

Abstract
Introduction
Diabetes mellitus (DM) has evolved as a major public health concern worldwide, as its prevalence is increasing exponentially. Pakistan now ranks seventh among the countries with the highest burden of DM. It is expected to become one of the major causes of morbidity within the next 25 years. Therefore, finding an effective way to identify individuals at risk of developing diabetes is a necessity. The Finnish Diabetes Risk Score (FINDRISC) has proved to be an effective noninvasive screening tool for identifying individuals at risk for developing diabetes. The objective of this study was to determine the frequency of individuals who are at risk for developing DM and their risk of developing DM over the next 10 years using the FINDRISC tool.
Methods
A cross-sectional survey was conducted on 241 adults. The data were collected using the FINDRISC questionnaire followed by calculation of a summated score and analysis to determine the association between the risk factors under study and the risk of developing diabetes.
Results
Out of 241 study participants, 137 (56.8%) were men and 104 (43.1%) were women. Our study showed that 129 (53.5%) participants had low risk, 68 (28.2%) had slightly elevated risk, 27 (11.2%) had moderate risk and 17 (7%) had high risk of developing DM.
Conclusion
The general population should be educated about the importance of healthy lifestyle, with special emphases on maintaining an ideal body mass index and a low-risk waist circumference, along with daily fruit and vegetable intake and physical activity of at least 30 min/day.
Keywords: Diabetes, diabetes risk, findrisc, screening tool
Introduction
Diabetes mellitus (DM) has evolved as a major public health concern worldwide, as its prevalence is increasing exponentially. According to the World Health Organization (WHO), there are approximately 347 million people with diabetes all over the world, and due to its exponential growth, it has been estimated that DM will become the seventh leading cause of mortality worldwide by 2030. Among the deaths caused by DM, more than 80% occur in low- and middle-income countries. Thus, diabetes can have a great impact on our health system and economic productivity by contributing to absence from work, disability, premature retirement and premature mortality.1,2
Without any interventions at primary level, this epidemic will continue to grow. It is expected to become one of the major causes of disability and morbidity within the next 25 years. Immediate action is needed to control this wave of diabetes and to reverse this trend.3 This can be best achieved by identifying those at risk for developing diabetes at an early stage and then intervening by primary prevention.
According to the WHO, Pakistan has an estimated 10% prevalence of diabetes among the general population. It now ranks seventh among countries with the highest burden of DM.4 The most alarming prediction is that Pakistan is expected to rank fourth among the countries with the highest burden of diabetes by 2030.5
Therefore, finding an effective way to identify individuals at risk for developing diabetes and to prevent DM is an important public health priority.
According to Chen et al.,6 a diabetes risk score can be used as an initial screening step, followed by a diagnostic test including an oral glucose tolerance test (OGTT). OGTT has long been used as a screening test for diabetes, but it is not feasible at the mass level. Using a risk score may greatly reduce the number of individuals who would otherwise need to undergo an OGTT while achieving adequate sensitivity, specificity and positive predictive value (PPV).7 The Finnish Diabetes Risk Score (FINDRISC) was found to be an effective tool for assessing diabetes risk from previous studies. A FINDRISC score of ≥15 was associated with a sensitivity and specificity of 67.7% and 67.2%, respectively, PPV of 51% and a negative predictive value of 80.5% for dysglycaemia (impaired fasting glucose + impaired glucose tolerance + Type 2 DM).8 Keeping in view that Pakistan is a developing country where people have limited resources and most of them cannot afford to have screening tests at their own expenses, there must be a diabetes risk assessment tool to identify high-risk individuals so that these individuals can be further tested through investigations and advised to take preventive measures.
FINDRISC is a simple, noninvasive screening tool to identify at-risk individuals for type 2 DM. The efficacy of FINDRISC has been proved in previous studies and was found to be positively associated with the prevalence of prediabetes (odds ratio [OR] = 1.15) and diabetes (OR = 1.48).9 A recent study from India showed that 12% of the Indian population is at high risk and approximately 75% is at moderate risk for developing diabetes.10
Various risk factors for developing DM have been reported. According to American Diabetes Association and International Diabetes Federation, physical inactivity, body mass index (BMI) > 25 kg/m2, family history of diabetes, hypertension and central obesity contribute towards the development of type 2 DM.11,12
To the best of our knowledge, very limited data from Pakistan are available on this topic.
Considering this issue as the need of the hour, we have conducted a cross-sectional survey in squatter settlements of Karachi, Pakistan. The objective of the study was to predict the risk of developing diabetes in the Pakistani population over a period of 10 years. In this way, we can reduce the rate of exponential growth of diabetes in the population by doing interventions at the primary care level and hence increase economic productivity.
Methods
A cross-sectional survey was conducted including adults aged 20 years or more visiting primary healthcare centres in two squatter settlements between July and November 2014. The sample size was calculated by using WHO sample size calculator on the basis of the lowest prevalence of diabetes in Pakistan reported in previous research, which was found to be approximately 7%.13 The calculated sample size was 225. The data were obtained from two different squatter settlements of Karachi by means of nonprobability consecutive sampling. Ethical approval was obtained from the ethics review committee of the Department of Community Health Sciences of Ziauddin University, Karachi before the commencement of the study. All adult patients who came to the primary healthcare centres at the time of the study were approached for data collection after taking verbal consent. A total of 250 patients were approached for data collection, out of which 241 patients consented to participate, with a response rate of 96.4%. Patients with a history of DM and those who were undergoing anti-diabetic treatment were excluded from the study.
The data were collected by the doctors in outpatient clinics through an interviewer-based questionnaire. The reliability of questionnaire was tested with the Cronbach's alpha value of 0.70. This questionnaire was adopted from the Finnish Type 2 Diabetes Risk Assessment Form.10 This questionnaire was developed in the year 2001 and was rated by International Diabetes Federation as an effective patient questionnaire for diabetes risk assessment in the general population. It contains eight scored questions related to age, BMI, waist circumference (WC), physical activity, intake of fruit and vegetables, current intake of anti-hypertensive medications, family history of DM and personal history of high blood glucose level during health examination. This questionnaire gives a summated score that provides a measure of the probability of developing type 2 DM over the following 10 years with 85% accuracy.14
It also detects asymptomatic diabetes and abnormal glucose tolerance with high reliability in other populations.9 Figure 1 shows the FINDRISC scoring. It classifies the patients into five risk categories according to the scores which as follows:
<7 = Low (estimated 1 in 100 will develop diabetes)
7–11 = Slightly elevated (estimated 1 in 25 will develop diabetes)
12–14 = Moderate (estimated 1 in 6 will develop diabetes)
15–20 = High (estimated 1 in 3 will develop diabetes)
>20 = Very high (estimated 1 in 2 will develop diabetes)
Figure 1.
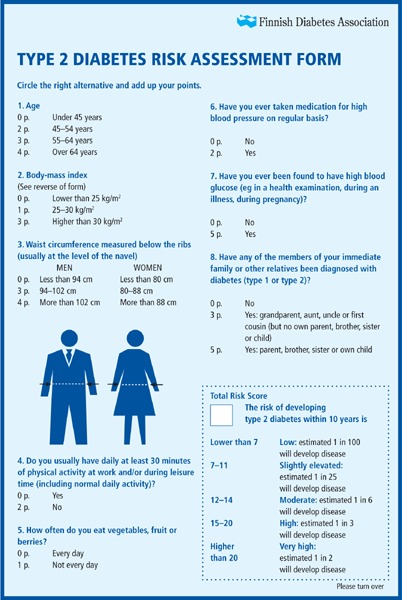
FINDRISC questionnaire with scoring
Height, weight, and waist and hip circumferences of all the subjects were measured, and BMI values were calculated for each patient. Weight of the patients was measured in light clothes only using bathroom scale to the nearest 0.1 kg. Height was measured without shoes, on a flat surface to the nearest 0.1 cm using wall-mounted stadiometers. The waist and hip circumferences were also measured using a measuring tape to the nearest 0.1 cm. BMI, WC and waist–hip ratio were classified according to the risk categories as defined by the WHO.15 Waist–hip ratio was categorised as follows: low risk (M ≤ 0.9 cm, F ≤ 0.85 cm) and high risk (M > 0.9 cm, F > 0.85 cm). WC was also defined according to WHO criteria as low risk (M < 94 cm, F = < 80 cm), high risk (M = 94–102 cm, F = 80–88 cm) and very high risk (M > 102 cm, F > 88 cm). WHO classification for BMI was used, where BMI between 18.5 and 24.9 kg/m2 was labelled as normal, BMI between 25 and 29.9 kg/m2 was labelled as overweight and BMI > 30 kg/m2 was categorised as obese.16
The data were analysed using IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp. For continuous variables such as weight, height, BMI and waist and hip circumferences, means and standard deviations were reported. Independent-samples t-test was applied to compare the anthropometry between the two genders. Categorical variables such as demographic characteristics and risk factors (WC, waist–hip ratio, frequency of fruit/vegetable intake, history of high blood sugar levels and intake of anti-hypertensive drugs) were expressed as percentages. Chi-square test was applied as the test of significance, considering p < 0.05 as significant.
Results
Out of 241 study participants, 137 (56.8%) were men and 104 (43.1%) were women. This was a multi-ethnic sample, with Pathans (28.6%) and Memons (37.8%) as predominant ethnic groups. Regarding marital status, 175 (72.6%) of the participants were married. Most of the men (86%) were employed, and 81% of the women were housewives. Socio-economic status analysis showed that monthly income of the majority of the participants (71.3%) was below Pakistani Rs. 20,000 (see Table 1). Comparison of anthropometric parameters between men and women is shown in Table 2. Although men had a higher mean for weight and height, mean BMI and waist and hip circumferences for women were higher than men.
Table 1.
Demographic characteristics
| Demographic parameter | N | Percentage |
|---|---|---|
| Gender | ||
| Male | 137 | 56.8 |
| Female | 104 | 43.2 |
| Ethnicity | ||
| Sindhi | 11 | 4.6 |
| Punjabi | 44 | 18.3 |
| Pathan | 69 | 28.6 |
| Balochi | 8 | 3.3 |
| Urdu speaking | 18 | 7.5 |
| Memon | 91 | 37.8 |
| Marital status | ||
| Single | 62 | 25.7 |
| Married | 175 | 72.6 |
| Widowed | 4 | 1.7 |
| Education | ||
| Nil | 57 | 23.7 |
| Primary | 57 | 23.7 |
| Matriculation | 65 | 27 |
| Graduation | 50 | 20.7 |
| Post-graduation | 12 | 5.0 |
| Monthly income (Rs.) | ||
| <10,000 | 89 | 36.9 |
| 10,000–20,000 | 83 | 34.4 |
| >20,000 | 69 | 28.6 |
| Occupation | ||
| Employed | 136 | 56.4 |
| Unemployed | 105 | 43.5 |
| Family type | ||
| Nuclear | 101 | 41.9 |
| Joint | 140 | 58.1 |
Table 2.
Relationship between gender and risk factors for DM
| Anthropometric measures | Men Mean ± SD | Women Mean ± SD | p-Value |
|---|---|---|---|
| Weight (kg) | 71.2 ± 13.5 | 67.4 ± 15.61 | 0.046 |
| Height (cm) | 170.2 ± 6.31 | 156.8 ± 7.09 | <0.001 |
| BMI (kg/m2) | 25.0 ± 5.17 | 26.8 ± 5.85 | 0.013 |
| Waist circumference (cm) | 86.1 ± 12.03 | 92.7 ± 15.43 | <0.001 |
| Hip circumference (cm) | 95.7 ± 10.92 | 104.9 ± 15.00 | <0.001 |
| Diet and lifestyle measures | N (%) | N (%) | |
| Physical activity >30 min | 101 (73.7) | 35 (33.7) | <0.001 |
| Fruit and vegetable intake | |||
| • Everyday | 103 (75.2) | 54 (51.9) | <0.001 |
| • Not everyday | 34 (24.8) | 50 (48.1) | |
| Taking antihypertensive medications | |||
| • Yes | 7 (5.1) | 19 (18.3) | 0.001 |
| • No | 130 (94.9) | 85 (81.7) | |
| Family history of DM | |||
| • No | 84 (61.3) | 56 (53.8) | |
| • Yes (grandparent, aunt, uncle or first cousin) | 14 (10.2) | 18 (17.3) | 0.246 |
| • Yes (parent, brother, sister, own child) | 39 (28.5) | 30 (28.8) |
Note: Test of significance: pooled t-test
Risk factors for DM as mentioned in the FINDRISC form were analysed according to the gender of the participants. With respect to risk categories, 129 (53.5%) of the participants had low risk, 68 (28.2%) had slightly elevated risk, 27 (11.2%) had moderate risk, 16 (6.6%) had high risk and 1 (0.41%) had very high risk of developing DM. When risk categories were further stratified according to gender, statistics were alarming. Figure 2 shows that as the risk score increases, the percentage of female population also increases; this difference was significant (p = <0.01).
Figure 2.
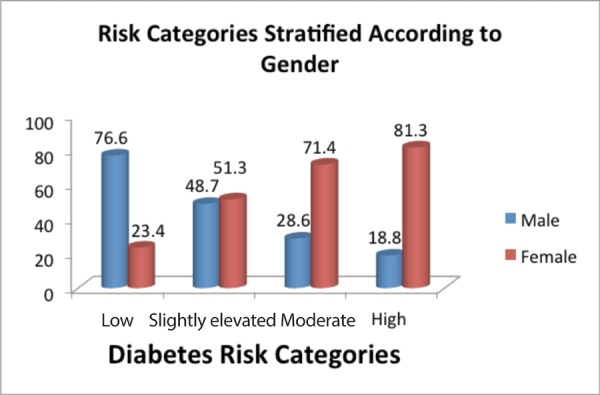
Risk of developing diabetes within 10 years (p = 0.033)
Difference in BMI was found to be statistically significant between the two genders (p = 0.013). Females were found to have a higher mean BMI as compared to males. In our study sample, women had a significantly higher WC and waist–hip ratio as compared to men (p < 0.001). A significant difference was found among men and women with respect to physical activity, daily intake of fruit and vegetable and current intake of anti-hypertensive medicines (p < 0.01). Positive family history of diabetes was not found to be a significant risk factor in our study.
Discussion
The FINDRISC tool was developed to identify persons at high risk for developing type 2 DM.17 In this study, we calculated the risk scores for patients in a cross-sectional setting. We used the FINDRISC tool for diabetes risk assessment in our population. This tool was previously used in a study by Saaristo et al. in 2005, and correctly identified 66% (men) and 70% (women) of previously undiagnosed patients with type 2 DM.17
Men with a WC of more than 102 cm and women with a WC of more than 88 cm were more likely to have high scores on FINDRISC (p < 0.001) and thus more likely to develop diabetes in future. Similar results were observed in a study by Siren et al. from Finland, where a WC ≥ 94 cm in middle-aged men was identified as a risk factor for type 2 diabetes, with a sensitivity of 84.4% (95% confidence interval [CI], 76.4–90.0%) and a specificity of 78.2% (95% CI, 68.4–85.5%).18
Majority of the men had a WC falling under low-risk category (WC < 94 cm), whereas the WC of a vast majority of women fell under high-risk category. These findings are also consistent with data from India.18
In our study population, 42% of the participants had a positive family history of diabetes, which is closer to the South Indian population.19 Among those who had a positive family history, 40% fell under moderate- to high-risk categories for developing diabetes.
The prevalence of the study participants at risk for developing type 2 diabetes within the next 10 years is shown in Figure 2. Among men, the prevalence of the participants at high risk for developing type 2 diabetes was found to be 2.9% as compared with other studies, including Wilson et al. (1.6%),19 FINDRISC (22.9%)20 and Griffin et al (24.9%).21 The female participants in our study showed a prevalence of 12.5% for high-risk category. When compared with the results from different parts of the world, our prevalence rates were higher than those reported by Wilson (1.1%),19 Balkau et al. (2.9%)22 and Kahn et al. (6.0%).23
A majority of studies have shown that men are more prone to develop diabetes.24 However, in the present study, more women were found to be at higher risk for developing diabetes, as compared with men. The reason for this could be the lifestyle of Pakistani women, who are mostly housewives with less active lifestyle and fewer outdoor activities. Therefore, they are more likely to be obese, thus explaining the findings of high-risk scores for women as compared with men.
Since a higher proportion of our female population was found to be at risk for developing diabetes due to physical inactivity, high-risk WC and poor fruit/vegetable intake, our suggestion is that at each visit to the primary care provider, the patient should be educated about the importance of at least 30 minutes of physical activity per day along with counselling on balanced nutrition, especially the intake of four to five portions of vegetable or fruit per day, to reduce the health risks. Emphasis should also be put on reducing weight, as the greater the BMI and WC, the greater will be the risk of developing diabetes. Another suggestion is that our female population should be given equal chances of participation in sports to enhance their activity level. This can be best achieved by creating awareness about the importance of healthy weight and adequate physical activity among school children and providing them with opportunities so that it becomes a part of their healthy behaviour.
This study is one of the preliminary studies done in Pakistan to find out at-risk population for diabetes using noninvasive risk assessment tool. The strength of this study is that, to the best of our knowledge, it is the first study of its kind in the Pakistani population. The limitation of this study is that it was only conducted in a low socio-economic group, so we do not have the data from higher socio-economic classes, where the results might have been different. Due to the nonprobability sampling method, the results of this study cannot be generalised. Another limitation of our study is that the FINDRISC tool was not validated in local language for the Pakistani population.
Conclusions
The general Pakistani population should be educated regarding the importance of a healthy lifestyle, with special emphases on maintaining an ideal BMI and a low-risk WC, along with daily fruit and vegetable intake and daily physical activity of at least 30 min/day. This would be beneficial in reducing the burden of DM in our population. Different strategies, including awareness sessions regarding lifestyle modifications, are required to sensitise the high-risk groups of our population and prevent them from developing DM in future.
Footnotes
Ishaque A, Shahzad F, Muhammad FH, et al. Diabetes risk assessment among squatter settlements in Pakistan: A cross-sectional study. Malays Fam Physician. 2016;11(2 & 3);9–15.
References
- 1.World Health Organization. [Accessed Mar 18;, 2014 ];Diabetes Programme. http://www.who.int/diabetes/en/ Available at:
- 2.Ontario Ministry of Health and Long-Term Care. [Accessed Apr 25;, 2014 ];Diabetes: Strategies for Prevention. http://www.health.gov.on.ca/en/common/ministry/publications/reports/diabetes/diabetes.aspx Available at:
- 3.CDC. Public health and aging: trends in aging—United States and worldwide. JAMA. 2003;52:101–6. [PubMed] [Google Scholar]
- 4.Gul N. Knowledge, attitudes and practices of type 2 diabetic patients. J Ayub Med Coll Abbottabad. 2010;22:128–31. [PubMed] [Google Scholar]
- 5. [Accessed Apr 25;, 2014 ];Diabetes Statistics in Pakistan. http://diabetespakistan.com/treatment/2013/05/08/diabetes-statistics-in-pakistan Available at:
- 6.Chen L, Magliano DJ, Balkau B. et al. Maximizing efficiency and cost-effectiveness of type 2 diabetes screening: the AusDiab study. Diabet Med. 2011;28:414–23. doi: 10.1111/j.1464-5491.2010.03188.x. [DOI] [PubMed] [Google Scholar]
- 7.Saydah SH, Byrd-Holt D, Harris MI. Projected impact of implementing the results of the Diabetes Prevention Program in the U.S. population. Diab Care. 2002;25(11):1940–45. doi: 10.2337/diacare.25.11.1940. [DOI] [PubMed] [Google Scholar]
- 8.Makrilakis K, Liatis S, Grammatikou S. et al. Validation of the Finnish diabetes risk score (FINDRISC) questionnaire for screening for undiagnosed type 2 diabetes, dysglycaemia and the metabolic syndrome in Greece. Diabetes Metab. 2011;37:144–51. doi: 10.1016/j.diabet.2010.09.006. [DOI] [PubMed] [Google Scholar]
- 9.Zhang L, Zhang Z, Zhang Y. et al. Evaluation of Finnish Diabetes Risk Score in screening undiagnosed diabetes and prediabetes among U.S. adults by gender and race: NHANES 1999–2010. PLoS One. 2014;9(5):e97865. doi: 10.1371/journal.pone.0097865. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Subramani R, Devi U, Shankar U. et al. Assessment of risk of type 2 diabetes mellitus among rural population in Tamil Nadu by using Indian diabetic risk score. Middle East J Sci Res. 2014;21:223–5. [Google Scholar]
- 11.American Diabetes Association. Standards of medical care in diabetes—2014. Diab Care. 2014;37:S14–80. doi: 10.2337/dc14-S014. [DOI] [PubMed] [Google Scholar]
- 12.International Diabetes Federation. [Accessed Feb 20;, 2016 ];Risk Factors. http://www.idf.org/about-diabetes/risk-factors Available at:
- 13.International Diabetes Federation. [Accessed Nov 29;, 2016 ];Pakistan. 2015 Jul 23; http://www.idf.org/membership/mena/pakistan [online] [cited. ] Available at:
- 14. [Accessed Jan 18;, 2015 ];Guidelines on Diabetes, Pre-diabetes and Cardiovascular Diseases: Executive Summary. http://eurheartj.oxfordjournals.org/content/28/1/88 Available at:
- 15. [Accessed Jan 14;, 2015 ];Waist Circumference and Waist-hip Ratio Report of A WHO Expert Consultation. Geneva. http://apps.who.int/iris/bitstream/10665/44583/1/9789241501491_eng.pdf Available at:
- 16.Finnish Diabetes Association. [Accessed Jan;2014 ];Type 2 Diabetes Risk Assessment Form. http://www.diabetes.fi/files/502/eRiskitestilomake.pdf Available at:
- 17.Saaristo T, Peltonen M, Lindström J. et al. Diabetes, abnormal glucose tolerance and metabolic syndrome cross-sectional evaluation of the Finnish Diabetes Risk Score: a tool to identify undetected type 2. DiabVasc Dis Res. 2005;2:67. doi: 10.3132/dvdr.2005.011. [DOI] [PubMed] [Google Scholar]
- 18.Siren R, Eriksson JG, Vanhanen H. Waist circumference a good indicator of future risk for type 2 diabetes and cardiovascular disease. BMC Public Health. 2012;12:631. doi: 10.1186/1471-2458-12-631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Wilson PW, Meigs JB, Sullivan L. et al. Prediction of incident diabetes mellitus in middle-aged adults: the Framingham offspring study. Arch Intern Med. 2007;167:1068–74. doi: 10.1001/archinte.167.10.1068. [DOI] [PubMed] [Google Scholar]
- 20.FINDRISK (“Finde das Risiko”) [Accessed Dec 12;, 2015 ];Fragebogen: Optimierte deutsche Version. http://www.diabetes-heute.De Available at:
- 21.Griffin SJ, Little PS, Hales CN. et al. Diabetes risk score: towards earlier detection of type 2 diabetes in general practice. Diabetes Metab Res Rev. 2000;16:164–171. doi: 10.1002/1520-7560(200005/06)16:3<164::aid-dmrr103>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- 22.Balkau B, Lange C, Fezeu L. et al. Predicting diabetes: Clinical, biological, and genetic approaches. Data from the epidemiological study on the insulin resistance syndrome (DESIR) Diab Care. 2008;31:2056–61. doi: 10.2337/dc08-0368. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kahn HS, Cheng YJ, Thompson TJ. et al. Two risk-scoring systems for predicting incident diabetes mellitus in U.S. adults age 45 to 64 years. Ann Intern Med. 2009;150:741–51. doi: 10.7326/0003-4819-150-11-200906020-00002. [DOI] [PubMed] [Google Scholar]
- 24.Harris MI, Hadden WC, Knowler WC. et al. Prevalence of diabetes and impaired glucose tolerance and plasma glucose levels in the US population. Diabetes. 1987;36:523–34. doi: 10.2337/diab.36.4.523. [DOI] [PubMed] [Google Scholar]