

Abstract
Diabetes mellitus is associated with adverse outcomes in patients with cardiovascular diseases, including heart failure. Left ventricular assist devices (LVADs) are increasingly used as life-saving therapy for advanced heart failure. The effects of pre-LVAD diabetes on long-term outcomes after LVAD implantation are not well understood. In this study, we retrospectively evaluated the effect of existing diabetes on post-LVAD outcomes.
Data on 288 LVAD recipients from 2006 through 2013 were reviewed. Patients were stratified in accordance with their histories of diabetes. Baseline demographic, laboratory, hemodynamic, and echocardiographic information before LVAD placement were reviewed, together with the post-LVAD incidence of major adverse outcomes. Kaplan-Meier analysis and Cox regression analysis were performed.
Our cohort comprised 122 patients with diabetes and 166 patients without. The mean glycosylated hemoglobin A1c level in the diabetes group was 7.4% ± 1.6%. Diabetic patients at baseline had a more adverse medical profile than did nondiabetic patients. There were no differences in major outcomes between the 2 groups other than a higher incidence of hemolysis in the diabetes group: 12 (10%) vs 5 (3%); P=0.02. There was no difference in survival outcomes between the groups.
Diabetic patients did not have worse survival or more adverse outcomes than did nondiabetic patients in this study, perhaps because of improved diabetes control, or improvement in biochemical derangements after normalization of cardiac output with LVAD therapy. A diagnosis of diabetes was an independent predictor of hemolysis. Further studies to evaluate the link between hemolysis and diabetes are indicated.
Keywords: Diabetes mellitus/complications, heart failure, hemolysis, left ventricular assist devices, retrospective studies, treatment outcome
Diabetes mellitus (DM) is a major risk factor for cardiovascular diseases and is associated with coronary artery disease, strokes, peripheral artery disease, cardiomyopathy, and congestive heart failure (CHF).1 The association between DM and CHF has been well established by the Framingham data, which indicated that DM leads to an estimated 2.4-fold increase in CHF incidence in men, and up to a 5-fold increase in women.2 The incidence of CHF is increasing in today's aging population and is projected to reach 772,000 new cases by the year 2040.3–5 Diabetes is also a well-known and independent risk factor for CHF morbidity and death.6–8 A 1% increase in glycosylated hemoglobin A1c (HbA1c) is associated with an 8% increase in the risk of heart-failure development.9
Although heart transplantation is considered a gold-standard treatment for advanced-heart-failure patients, DM, even in the absence of end-organ damage, is a relative contraindication to heart transplantation.10 Because of the paucity of available hearts for transplantation, left ventricular assist devices (LVADs) are increasingly being used as a bridge to transplantation or as destination therapy in advanced-heart-failure patients.11–13 The effects of pre-LVAD diagnoses of DM on the outcomes of diabetic patients are not well understood.14 Therefore, we investigated outcomes after LVAD implantation, in both diabetic and nondiabetic patients. We hypothesized that DM patients, as conventionally depicted, would have worse outcomes after LVAD implantation than would non-DM patients.
Patients and Methods
This retrospective, institutional-review-board-approved study included 288 consecutive patients who underwent LVAD placement from 2006 through 2013 at Advocate Christ Medical Center, Oak Lawn, Illinois. Of these, 244 had a HeartMate II® LVAD (Thoratec, part of St. Jude Medical, Inc.; Pleasanton, Calif) and 44 had a HeartWare HVAD® (HeartWare, Inc.; Framingham, Mass). Patients were stratified in accordance with the presence or absence of DM. Diabetes mellitus was defined as a preexisting history of DM on chart review, or on the patient's use of insulin or oral hypoglycemic medications, or on the patient's new diagnosis of DM on the basis of a laboratory value of HbA1c >7%.
Demographic information—including sex, race, body mass index, height, and weight—was obtained through retrospective chart review. Baseline medical information at the time of LVAD placement was tabulated. These data included cardiac risk factors, prior cardiac history, and hemodynamic and echocardiographic data on admission. Pre-LVAD laboratory values, including HbA1c, were collected. Information on post-LVAD HbA1c and major adverse outcomes—including death, heart failure, hospitalizations, gastrointestinal bleeding, stroke/transient ischemic attack, intracranial hemorrhage, hemolysis, thrombosis, pump exchanges, infections, and postoperative right ventricular failure—were obtained.
For the purposes of the study, hemolysis was defined as a lactate dehydrogenase (LDH) level >650 U/L, or as clinically substantial hemolysis resulting in hospitalization.
Statistical Analysis
Data were analyzed with use of SPSS 19 (IBM Corporation; Endicott, NY). Continuous variables were summarized as mean ± SD. Student t tests were used to evaluate differences in continuous variables. Categorical variables were displayed as percentages and were compared by means of χ2 testing. Kaplan-Meier survival analysis was performed. Binary logistic regression and Cox survival analysis were performed as well. A P value <0.05 was considered statistically significant.
Results
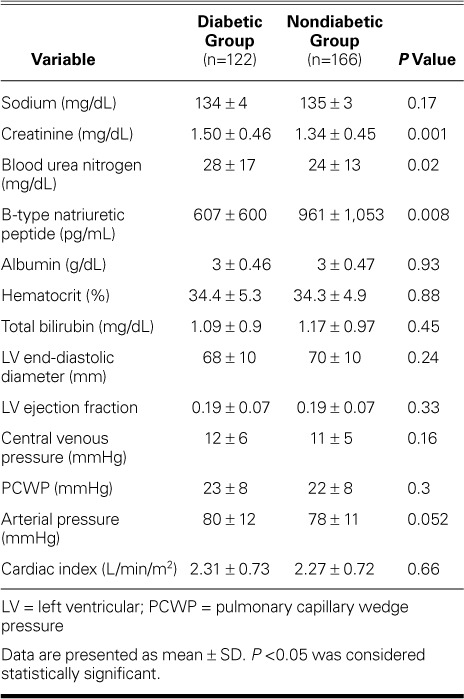
The mean durations of follow-up were 1,132 ± 878 days for the DM group and 1,143 ± 875 days for the non-DM control group. The diabetic patients were, on average, older than the nondiabetic patients (mean age, 62 ± 11 vs 59 ± 14 yr; P=0.03) and were more obese (body mass index, 29.8 ± 6 vs 26.6 ± 6 kg/m2; P <0.001). The diabetic patients had more comorbidities, such as atrial fibrillation (48% vs 33%; P =0.01) and obstructive sleep apnea (30% vs 14%; P =0.001) (Table I). There were no differences between the 2 populations in baseline laboratory data (Table II), although the DM group had an elevated mean creatinine level and a lower mean B-type natriuretic peptide level (1.5 vs 1.34 mg/dL; P=0.001; and 607 vs 961 pg/dL; P= 0.008). The mean pre-implantation HbA1c level in the DM patients was 7.4% ± 1.6%.
TABLE I.
Baseline Data in the 2 Groups
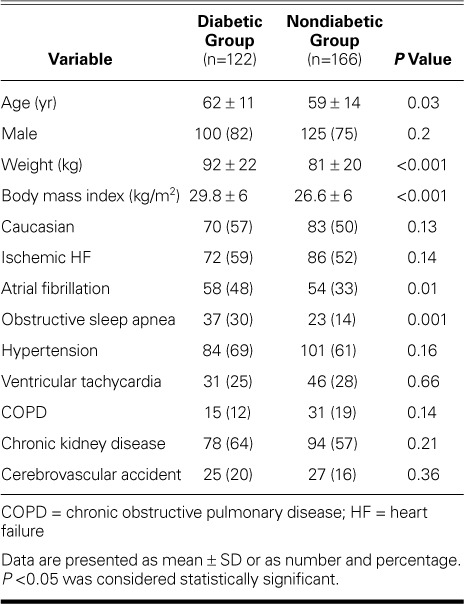
TABLE II.
Baseline Laboratory, Hemodynamic, and Echocardiographic Values in the 2 Groups
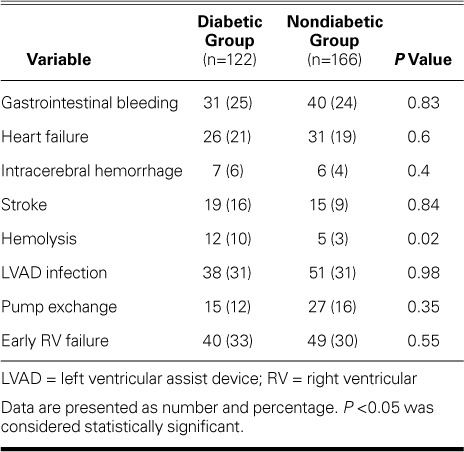
Outcomes. Post-LVAD outcomes analysis yielded no significant differences in adverse events between the groups (Table III). The incidence of post-LVAD hemolysis was higher in the DM group (10% vs 3%; P=0.02). Despite this increase in hemolysis, a corresponding statistically significant increase in pump exchanges was not seen (Table III). Kaplan-Meier survival analysis revealed no differences in all-cause death between the groups (1,326 vs 1,551 d; log rank P =0.71). The post-implantation HbA1c level was significantly better than that before implantation (6.2% ± 1.2% vs 7.4% ± 1.6%; P <0.001).
TABLE III.
Adverse Outcomes in the 2 Groups
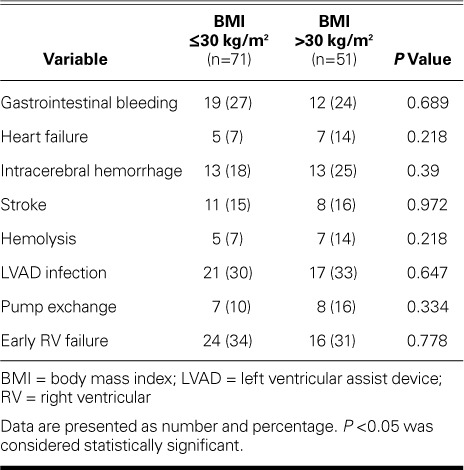
Obesity Paradox. Because our diabetic group was mainly obese (mean body mass index, 29.8 ± 6 kg/m2), we entertained the possibility of an obesity paradox contributing to lack of survival differences between the 2 groups. Our analysis revealed no difference in outcomes within the diabetic group stratified by a body mass index cutoff of 30 kg/m2 (Table IV).
TABLE IV.
Evaluation of the Obesity Paradox in the Diabetic Population
Adjustments for Covariates. Because of the statistically significant differences between the groups in age, body mass index, renal function, and atrial fibrillation, we performed a binary logistic regression for hemolysis, controlling for the above-listed covariates. The analysis revealed that DM was an independent predictor for hemolysis (odds ratio=4.77; 95% confidence interval [CI], 1.4–16.2; P=0.01). Similarly, a Cox regression analysis was performed to control for the above covariates and to evaluate survival function. The analysis did not reveal DM as a predictor of poor survival in these patients (hazard ratio=0.99; 95% CI, 0.65–1.6; P=0.97) (Fig. 1).
Fig. 1.
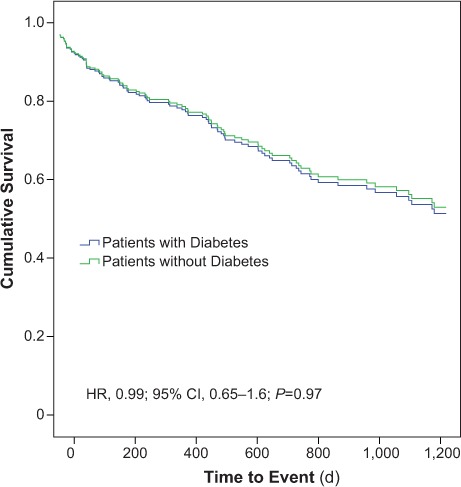
Graph illustrates Cox survival analysis after controlling for age, body mass index, renal function, and atrial fibrillation. It shows no statistically significant difference between survival outcomes in diabetic and nondiabetic patients.
P <0.05 was considered statistically significant.
CI = confidence interval; HR = hazard ratio
Discussion
Diabetes mellitus is often considered an adverse risk factor for heart disease. Evidence suggests that diabetic patients with heart disease have a more adverse prognosis than do nondiabetic patients.14,15 Such an evaluation is lacking in patients who undergo LVAD therapy. Diabetic patients with advanced heart failure that necessitates LVAD implantation are conventionally thought to be at a higher risk of adverse outcomes—associated mainly with a more aggressive disease phenotype, increased comorbidities, increased risk of postoperative infections, and poor outcomes and survival prospects.16–18
In our study, we have shown that diabetic patients, despite having an unfavorable baseline medical profile, did not have significantly adverse post-LVAD outcomes in comparison with nondiabetic patients. These findings are intriguing and contrary to traditional thinking. Although DM patients are often thought to be at increased risk of infection, an increase in post-LVAD occurrence of infection was not seen in our group.16 In addition, the incidence of stroke, which is typically higher in DM patients, was nonsignificant between groups.19,20 Similar results were noted for ventricular and atrial arrhythmias.
Diabetic patients with CHF are also thought to have poorer event-free survival prospects than do non-DM patients. In the Studies of Left Ventricular Dysfunction (SOLVD) trial, the authors concluded that patients with DM had higher all-cause, cardiovascular, and pump-failure mortality rates.15 Similarly, Bertoni and colleagues8 showed that DM patients with CHF had a mortality rate of almost 33% at one year, and an age-, sex-, and race-adjusted hazard ratio of 9.5. Although survival analysis in advanced-heart-failure DM patients with LVADs is lacking, our analysis indicated that there was no difference in survival between DM and non-DM groups. Cox regression survival analysis controlling for possible confounders also did not reveal any difference between the 2 groups (Fig. 1).
Our DM group had a higher incidence of hemolysis. However, our binary logistic regression model controlling for age, body mass index, atrial fibrillation, and chronic kidney disease indicated that DM was an independent risk factor for hemolysis. Hemolysis tends to be higher in continuous-flow LVAD patients because of increased shear stress exposure on erythrocytes. Despite the above-noted increase in hemolysis, no corresponding increase in pump exchanges was noted between the 2 groups. The phenomenon of increased red-blood-cell fragility secondary to hyperglycemia has been reported previously.19 This is thought to result from glucose-induced membrane lipid peroxidation, which can lead to increased osmotic fragility in erythrocytes.20 It might be possible that such increased fragility of the red blood cell membranes and LVAD shear contributed to higher hemolysis in our study group. However, these findings might be happenstance. In addition, the low absolute incidence of hemolysis in both the study and control groups might have confounded our findings.
Our DM patients showed significant improvement in HbA1c levels on follow-up testing (7.4% ± 1.6% vs 6.2% ± 1.2%; P <0.001). Such improvement might be because of increased access to DM care after LVAD placement. In addition, as previously reported, LVAD therapy itself improves glycemic control, possibly because of decreased pancreatic congestion, normalization of biochemical derangements that result from depressed cardiac output, and improved circulation of insulin.21–24 Finally, a multidisciplinary team approach to LVAD patients, including dietary consultation, might lead to improved glycemic control.21 It is possible that such aggressive treatment resulted in a lack of significant differences in outcomes and survival between DM and non-DM groups. Further research is needed to confirm these findings.
Last, because many of our DM patients were obese, we explored the possibility of an obesity paradox in our group. The obesity paradox is a poorly understood but well-reported phenomenon in which obese CHF patients have better survival rates than nonobese patients.25,26 We postulated, as previously reported, that the obesity paradox could have improved survival in our DM group. Our analysis failed to show any major difference between the obese and nonobese DM patients, eliminating any obesity-related confounders. Review of our data indicates that obese DM patients have significantly lower B-type natriuretic peptide levels than do nonobese DM patients (425 vs 737 pg/mL; P=0.006). In addition, it remains unclear whether the obesity paradox applies to our advanced-heart-failure diabetic patients who had received an LVAD. Further investigation into the possibility of such a link is indicated.
Limitations
This retrospective study was subject to inherent limitations. The sample size was small. Patient information was collected by means of chart review, which carries the potential of incomplete clinical records. Despite these limitations, we think that this study has important clinical implications for diabetic patients who are under consideration for LVAD implantation.
Conclusion
Although DM is a risk factor for poor cardiovascular outcomes, LVAD implantation may proceed in diabetic advanced-heart-failure patients without an increased risk of adverse events or worsened prospects for survival. A diagnosis of DM should not be used as a contraindication for advanced therapies. Diabetes is an independent predictor of post-LVAD hemolysis, but it does not appear to be associated with increased pump thrombosis or the need for pump exchange.
References
- 1. Buse JB, Ginsberg HN, Bakris GL, Clark NG, Costa F, Eckel R, . et al. Primary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes Association. Circulation 2007; 115( 1): 114– 26. [DOI] [PubMed] [Google Scholar]
- 2. Kannel WB, Hjortland M, Castelli WP.. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 1974; 34( 1): 29– 34. [DOI] [PubMed] [Google Scholar]
- 3. Nichols GA, Hillier TA, Erbey JR, Brown JB.. Congestive heart failure in type 2 diabetes: prevalence, incidence, and risk factors. Diabetes Care 2001; 24( 9): 1614– 9. [DOI] [PubMed] [Google Scholar]
- 4. Owan TE, Redfield MM.. Epidemiology of diastolic heart failure. Prog Cardiovasc Dis 2005; 47( 5): 320– 32. [DOI] [PubMed] [Google Scholar]
- 5. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Blaha MJ, . et al. Heart disease and stroke statistics--2014 update: a report from the American Heart Association. Circulation 2014; 129( 3): e28– e292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Varela-Roman A, Grigorian Shamagian L, Barge Caballero E, Mazon Ramos P, Rigueiro Veloso P, Gonzalez-Juanatey JR.. Influence of diabetes on the survival of patients hospitalized with heart failure: a 12-year study. Eur J Heart Fail 2005; 7( 5): 859– 64. [DOI] [PubMed] [Google Scholar]
- 7. MacDonald MR, Petrie MC, Varyani F, Ostergren J, Michelson EL, Young JB, . et al. Impact of diabetes on outcomes in patients with low and preserved ejection fraction heart failure: an analysis of the Candesartan in Heart failure: Assessment of Reduction in Mortality and morbidity (CHARM) programme. Eur Heart J 2008; 29( 11): 1377– 85. [DOI] [PubMed] [Google Scholar]
- 8. Bertoni AG, Hundley WG, Massing MW, Bonds DE, Burke GL, Goff DC Jr.. Heart failure prevalence, incidence, and mortality in the elderly with diabetes. Diabetes Care 2004; 27( 3): 699– 703. [DOI] [PubMed] [Google Scholar]
- 9. Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, . et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000; 321( 7258): 405– 12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Marelli D, Laks H, Patel B, Kermani R, Marmureanu A, Patel J, . et al. Heart transplantation in patients with diabetes mellitus in the current era. J Heart Lung Transplant 2003; 22( 10): 1091– 7. [DOI] [PubMed] [Google Scholar]
- 11. Morgan JA, John R, Rao V, Weinberg AD, Lee BJ, Mazzeo PA, . et al. Bridging to transplant with the HeartMate left ventricular assist device: The Columbia Presbyterian 12-year experience. J Thorac Cardiovasc Surg 2004; 127( 5): 1309– 16. [DOI] [PubMed] [Google Scholar]
- 12. Hunt SA, Frazier OH.. Mechanical circulatory support and cardiac transplantation. Circulation 1998; 97( 20): 2079– 90. [DOI] [PubMed] [Google Scholar]
- 13. Alba AC, McDonald M, Rao V, Ross HJ, Delgado DH.. The effect of ventricular assist devices on long-term post-transplant outcomes: a systematic review of observational studies. Eur J Heart Fail 2011; 13( 7): 785– 95. [DOI] [PubMed] [Google Scholar]
- 14. From AM, Leibson CL, Bursi F, Redfield MM, Weston SA, Jacobsen SJ, . et al. Diabetes in heart failure: prevalence and impact on outcome in the population. Am J Med 2006; 119( 7): 591– 9. [DOI] [PubMed] [Google Scholar]
- 15. Shindler DM, Kostis JB, Yusuf S, Quinones MA, Pitt B, Stewart D, . et al. Diabetes mellitus, a predictor of morbidity and mortality in the Studies of Left Ventricular Dysfunction (SOLVD) Trials and Registry. Am J Cardiol 1996; 77( 11): 1017– 20. [DOI] [PubMed] [Google Scholar]
- 16. Yumun G, Erdolu B, Toktas F, Eris C, Ay D, Turk T, As AK.. Deep sternal wound infection after coronary artery bypass surgery: management and risk factor analysis for mortality. Heart Surg Forum 2014; 17( 4): E212– 6. [DOI] [PubMed] [Google Scholar]
- 17. Gimenes C, Barrile SR, Martinelli B, Ronchi CF, Arca EA, Gimenes R, . et al. Association of pre and intraoperative variables with postoperative complications in coronary artery bypass graft surgery. Rev Bras Cir Cardiovasc 2013; 28( 4): 518– 23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Ledur P, Almeida L, Pellanda LC, Schaan BD.. Predictors of infection in post-coronary artery bypass graft surgery. Rev Bras Cir Cardiovasc 2011; 26( 2): 190– 6. [PubMed] [Google Scholar]
- 19. Marar T. Amelioration of glucose induced hemolysis of human erythrocytes by vitamin E. Chem Biol Interact 2011; 193( 2): 149– 53. [DOI] [PubMed] [Google Scholar]
- 20. Jain SK. Hyperglycemia can cause membrane lipid peroxidation and osmotic fragility in human red blood cells. J Biol Chem 1989; 264( 35): 21340– 5. [PubMed] [Google Scholar]
- 21. Mohamedali B, Yost G, Bhat G.. Mechanical circulatory support improves diabetic control in patients with advanced heart failure. Eur J Heart Fail 2014; 16( 10): 1120– 4. [DOI] [PubMed] [Google Scholar]
- 22. Choudhary N, Chen L, Kotyra L, Wittlin SD, Alexis JD.. Improvement in glycemic control after left ventricular assist device implantation in advanced heart failure patients with diabetes mellitus. ASAIO J 2014; 60( 6): 675– 80. [DOI] [PubMed] [Google Scholar]
- 23. Uriel N, Naka Y, Colombo PC, Farr M, Pak SW, Cotarlan V, . et al. Improved diabetic control in advanced heart failure patients treated with left ventricular assist devices. Eur J Heart Fail 2011; 13( 2): 195– 9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Guglin M, Maguire K, Missimer T, Faber C, Caldeira C.. Improvement in blood glucose control in patients with diabetes after implantation of left ventricular assist devices. ASAIO J 2014; 60( 3): 290– 3. [DOI] [PubMed] [Google Scholar]
- 25. Lavie CJ, De Schutter A, Alpert MA, Mehra MR, Milani RV, Ventura HO.. Obesity paradox, cachexia, frailty, and heart failure. Heart Fail Clin 2014; 10( 2): 319– 26. [DOI] [PubMed] [Google Scholar]
- 26. Chase PJ, Davis PG, Bensimhon DR.. The obesity paradox in chronic heart failure: what does it mean? Curr Heart Fail Rep 2014; 11( 1): 111– 7. [DOI] [PubMed] [Google Scholar]