

Abstract
Analysis of world record performances by master athletes suggests an essentially linear decline with age until around the eighth decade after which performance decline accelerates. Because these records are obtained from highly trained individuals they can be viewed as being reflective of the diminution of integrative physiological prowess that occurs solely as a result of ageing, unaffected by the confounding effects of inactivity. It can also be argued that these performance profiles mirror and provide an insight into the trajectory of the physiology of the human ageing process. Here we propose a set point theory that hypothesises that a given threshold of physical activity is needed to age optimally and to maximise the ‘healthspan’. Exercising at levels below the set point will result in ageing being contaminated by the unpredictable and pathological effects of inactivity. Exercise above this threshold stimulates adaptations towards maximising athletic performance, but is unlikely to have further beneficial effects on health. Thus the decades‐long, controlled diminution in athletic performance, should not be seen as a disease process. The ageing process is separate from, and independent of, exercise‐mediated processes that maintain or adapt physiological function. Whether an understanding of these mechanisms will also help uncover mechanisms underpinning the ageing process itself is open to question. However, any model which does not take into account the effects of activity will not adequately describe the inherent ageing process.

Keywords: ageing, exercise physiology, health, performance, physical activity
Introduction
The necessity to be physically active and partake in exercise in order to be healthy throughout the life course is now well established (Booth et al. 2012) and it has been suggested by many that exercise should now be incorporated into the armamentarium of medical treatments (Booth et al. 2012; Hallal & Lee, 2013; Pedersen & Saltin, 2015). Indeed, while population demographics clearly show an increase in lifespan, for many this is not being accompanied by equivalent years of good health or concomitantly increased ‘healthspan’ (Pierce, 2012). An objective of ageing research is not to increase lifespan per se, but to increase the ‘healthspan’ and to compress morbidity in later life (Fries, 1980; Seals et al. 2016). On a population level, ageing has long been associated with an increase in sedentary behaviour (Bouchard et al. 1994), but it is clear that a wide continuum of activity levels exists among older people. This spectrum ranges from the very sedentary, as evidenced by prolonged periods of sitting – itself an independent risk factor for all‐cause mortality (Bouchard et al. 2015), through to individuals who maintain very high levels of exercise training and are still competitive athletes. Athletes over 35–40 years of age are usually referred to as ‘master’, ‘veteran’ or ‘senior’ athletes and regional, national and world championship events exist which cater for the full range of athletic disciplines and exercise types (track and field, cycling, weightlifting, swimming, etc.). Aside from their remarkable athletic performances, from a gerontological perspective, master athletes have been proposed as being a biological model in which an understanding of the physiology of the healthy and inherent human ageing process can be gleaned (Hawkins et al. 2003; Tanaka & Seals, 2003; Lazarus & Harridge, 2007).
This short review discusses the contention that the trajectory of decline in athletic performance reflects the characteristics of decline in integrative physiological function that occurs as a result of an optimal and inherent ageing process. It integrates this concept into a set point hypothesis that aims to describe how exercise, health and ageing are interlinked.
Performance and world records
Performance in athletic competitions is arguably the greatest test of physiological integration, where cardiovascular, respiratory, neuromuscular as well as cognitive systems, to name but a few, must all be coherent (Basset & Hawley, 2000). Indeed, A. V. Hill (1925) famously noted that much could be learned about human physiology ‘from the analysis of athletic records and racing’, an observation that can also be applied to the study of the physiology of human ageing. In recent years, world records of master athletes have been the subject of detailed study (Meltzer, 1994; Tanaka & Seals, 2003; Rittwigger et al. 2009; Baker & Tang, 2010). Figure 1 shows one example of the trajectory of decline with age in the current world record performances in two athletic disciplines – high‐power short‐duration sprinting (100 m) and endurance running (10,000 m). In both events an essentially linear increase is followed by an exponential rise in performance times after the seventh to eighth decade. It may be that this accelerated decline (sometimes referred to as a ‘breakpoint’) is simply due to a reduction in the pool of older competitors. Alternatively, it may reflect a diminution in the amount and intensity of training (Tanaka & Seals, 2008), or more intriguingly it may reflect the trajectory of a fading integrative physiological capacity even though training levels may remain appropriate for age.
Figure 1. World record performances for the 100 m and 10,000 m track event as of June 2016 for both male and female master athletes.
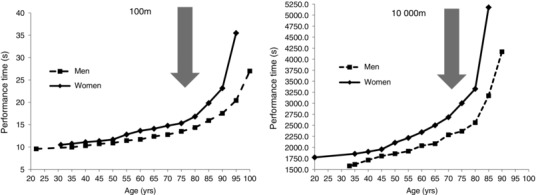
The data are from each age category group (5 year increments) from age 35 and also include the current world record performances by non‐master athletes. (Data from www.world‐masters‐athletics.org.) The arrows indicate the accelerated increased in performance times around the eighth decade.
These, like many studies of the relationship between age and physiological function, are cross‐sectional in nature and with a few exceptions (e.g. Hawkins et al. 2001), it is not possible to chart the decline in performance that occurs with ageing in a given individual. Furthermore, distinctions need to be made between exercisers and athletes (Araújo & Scharhag, 2016), as well between elite athletes and elite ‘master’ athletes. The past histories of master athletes are usually unspecified and the alumni of master world record holders rarely contain athletes who were world record holders in their prime.
Despite the deficiencies in cross‐sectional data there are nonetheless some interesting conclusions that can be drawn from studying the relationship between performance decline and age. What is especially striking is that, as mentioned above, the falloff in performance is not linear, but curvilinear (Baker & Tang, 2010) and with some exceptions (Senefield et al. 2016), is generally similar for both men and women (Wiswell et al. 2001). Tanaka & Seals (2008) suggested that declines with increasing age in endurance exercise performance and its physiological determinants, such as maximal oxygen uptake (), appear to be mediated in large part by a reduction in the absolute intensity and total volume of training undertaken. This implies that should the older athletes simply increase their training load then performance would increase. This raises an important issue as to the maximum intensity and volume of training of which an older athlete is capable. Indeed, it could be argued that older athletes, particularly at the elite level, are already training at the maximum capability that their age dictates or allows. Thus, despite training at reduced absolute levels of intensity and volume, they may well be training at the same relative level, normalised in some way for the ageing process. Until data from longitudinal studies are obtained which determine the relationship between advancing age and training load that are appropriate for the age under study this question remains open. In contrast to endurance events, power based activities such as 100 m sprint running (Fig. 1 B) are not limited by cardio‐respiratory fitness, but essentially by neuromuscular/muscular–tendinous function (Kohanen et al. 2009). Here a similar ageing profile is seen for the age‐related declines in world record performances. Whilst these individuals have training regimens which specifically target power generation and sprint running speed, the data suggest that, as for other systems, this decline reflects an inherent ageing effect. Importantly, whilst these two examples are from running, the decline in performance with age is essentially the same among many athletic disciplines (Baker & Tang, 2010), providing support for the notion that these curves reflect a profile of inherent age‐related changes in integrative physiological function that is broadly applicable.
On examining the performance curves there are a number of points which the above observations do not address. Master athletes, by exercising, although not completely free of disease, have avoided most of the negative effects brought on by inactivity and therefore it is suggested that these curves represent optimal declinations in performance that are driven largely by an inherent ageing process. If so, these curves might suggest that the ageing process results in a smooth, coordinated and synchronous reduction in physiological systems enabling the body to achieve maximum performance for a given age. When considered in this light it is worth noting how remarkable the performances of the oldest master athletes are relative to their age‐matched sedentary individuals, who are often frail with multiple morbidities. These observations also suggest that this seemingly age‐coordinated diminution of physiological function during healthy ageing has little resemblance to a disease process.
Physically active/exercising individuals represent the optimum phenotype for ageing studies because they should be free from the negative effects of inactivity (Lazarus & Harridge, 2010). However, it is clear that exercise does not halt the ageing process, even though superior levels of function are achieved by the most active for a given age. There are two distinct processes that need addressing; the first is the unfolding of the mechanisms by which exercise acts as a stimulus to maintain health and the second is the elucidation of the mechanisms of the ageing process driving changes in physiological function. As being physically active is key to health, it is unfortunate that in most studies of human ageing, which do not involve athletes, the exercise and/or physical activity profiles of the subjects are not accorded the same importance as other lifestyle factors. The result is that it becomes difficult to unravel the effects of ageing from those induced by inactivity mediated processes. We emphasise that during this healthy ageing process exercise is not the only influential factor. Other lifestyle factors such as appropriate diet, lack of smoking and no, or moderate, alcohol consumption must also be in place.
Some of the reasons for this lack of a clear definition include the collection of self‐reported activity data, the failure to objectively assess duration, intensity and frequency, as well as the different types of activities. Unless and until objective measurements of physical activity are incorporated into protocols examining the ageing process in healthy individuals of all ages, incorrect perceptions of the ageing process will persist.
The nexus between exercise, health and ageing
From an overview of the above limited longitudinal and extensive cross‐sectional data and despite the many caveats using cross‐sectional data for model building, we put forward the following set point hypothesis. This model seeks to explain and predict some of the effects that are the product of an interaction between physical activity/exercise, age and health. It has been cogently argued that exercise is integrated into human physiology as part of our evolutionary heritage (Booth et al. 2002). The set point hypothesis predicts how health, age and exercise are interlinked. Health here is defined as the state in which sufficient physical activity/exercise is undertaken in order to maintain physiological function uncontaminated by inactivity. Essentially the negative effects of inactivity are mostly eliminated. The set point might be attained via different combinations of volume and intensity of physical activity/exercise as well as mode. There are three important physiological scenarios in which to apply the Set Point Model. The first is an examination of the physiological and ageing effects of individuals engaging in physical activity at the set point level. The second are effects on individuals operating below set point levels and the third are those individuals who engage in exercise regimens, in which the amount of exercise is above set point levels, the category in which master athletes will fall.
Individuals operating at set point levels of physical activity
Given the heterogeneity of human physiology, the set point will not be the same for all individuals. Longitudinal studies are required to determine whether, or the extent to which, the set point is genetically determined, or is a product of other factors including the physiognomy of an individual. Populations or individuals with inherently lower set points would be able to preserve health at lower levels of physical activity compared to those with higher set points. Unlike master athletes, individuals exercising at the set point will probably not engage in competitive events. The effects of operating at the set point are depicted in Fig. 2 A. Because of the elimination of inactivity, the decline in function is not compromised and only governed by the inherent ageing process. The effect of this process is for physiological capacity to ‘shrink’ in a co‐ordinated and controlled manner so that health is preserved through the decades and as a result, the set point to offset physical inactivity‐mediated pathologies on a shrinking physiology also decreases. At advanced age inherent physiological differences between subjects will probably have been minimised and physical activity levels to maintain healthspan are likely to be within a narrow range (Fig. 2 A). Because of the compression of the set point, reflecting the reduced absolute level and range of physical activity necessary to maintain health, healthy older individuals (e.g. ∼80 years) could be suggested as the most appropriate group in whom to try and begin to define set point levels.
Figure 2. The set point theory of healthy human ageing.
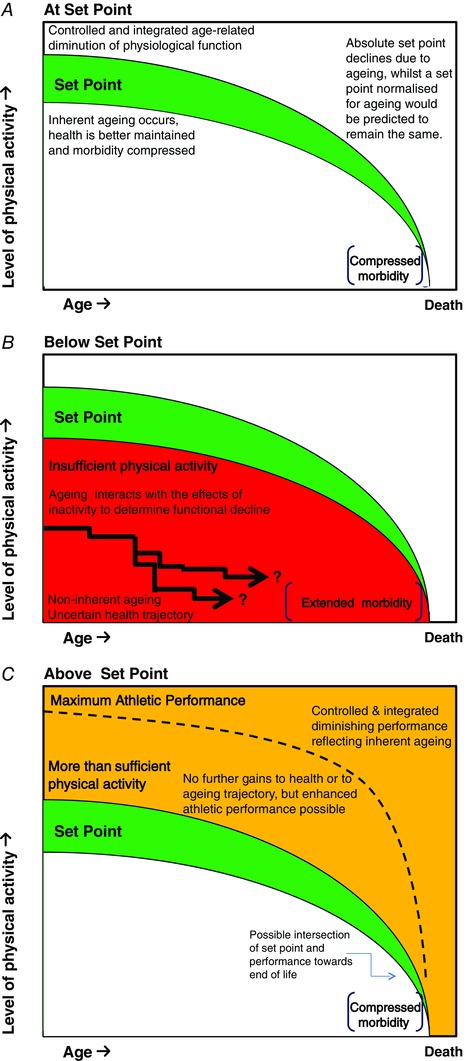
A, at the set point, physical activity/exercise is sufficient to counteract the effects of inactivity and health is optimised. The decrement in physiological function that occurs through the decades is governed by the inherent ageing process. Because the decrement in physiology generated by the inherent ageing process is co‐ordinated and integrated, the amount of physical activity necessary to counter inactivity also concomitantly decreases. Health is still maintained, but at a lower physical activity level. This intertwined relationship between health and the amount of physical activity necessary to counter inactivity applies throughout the ‘healthspan’ and morbidity is compressed. The green shaded area depicts the heterogeneity of set points that could be expected in the general population. B, below the set point the negative and unpredictable effects of inactivity on physiological systems may not be perceived in the early ages, but as age progresses the added decremental effect of the inherent ageing process on an increasingly compromised physiology will result in one or more systems showing clinical disease with extended morbidity. C, individuals who engage in exercise above the set point level will also have countered the effects of inactivity and be inherently ageing. Master athletes will represent a group that are probably exercising at levels of exercise that are maximal. When engaged in competitive events the traditional performance curve will be produced. The decrement in the performance curve as age advances is due to the inherent ageing process. Analogous to the influence of the inherent ageing process at set point, the ageing process reduces performance mechanisms that are both co‐ordinated and integrated to deliver maximum performance for a given age. In later life, where the decline in performance accelerates, the levels of exercise needed to preserve maximum performance may now be approaching the set point level for that age. Individuals exercising below maximal levels, but above the set point are hypothesised to generate performance curves of a similar shape, but at lower absolute performance levels and dependent on the degree of exercise training.
In the very late decades the amount of physical activity required to combat the effects of inactivity may not be readily apparent without objective measurements. Eventually a critical level of physiological decline is reached as death approaches, but healthspan is maximised and morbidity compressed. Importantly, and as previously emphasised, during this healthy ageing process other important life style factors (healthy diet, a lack of smoking, moderate or no alcohol consumption) must also be in place.
Individuals operating below set point levels of physical activity
People who have physical activity levels below their set point will have a compromised physiology because of the negative and pathology‐inducing effects of inactivity (Fig. 2 B). The diminishing physiology that is determined by the inherent ageing process will now be influenced by an interaction with the negative effects of inactivity and this interaction will be conducive to the production of those diseases that are related to inactivity.
In the early years the onset of diseases may be incipient or subclinical, but as age and inactivity interact individuals are likely to suffer from one or more pathologies. The onset of morbidity is uncertain and the decline in physiological function is not related to the inherent ageing process. Other lifestyle factors may also be suboptimal bringing further medical complications. Importantly, it is clear that sedentary people who decide to adopt, or who are prescribed, increased physical activity will benefit in terms of both physiological function and health status. The beneficial effects of increased activity at this point will depend upon numerous factors such as the extent to which inactivity has decreased physiological function and the amount of physical activity now undertaken.
Individuals operating above set point levels of physical activity
Increasing physical activity/exercise above the set point (for example to target a high level of a specific athletic performance), will allow adaption of the challenged physiological systems until maximum levels of exercise performance are reached (Fig. 2 C). Master athletes are representative of this group and will produce the documented performance curves illustrated in Fig. 1. However, an important aspect of the set point model is that increasing exercise levels above the set point in order to increase athletic performance will not necessarily improve health and would be detrimental to health in the case of overtraining. The diminution in athletic performance is the result of the inherent ageing process. Although absolute maximum levels of exercise decrease, they remain maximal relative to age and still produce maximum age‐related performance. We suggest that eventually in the final stages of life the levels of exercise necessary to produce a maximal performance will essentially coincide with the set point level and individuals will now enter the compressed morbidity zone. It could be argued that if age‐related performance curves from individuals of differing ability could be normalised for physiological differences, they would essentially superimpose. This controlled and integrated ageing is the same process that is exerting its effects on those individuals at set point levels of physical activity (Fig. 2 A).
Master athletes compared to other models of ageing
The literature of theoretical models that have addressed the biology of ageing per se is fairly extensive but explanation of the process in the context of human physiology remains elusive (Edelstein‐Kechet et al. 2001; Steinsaltz et al. 2012). Sedentariness has been shown to alter the profiles of nearly all physiological indices and using the values of these indices to construct models of ageing will be erroneous. For example, the widespread theories of mitochondrial dysfunction or telomere lengths being linked to inherent human ageing is likely based on values of these indices being obtained from participants whose physiology is already compromised by the effects of inactivity or stress (Werner et al. 2008; Peterson et al. 2012). The free radical theory of ageing also deserves testing in subjects who are lifelong vigorous exercisers (Beckman & Ames, 1998). These theories are best described as hypotheses linking physiological systems damaged by inactivity to incipient disease. One example in support of this concept is the study by Lanza et al. (2008) who tested the effects of exercise on two physiological processes that are widely reported to be due to ageing, i.e. reduced insulin sensitivity and mitochondrial dysfunction. The exercisers studied had performed at least 1 h of cycling or running 6 days a week over the previous 4 years or longer. These subjects were likely exercising above their given set points and are representative of an approach that does not need to study elite athletes in order to investigate the ageing process. In contrast to the sedentary individuals who, it might be argued, had physical activity levels below their set point, no age effects on insulin sensitivity or mitochondrial oxidative function were observed in the exercisers.
Human ageing research: an interdisciplinary science
Estes & Binney (1989) wrote about the medicalisation of ageing and how this ‘biomedicalisation’ socially constructs old age as a process of decremental physical decline and places ageing under the domain and control of biomedicine. In this specialty of biomedicine, a piecemeal approach has been adopted to diseases of ageing that leads to the rapid replacement of one disease by another (Gems, 2011). This construction is based on data mostly obtained from sedentary subjects. However, as Tulle (2008) has noted, the science of ageing should neither be the property of biomedicine nor, indeed, become solely the province of exercise scientists. As discussed, an exercising participant is the most appropriate in whom the physiology of optimal ageing should be studied provided that nutritional status and other important lifestyle and environmental factors are not confounding influences.
Most of the data in this review could be viewed as an exercise scientist's perspective of ageing viewed through the prism of physical ability. However the fundamental biological processes underlying human ageing are not necessarily being elucidated unless an understanding of the physiological mechanisms of exercise equate to knowledge of ageing. There are other factors, such as mind–body interactions and mechanisms of physiological integration, that need to be explained. However, it is known that being physically active enables older people to recover a sense of physical and mental wellbeing (Tulle, 2008). We recognise that the end point for all humans is death, but we question whether that end point must necessarily be reached via polypharmacy and multiple organ failure. The pathway from being optimally aged to death may have a different and better trajectory which includes an increased healthspan and a compressed end of life morbidity.
Additional information
Competing interests
None declared.
Author contributions
Both authors have approved the final version of the manuscript and agree to be accountable for all aspects of the work. All persons designated as authors qualify for authorship, and all those who qualify for authorship are listed.
Biographies
Norman Lazarus has a medical degree from South Africa and a PhD from the State University of New York. He has worked in academia and in the pharmaceutical industry. Since 2006 he has been Emeritus Professor at the Centre of Human Aerospace and Physiological Sciences at King's College London. His particular interest is in trying to unravel the interactions between exercise, healthspan and ageing in humans.

Stephen Harridge obtained his PhD from the University of Birmingham and performed postdoctoral training at the Karolinska Institute, Sweden and Copenhagen Muscle Research, Denmark. His first faculty positions were at the Royal Free Hospital School of Medicine and in the Department of Physiology, University College London. Since 2005 he has been Professor of Human and Applied Physiology at King's College London, where he is Director of the Centre of Human and Aerospace Physiological Sciences. Using cell biology through to exercise physiology approaches his research focuses on increasing understanding of human skeletal muscle function and plasticity, with particular regard to ageing.
This review was presented at the symposium “Sports and exercise medicine”, which took place at the meeting of The Biomedical Basis of Elite Performance in Nottingham, UK, 6–8 March 2016.
References
- Araújo CGS & Scharhag J (2016). Athlete: a working definition for medical and health sciences research. Scand J Med Sci Sports 26, 4–7. [DOI] [PubMed] [Google Scholar]
- Baker AA & Tang YQ (2010). Aging performance for masters records in athletics, swimming, rowing, cycling, triathlon and weightlifting. Exp Aging Res 36, 453–477. [DOI] [PubMed] [Google Scholar]
- Basset DR & Howley ET (2000). Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exerc 32, 70–84. [DOI] [PubMed] [Google Scholar]
- Beckman KB & Ames BN (1998). Free radical theory of ageing matures. Physiol Rev 78, 547–581. [DOI] [PubMed] [Google Scholar]
- Booth FW, Chakravarthy MV & Spangenburg EE (2002). Exercise and gene expression: physiological regulation of the human genome through physical activity. J Physiol 534, 399–411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Booth FW, Roberts CK & Laye MJ (2012). Lack of exercise is a major cause of chronic disease. Compr Physiol 2, 1143–1211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bouchard C, Blair SN & Katzmarzyk PT (2015). Less sitting, more physical activity, or higher fitness? Mayo Clin Proc 90, 1533–1540. [DOI] [PubMed] [Google Scholar]
- Bouchard C, Shephard RJ. & Stephens T. (eds) (1994). Physical Activity and Health: International Proceedings and Consensus Statement. Human Kinetics, Champaign, IL. [Google Scholar]
- Edelstein‐Keshet L, Israel A & Lansdorp P (2001). Modelling perspectives of ageing: Can mathematics help us stay young? J Theor Biol 213, 509–525. [DOI] [PubMed] [Google Scholar]
- Estes CL & Binney EA (1989). The biomedicalization of aging: dangers and dilemmas. Gerontologist 29, 587–596. [DOI] [PubMed] [Google Scholar]
- Fries JF (1980). Aging, natural death, and the compression of morbidity. N Engl J Med 303, 130–135. [DOI] [PubMed] [Google Scholar]
- Gems D (2011). Tragedy and delight: the ethics of decelerated ageing Philos Trans R Soc Lond B Biol Sci 366, 108–112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hallal PC & Lee I‐M (2013). Prescription of physical activity: an undervalued intervention. Lancet 381, 356–357. [DOI] [PubMed] [Google Scholar]
- Hawkins SA, Marcell TJ, Jaque SV & Wiswell RA (2001). A longitudinal assessment of change in VO2max and maximal heart rate in master athletes. Med Sci Sports Exerc 33, 1744–1750. [DOI] [PubMed] [Google Scholar]
- Hawkins SA, Wiswell RA & Marcell TJ (2003). Exercise and the master athlete – a model of successful aging. J Gerontol A Biol Sci Med Sci 58, M1009–M1011. [DOI] [PubMed] [Google Scholar]
- Hill AV (1925). The physiological basis of athletic records. Lancet 209, 483. [Google Scholar]
- Korhonen MT, Mero AA, Alén M, Sipilä S, Häkkinen K, Liikavainio T, Viitasalo JT, Haverinen MT & Suominen H (2009). Biomechanical and skeletal muscle determinants of maximum running speed with aging. Med Sci Sports Exerc 41, 844–856. [DOI] [PubMed] [Google Scholar]
- Lanza IR, Short DK, Short KR, Raghavakaimal S, Basu R, Joyner MJ, McConnell JP & Nair KS (2008). Endurance exercise as a countermeasure for aging. Diabetes 57, 2933–2942. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lazarus NR & Harridge SDR (2007). Inherent ageing in humans: the case for studying master athletes. Scand J Med Sci Sports 17, 461–463. [DOI] [PubMed] [Google Scholar]
- Lazarus NR & Harridge SDR (2010). Exercise, physiological function and the selection of participants for ageing research. J Gerontol A Biol Sci Med Sci 65, 854–857. [DOI] [PubMed] [Google Scholar]
- Meltzer DE (1994). Age dependence of Olympic weightlifting ability. Med Sci Sports Exerc 26, 1053–1067. [PubMed] [Google Scholar]
- Pedersen BK & Saltin B (2015). Exercise as medicine – evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports 35, 1–72. [DOI] [PubMed] [Google Scholar]
- Peterson CM, Johannsen DL & Ravussin E (2012). Skeletal muscle mitochondria and aging: a review. J Aging Res 2012, 194821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pierce MB, Silverwood RJ, Nitsch D, Adams JE, Stephen AM, Nip W, Macfarlane P, Wong A, Richards M, Hardy R & Kuh D (2012). Clinical disorders in a post war British cohort reaching retirement: evidence from the first national birth cohort study. Plos One 7, e44857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rittweger J, di Prampero PE, Maffulli N & Narici MV (2009). Sprint and endurance power and ageing: an analysis of master athletic world records. Proc Biol Sci 276, 683–689. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Seals DR, Justice JN & LaRocca TJ (2016). Physiological geroscience: targeting function to increase healthspan and achieve optimal longevity. J Physiol 594, 2001–2024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Senefeld J, Joyner MJ, Stevens A & Hunter SK (2016). Sex differences in elite swimming with advanced age are less than marathon running. Scand J Med Sci Sports 26, 17–28. [DOI] [PubMed] [Google Scholar]
- Steinsaltz D, Mohan G & Kolb M (2012). Markov models of ageing theory and practice. Exp Gerontol 47, 792–802. [DOI] [PubMed] [Google Scholar]
- Tanaka H & Seals DR (2003). Dynamic exercise performance in masters athletes: insight into the effects of primary human aging on physiological functional capacity. J Appl Physiol 95, 2152–2162. [DOI] [PubMed] [Google Scholar]
- Tanaka H & Seals DR (2008). Endurance exercise performance in masters athletes: age‐associated changes and underlying physiological mechanisms. J Physiol 586, 55–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tulle E (2008). Acting your age? Sports science and the ageing body. J Aging Stud 22, 340–347. [Google Scholar]
- Werner C, Hanhoun M, Widmann T, Kazakov MA, Semenov A, Poss J, Bauersachs J, Thum T, Pfreundschuh M, Muller P, Haendeler J, Bohm M & Laufs U (2008). Effects of physical exercise on myocardial telomere‐regulating proteins, survival pathways, and apoptosis. J Am Coll Cardiol 52, 470–482. [DOI] [PubMed] [Google Scholar]
- Wiswell RA, Hawkins SA, Jaque SV, Hyslop D, Constantino N, Tarpenning K, Marcell T & Schroeder TE (2001). Relationship between physiological loss, performance decrement and age in master athletes. J Gerontol A Biol Sci Med Sci 56A, M618–M626. [DOI] [PubMed] [Google Scholar]