birth after assisted conception: A systematic review and meta-analysis of the literature. Hum Reprod Update. 2014;20:560–70. doi: 10.1093/humupd/dmu003. [DOI] [PubMed] [Google Scholar]
- 25.Hazout A, Bouchard P, Seifer DB, Aussage P, Junca AM, Cohen-Bacrie P. Serum antimullerian hormone/mullerian-inhibiting substance appears to be a more discriminatory marker of assisted reproductive technology outcome than follicle-stimulating hormone, inhibin B, or estradiol. Fertil Steril. 2004;82:1323–9. doi: 10.1016/j.fertnstert.2004.03.061. [DOI] [PubMed] [Google Scholar]
- 26.Honnma H, Baba T, Sasaki M, Hashiba Y, Oguri H, Fukunaga T, et al. Serum anti-Mullerian hormone levels affect the rate of ongoing pregnancy after in vitro fertilization. Reprod Sci. 2013;20:51–9. doi: 10.1177/1933719112450329. [DOI] [PubMed] [Google Scholar]
- 27.Kwee J, Schats R, McDonnell J, Themmen A, de Jong F, Lambalk C. Evaluation of anti-Mullerian hormone as a test for the prediction of ovarian reserve. Fertil Steril. 2008;90:737–43. doi: 10.1016/j.fertnstert.2007.07.1293. [DOI] [PubMed] [Google Scholar]
- 28.Nelson SM, Yates RW, Fleming R. Serum anti-Mullerian hormone and FSH: Prediction of live birth and extremes of response in stimulated cycles − Implications for individualization of therapy. Hum Reprod. 2007;22:2414–21. doi: 10.1093/humrep/dem204. [DOI] [PubMed] [Google Scholar]
- 29.Wang JG, Douglas NC, Nakhuda GS, Choi JM, Park SJ, Thornton MH, et al. The association between anti-Mullerian hormone and IVF pregnancy outcomes is influenced by age. Reprod Biomed Online. 2010;21:757–61. doi: 10.1016/j.rbmo.2010.06.041. [DOI] [PubMed] [Google Scholar]
- 30.van Rooij IA, Broekmans FJ, Hunault CC, Scheffer GJ, Eijkemans MJ, de Jong FH, et al. Use of ovarian reserve tests for the prediction of ongoing pregnancy in couples with unexplained or mild male infertility. Reprod Biomed Online. 2006;12:182–90. doi: 10.1016/s1472-6483(10)60859-0. [DOI] [PubMed] [Google Scholar]
- 31.Eldar-Geva T, Ben-Chetrit A, Spitz IM, Rabinowitz R, Markowitz E, Mimoni T, et al. Dynamic assays of inhibin B, anti-Mullerian hormone and estradiol following FSH stimulation and ovarian ultrasonography as predictors of IVF outcome. Hum Reprod. 2005;20:3178–83. doi: 10.1093/humrep/dei203. [DOI] [PubMed] [Google Scholar]
- 32.Silberstein T, MacLaughlin DT, Shai I, Trimarchi JR, Lambert-Messerlian G, Seifer DB, et al. Mullerian inhibiting substance levels at the time of HCG administration in IVF cycles predict both ovarian reserve and embryo morphology. Hum Reprod. 2006;21:159–63. doi: 10.1093/humrep/dei270. [DOI] [PubMed] [Google Scholar]
- 33.Fanchin R, Mendez Lozano DH, Frydman N, Gougeon A, di Clemente N, Frydman R, et al. Anti-Mullerian hormone concentrations in the follicular fluid of the preovulatory follicle are predictive of the implantation potential of the ensuing embryo obtained by in vitro fertilization. J Clin Endocrinol Metab. 2007;92:1796–802. doi: 10.1210/jc.2006-1053. [DOI] [PubMed] [Google Scholar]
- 34.Ficicioglu C, Kutlu T, Bagla E, Bakacak Z. Early follicular antimullerian hormone as an indicator of ovarian reserve. Fertil Steril. 2006;85:592–6. doi: 10.1016/j.fertnstert.2005.09.019. [DOI] [PubMed] [Google Scholar]
- 35.Peñarrubia J, Fábregues F, Manau D, Creus M, Casals G, Casamitjana R, et al. Basal and stimulation day 5 anti-Mullerian hormone serum concentrations as predictors of ovarian response and pregnancy in assisted reproductive technology cycles stimulated with gonadotropin-releasing hormone agonist − Gonadotropin treatment. Hum Reprod. 2005;20:915–22. doi: 10.1093/humrep/deh718. [DOI] [PubMed] [Google Scholar]
- 36.Smeenk JM, Sweep FC, Zielhuis GA, Kremer JA, Thomas CM, Braat DD. Antimullerian hormone predicts ovarian responsiveness, but not embryo quality or pregnancy, after in vitro fertilization or intracytoplasmic sperm injection. Fertil Steril. 2007;87:223–6. doi: 10.1016/j.fertnstert.2006.06.019. [DOI] [PubMed] [Google Scholar]
- 37.Nelson SM. Biomarkers of ovarian response: current and future applications. Fertil Steril. 2013;99:963–9. doi: 10.1016/j.fertnstert.2012.11.051. [DOI] [PubMed] [Google Scholar]
- 38.Nikolaou D. Early ovarian ageing. In: Luesley DN, Baker PN, editors. Obstetrics and Gynaecology an Evidence Based Text for MRCOG. London: Edward Arnold Publishers Limited; 2010. pp. 657–67. Chapter 58. [Google Scholar]
- 39.Gianaroli L, Racowski C, Geraedts J, Cedars M, Makrigiannakis A, Lobo RA. Best practices of ASRM and ESHRE: A journey through reproductive medicine. Fertil Steril. 2012;98:1380–94. doi: 10.1016/j.fertnstert.2012.07.1164. [DOI] [PubMed] [Google Scholar]
- 40.Sowers MR, Eyvazzadeh AD, McConnell D, Yosef M, Jannausch ML, Zhang D, et al. Anti-müllerian hormone and inhibin B in the definition of ovarian aging and the menopause transition. J Clin Endocrinol Metab. 2008;93:3478–83. doi: 10.1210/jc.2008-0567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Tehrani FR, Solaymani-Dodaran M, Azizi F. A single test of antimullerian hormone in late reproductive-aged women is a good predictor of menopause. Menopause. 2009;16:797–802. doi: 10.1097/gme.0b013e318193e95d. [DOI] [PubMed] [Google Scholar]
- 42.van Rooij IA, Tonkelaar I, Broekmans FJ, Looman CW, Scheffer GJ, de Jong FH, et al. Anti-mullerian hormone is a promising predictor for the occurrence of the menopausal transition. Menopause. 2004;11:601–6. doi: 10.1097/01.gme.0000123642.76105.6e. [DOI] [PubMed] [Google Scholar]
- 43.Tal R, Seifer DB, Khanimov M, Schwartz E, Grazi RV, Malter HE. Anti-Mullerian hormone as an independent predictor of twin versus singleton pregnancy in fresh cycles. Reprod Biomed Online. 2013;26:360–7. doi: 10.1016/j.rbmo.2012.12.002. [DOI] [PubMed] [Google Scholar]
- 44.Brodin T, Hadziosmanovic N, Berglund L, Olovsson M, Holte J. Antimullerian hormone levels are strongly associated with live-birth rates after assisted reproduction. J Clin Endocrinol Metab. 2013;98:1107–14. doi: 10.1210/jc.2012-3676. [DOI] [PubMed] [Google Scholar]
- 45.Arce JC, La Marca A, Mirner Klein B, Nyboe Andersen A, Fleming R. Antimullerian hormone in gonadotropin releasing-hormone antagonist cycles: Prediction of ovarian response and cumulative treatment outcome in good-prognosis patients. Fertil Steril. 2013;99:1644–53. doi: 10.1016/j.fertnstert.2012.12.048. [DOI] [PubMed] [Google Scholar]
- 46.Lin WQ, Yao LN, Zhang DX, Zhang W, Yang XJ, Yu R. The predictive value of anti-Mullerian hormone on embryo quality, blastocyst development, and pregnancy rate following in vitro fertilization-embryo transfer (IVF-ET) J Assist Reprod Genet. 2013;30:649–55. doi: 10.1007/s10815-013-9973-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Majumder K, Gelbaya TA, Laing I, Nardo LG. The use of anti-Mullerian hormone and antral follicle count to predict the potential of oocytes and embryos. Eur J Obstet Gynecol Reprod Biol. 2010;150:166–70. doi: 10.1016/j.ejogrb.2010.02.029. [DOI] [PubMed] [Google Scholar]
- 48.Nelson SM, Telfer EE, Anderson RA. The ageing ovary and uterus: new biological insights. Hum Reprod Update. 2013;19:67–83. doi: 10.1093/humupd/dms043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Engmann L, Maconochie N, Sladkevicius P, Bekir J, Campbell S, Tan SL. The outcome of in-vitro fertilization treatment in women with sonographic evidence of polycystic ovarian morphology. Hum Reprod. 1999;14:167–71. doi: 10.1093/humrep/14.1.167. [DOI] [PubMed] [Google Scholar]
- 50.Nikolaou D, Lavery S, Trew G. What is the significance of polycystic ovarian morphology, in the absence of clinical symptoms, for the outcome of IVF? Hum Fertil. 2002;5:159–60. [Google Scholar]
- 51.Webber L, Stubbs S, Stark J, Trew G, Margara R, Hardy K, et al. Formation and early development of follicles in the polycystic ovary. Lancet. 2003;362:1017–21. doi: 10.1016/s0140-6736(03)14410-8. [DOI] [PubMed] [Google Scholar]
- 52.Boomsma CM, Macklon NS. What can the clinician do to improve implantation? Reprod Biomed Online. 2006;13:845–55. doi: 10.1016/s1472-6483(10)61034-6. [DOI] [PubMed] [Google Scholar]