

Abstract
Neonatal herpes simplex virus (HSV) infections have high morbidity and mortality rates. Optimization of treatment and prevention strategies are imperative to improve the care and outcomes of neonates infected with HSV. Management of HSV includes reducing neonatal transmission, treating acute infections, and limiting adverse neurodevelopmental outcomes and future cutaneous outbreaks after acute infections. Transmission risk may be affected by route of delivery and maternal suppressive therapy. Neonatal HSV infections are divided into 3 categories: localized skin, eyes, or mouth; localized central nervous system; or disseminated infections. Parenteral acyclovir, the pharmacologic agent of choice, is used when treating each type of infection. However, dosage strategies and durations of therapy may vary based on disease state severity, presentation, and patient characteristics. Oral acyclovir may be used as suppressive therapy after acute treatment completion in specific neonatal populations, reducing long-term adverse neurodevelopmental outcomes and future skin eruptions. The mortality rate remains high even with treatment.
Keywords: acyclovir, congenital, disseminated, herpes simplex virus, neonatal HSV infection
Background
Herpes simplex viruses (HSVs) are double-stranded, enveloped DNA viruses. An estimated 1 in 3000 to 20,000 live births will be infected with HSV.1 Herpes simplex virus type 1 (HSV-1) and HSV type 2 (HSV-2) are the two types of HSVs that may cause neonatal disease.1,2 In 2012, HSV-1 prevalence was estimated at 3.7 billion people globally between the ages of 0 and 49 years, with an estimated 140 million people ages 15 to 49 years having genital HSV-1 infections.3 The HSV-2 prevalence in 2012 was estimated at 417 million individuals worldwide between the ages of 15 and 49 years.4 The burden increases risk of transmission of HSV infections to neonatal offspring.
Herpes simplex virus may be transmitted to the neonate via 4 methods: delivery through infected genital tract, ascending HSV exposure through ruptured amniotic membranes, intrauterine HSV exposures, or postnatal exposure from an infected caregiver. Intra-uterine transmission is rare, occurring in 1 in 100,000 to 300,000 births.2 Intrauterine or transplacental HSV exposure may lead to non-immune hydrops fetalis even in the setting of a recurrent infection or fulminant disseminated disease from maternal primary gingivostomatitis.5,6 Parra et al7 reported an example of HSV transmission postnatally while feeding from a breast with an HSV-1 skin lesion.
The methods of transmission can be classified into 3 different infection acquisition time frames: in utero, peripartum, or postpartum. Approximately 95% of neonatal HSV infections are acquired during the peripartum or postpartum periods.2 The risk of transmission to a neonate varies greatly based on type of maternal infection: primary or secondary. A neonate born to a mother with a primary genital HSV infection relatively near the time of delivery has an estimated infection risk of 25% to 60%.1 A neonate born to a mother who has a reactivated infection or secondary infection from a prior infection has an approximately 2% risk of HSV transmission.1 Other factors associated with increased risk of HSV transmission to a neonate are negative HSV antibody status, vaginal delivery, longer duration of membrane rupture, compromised cutaneous barrier (e.g., scalp electrode), and HSV-1 infection.8 More than 75% of neonates with HSV infections are born to mothers with no known history of a genital HSV infection, limiting maternal history impact on neonatal differential diagnoses.1,9
Presentation
Although rare, neonatal intrauterine HSV exposure presents with 3 classic manifestation locales: dermatologic, neurologic, and ocular. Cutaneous presentation may include aplastic cutis, hyperpigmentation, hypopigmentation, or lesions. Neurologic findings may include calcifications, hydranencephaly, or microcephaly. Ocular presentation may include chorioretinitis, microphthalmia, or optic atrophy.2
Neonatal peripartum- and postpartum-acquired HSV infections manifest in 3 specific forms: localized skin, eyes, or mouth disease; localized central nervous system (CNS) disease; or disseminated disease. Skin lesions may be a characteristic of all neonatal HSV infections. However, lesions may not be present at disease onset.1,2,9–12 Skin lesion cultures are often positive for HSV if present.10
Skin, Eyes, or Mouth Disease
An estimated 45% of neonatal HSV infections are skin, eyes, or mouth disease,1,2 which usually presents between 5 and 11 days of life.13 Skin lesions are present in more than 80% of neonates with skin, eyes, or mouth disease, with 20% involving eyes and/or mouth.1,2 Small vesicles are found on the skin near sites of compromised skin integrity or around the eyes or mouth. Inadequately treated disease may lead to CNS or disseminated disease.13 Of the 3 disease types, skin, eyes, or mouth disease has the best morbidity and mortality outcomes.1
CNS Disease
Central nervous system disease typically presents between 8 and 17 days of life.13 A total of 30% of HSV disease in neonates is localized CNS disease with or without skin manifestations.1,2 Up to two-thirds of neonates with CNS or disseminated disease have skin manifestations.1,2,9 Neonates with CNS disease often present with nondescript symptoms of decreased or inadequate enteral intake, irritability, lethargy, and temperature instability that mirror neonatal bacterial infections.2,10 Analysis of cerebrospinal fluid (CSF) may show pleocytosis.14 Physical signs of CNS disease may include a bulging fontanelle and seizures.3 A total of 50% of untreated neonates receiving a diagnosis of localized CNS disease will die. Surviving neonates will have severe neurologic sequelae.13
Disseminated Disease
Disseminated disease accounts for approximately 25% of neonatal HSV infections.1 Disseminated disease typically involves the lungs and/or liver of the neonate. Al Aswad and Suryadevara15 described a neonate receiving a diagnosis of disseminated disease, with hepatic involvement as the single-organ system presentation. Other organ systems may also be affected, including cardiac and adrenal systems.13 In approximately two-thirds of disseminated HSV infections, the CNS is also involved1 and/or the neonate has skin manifestations.1,2,9 Neonates with disseminated disease often present with fevers and respiratory distress or pneumonia.9,10,13 Neonates may also appear septic and experience disseminated intravascular coagulopathy.1,2,13 Typically patients have positive HSV blood polymerase chain reactions (PCRs), although this alone is not diagnostic for type of disease. Most patients have elevated transaminases, specifically aspartate and alanine, and C-reactive protein.9 Disseminated disease usually presents between days 5 and 11 of life. Only 10% of neonates survive when disseminated disease is untreated.13 Nearly 30% of neonates with disseminated disease die even with treatment.1 All surviving patients have severe neurologic sequelae, with delays in motor, speech, and development.13
Diagnosis
A conclusive neonatal HSV infection is best diagnosed using viral cultures. The American Academy of Pediatrics (AAP) recommends obtaining viral cultures via swab from the anus, conjunctivae, mouth, and nasopharynx, as well as suspected vesicles.1,16 Herpes simplex virus PCR may also be performed on samples obtained while swabbing the surfaces. The gold standard for diagnosis is a positive viral culture. Viral surface cultures should be obtained for all patients with or without HSV PCR analysis.1 Additional specimens may be obtained from blood, CSF, or skin lesions for HSV culture.1,17 The HSV cultures might not be evaluated at laboratories within all institutions, requiring specimens to be sent for outside assessment. Culture positivity is not required to initiate treatment. Treatment should begin immediately. Herpes simplex virus PCR testing is especially useful when the CNS is involved in either disseminated or CNS disease. A positive CSF HSV PCR confirms CNS involvement.16 Blood HSV PCR may be obtained. A positive blood HSV PCR may be the first or only positive result for patients.18 A positive blood result corroborates with neonatal HSV infection. However, blood HSV PCR cannot be used to determine the type of disease. Skin eyes, and mouth disease; CNS disease; or disseminated disease may have DNAemia or viremia, resulting in positive blood HSV PCR for an extended period of time, curbing serial use as a methodology for therapeutic response.1,11,17,19–21 Laboratory assessment should take place immediately in all suspected and symptomatic neonates, in conjunction with intravenous pharmacotherapy. If a neonate is born to a mother with suspected HSV genital lesions and the neonate is asymptomatic, laboratory assessment should be obtained 24 hours after birth. However if the neonate is ≤37 weeks' gestation or born after maternal prolonged rupture of membranes, defined as >4 to 6 hours, immediate assessment and initiation of intravenous acyclovir may be warranted.1
Prevention
Both the Royal College of Obstetricians and Gynecologists and the American Congress of Obstetricians and Gynecologists (ACOG) provide guidance for management of HSV disease in pregnancy, with the goal of preventing maternal-fetal transmission of the virus.22,23 Risk of perinatal transmission is associated with active maternal lesions; consequently, guidelines recommend delivery via cesarean delivery for women with active genital lesions or prodromal symptoms. Infants delivered via cesarean delivery with either intact or ruptured membranes can acquire congenital HSV infection; therefore, treatment should not be withheld in such infants if they are displaying signs and symptoms of active disease.
The ACOG and the Centers for Disease Control and Prevention recommend pregnant women with a history of genital herpes infection begin taking oral suppressive therapy at 36 weeks' gestation.23,24 Recommended medication options include oral acyclovir 400 mg 3 times daily or oral valacyclovir 500 mg twice daily. Currently no evidence demonstrates a decrease in maternal-fetal transmission due to prophylaxis, although it may reduce the number of recurrences near term, reducing the need for cesarean delivery. A case series published in 2012 documented 8 cases of neonatal herpes disease following maternal suppression therapy, demonstrating viral shedding may continue with antiviral prophylaxis.25
There is no vaccine available to prevent HSV infection, and routine screening of pregnant women for HSV is not recommended. The AAP recommends mothers with active HSV lesions on the breast not breastfeed the neonate. However, expressed maternal breastmilk may be used.26
Treatment
Early treatment regimens for congenital HSV infection included the use of vidarabine, although toxicities restricted its use.2,8,27,28 Acyclovir replaced vidarabine in the treatment of HSV because of its superior efficacy and better safety profile.28 Based on evidence demonstrating improved outcomes, parenteral acyclovir, which works by blocking viral DNA synthesis,28 has been the standard therapy for congenital HSV infection for several decades. Early studies established effectiveness of “low-dose” acyclovir (30 mg/kg/day); however, more recent data have demonstrated a lower mortality rate with “large-dose” acyclovir (60 mg/kg/day), establishing this regimen as the standard of care.29 The dosage continues to be the current recommendation from the AAP.1 Length of treatment varies depending on disease classification. Infants with skin, eyes, or mouth disease should be treated for 14 days. Infants with CNS or disseminated disease should be treated for a minimum of 21 days. Consideration should be given to the need to weight-adjust the acyclovir dose during the treatment course based on institution-specific policies or practices. Typically, adjustments occur when dosage exceeds 5% to 10% variance.
Infants treated for CNS disease should have a repeat CSF HSV PCR near the end of the treatment course. If the CSF HSV PCR result continues to be positive, then treatment should be extended past 21 days in 7-day increments until the CSF HSV PCR result is negative. Repeat CSF HSV PCR should occur near the end of the extended course.1 Rare cases of recurrent infection with CNS disease involvement have been documented, with at least 1 case thought to be related to inadequate evaluation at the end of the treatment course.30
Although the standard of care is accepted as acyclovir 60 mg/kg/day given as 20 mg/kg per dose every 8 hours, there is some variability in approach to treating premature infants. There have been reports of practitioners reducing frequency to every 12 hours at varying gestational ages because of decreased renal function in lower gestational ages. Other dosage considerations include need for potential dose escalation (e.g., 30 mg/kg per dose every 8 hours) in the setting of continuous renal replacement therapy and/or extracorporeal membranous oxygenation as described by Cies and colleagues.31
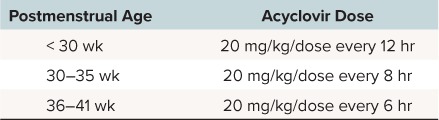
A population-based pharmacokinetic study using Monte Carlo simulation determined postmenstrual age is the most significant age predictor for acyclovir clearance.32 The pharmacokinetic modeling in this study was based on a target plasma steady-state concentration at half of the dosage interval ≥ 3 mg/dL, which was considered necessary to reach ≥1 mg/dL in CSF. This goal was established in a previous cohort, which found all HSV isolates to have a half-maximal inhibitory concentration of < 1 mg/dL. Dosage recommendations from that study are listed in the Table. It should be noted that this dosage is considered controversial and was not adopted in the latest edition of AAP's RedBook.
Table.
Intravenous Acyclovir Dosage Considerations Based on Monte Carlo Simulation32
Following intravenous treatment completion for disseminated or CNS infection, infants should receive oral suppression therapy.33 Although other doses have been reported in the literature, a randomized controlled trial established that acyclovir 300 mg/m2 per dose orally 3 times daily administered for 6 months can improve neurodevelopmental outcomes and decrease the number of cutaneous outbreaks.
Although the treatment of choice for HSV infection is clear, there has been debate over when empiric therapy should be initiated.34 Most patients screened for HSV are not infected, and commencement of empiric therapy increases cost as well as exposure to adverse effects from acyclovir. Evidence has demonstrated an association between delays in initiation of empiric acyclovir and increased mortality in neonates with HSV infections.35 The increase in risk of mortality is greatest in infants younger than age 14 days. Risk of mortality increases further with each day that therapy is delayed. Experts recommend initiating acyclovir in any instance when HSV is suspected. As previously described, the greatest risk of transmission occurs during primary infection of the pregnant woman. For this reason, empiric acyclovir should never be withheld in a symptomatic neonate on the basis of a negative maternal history of HSV infection.
Experts recommend that infants who present in the first 2 months of life with a sepsis-like picture in combination with elevated liver enzymes should receive empiric acyclovir.36 Most agree that infants presenting during this period of time with signs and symptoms of meningitis, such as fever or seizure, should receive empiric acyclovir while testing is completed. Empiric acyclovir is also recommended for neonates born to mothers with a presumed first-episode primary infection or first-episode non-primary infection (e.g., primary infection with HSV-2 but previously infected with HSV-1) when delivered vaginally or by cesarean delivery after membranes ruptured. Although the AAP does not specifically address this, Canadian guidelines state that acyclovir does not need to be started empirically for infants delivered via cesarean prior to rupture of membranes to mothers with presumed first-episode primary infection or first-episode non-primary infection, nor to those delivered vaginally to a mother with recurrent infection at delivery.36
Specific recommendations outline management of asymptomatic infants born to mothers with active lesions regardless of method of delivery.37 The approach to management of these infants depends on the presence or absence of maternal history of genital HSV infection prior to the pregnancy. Infants born to mothers with a prior history should have surface cultures (with or without HSV PCR) and blood HSV PCR testing at 24 hours of life. There is no need to start acyclovir if the infant remains asymptomatic. If virologic testing is negative, then no treatment is needed. Caregivers should be educated to recognize signs and symptoms of HSV disease should an infant develop symptoms after discharge. If virologic testing is positive, then CSF HSV PCR should be obtained and acyclovir should be initiated. If the infant remains asymptomatic, a preemptive 10-day course of acyclovir should be completed. If at any time the infant becomes symptomatic, then treat as previously described with acyclovir for 14 to 21 days depending on type of disease.
Asymptomatic infants born to mothers with active lesions and no prior history of genital HSV should have acyclovir initiated empirically.37 In addition to surface cultures (with or without HSV PCR) and blood HSV PCR testing at 24 hours of life, infants should have an alanine aminotransferase (ALT) and also undergo a lumbar puncture to obtain CSF cell count, chemistries, and HSV PCR. Maternal type–specific serologies should be sent if available at the delivery hospital. If this is determined to be the primary maternal infection, acyclovir should be continued as previously described (10 days if asymptomatic or 14 to 21 days depending on disease type if symptomatic). For recurrent maternal infection, acyclovir can be discontinued if all virology studies are negative. If virologic tests return positive, then treat as described previously.
Resistance
Although uncommon, acyclovir resistance does exist. The prevalence of resistance in the neonatal population is unknown but has been reported.37 The prevalence of acyclovir resistance is greater in immunocompromised patients compared with immunocompetent ones.38,39 Of note, one of the infants in the aforementioned case series evaluating maternal antiviral suppressive therapy was infected with a resistant organism.25 It is not known whether the resistance developed during maternal suppressive therapy or during treatment of the neonate. Resistance should be suspected if there is symptomatic treatment failure or persistently positive CSF PCR results.
Second-line therapies recommended for acyclovir-resistant HSV infections include foscarnet and cidofovir.39 Foscarnet is active against all known human herpes viruses regardless of resistance to other antivirals.40 It works by directly inhibiting DNA polymerase. Cidofovir competitively inhibits DNA polymerase and is active against both HSV and cytomegalovirus. The 2 agents are not well studied in neonatal populations. Additionally, both agents have a significant risk of adverse events. Specifically, some of the more serious adverse effects that foscarnet is associated with significant risk include nephrotoxicity and metabolic disturbances.40 Cidofovir is also associated with a significant risk for nephrotoxicity. Second-line therapies may require dose adjustments based on patient-specific parameters, including renal function.
Medication Shortage
Parenteral acyclovir is currently not only the gold standard for congenital HSV infection; it is the only recommended treatment. Because of poor oral bioavailability, oral acyclovir is not an acceptable alternative. Valacyclovir does offer the benefit of improved oral bioavailability. However, it has not been adequately studied as an alternative therapy for parenteral acyclovir. Oral antiviral agents are not recommended for acute management. Many times during the past decade, acyclovir could be found on a long list of medication shortages. Allocation and conservation often stretched supplies, but occasionally the shortage became concerning. The AAP made recommendations for alternative antiviral regimens during shortages. In the event that intravenous acyclovir is unavailable, first-line treatment is intravenous ganciclovir every 12 hours dosed at 6 mg/kg per dose for neonates.41 The secondary alternative is foscarnet 60 mg/kg per dose intravenously every 12 hours.41
Monitoring
In general, acyclovir is a well-tolerated medication. The adverse effects most often associated with acyclovir are renal dysfunction, related to crystalluria, phlebitis, and neutropenia. Adequate hydration is recommended during acyclovir therapy in order to prevent renal toxicity. Regular monitoring of serum creatinine and urine output is recommended to assess for this potential adverse effect. Acyclovir administration is associated with phlebitis and can be damaging to surrounding tissue if extravasation occurs. Routine assessment of the intravenous access site is recommended during acyclovir administration. To monitor for potential neutropenia, the absolute neutrophil count should be assessed twice weekly during the initial parenteral therapy.2 Absolute neutrophil counts should be monitored at weeks 2 and 4 ,and then monthly, for infants receiving oral acyclovir for suppression therapy. Acyclovir dose reduction or granulocyte colony–stimulating factor administration may be considered if the absolute neutrophil count remains under 500/m3 for a prolonged period. Absolute neutrophil counts often recover without intervention during the course of therapy or after completion of therapy.39 Neonates receiving a diagnosis of HSV infection should have a follow-up plan, including neurodevelopmental progress monitoring, regular ophthalmological examinations, and potential hearing-related issues as a result of the infection.36
Pharmacist Involvement
The role of the pediatric pharmacist is vital in managing neonatal HSV diseases. Pharmacists should recommend appropriate empiric medication dosage strategies and adjustments based on changing patient characteristics, such as renal function, neutropenia, or weight, if needed. Properly monitoring antiviral therapies allows for improved patient outcomes and reduced risk of adverse drug events. Pharmacists can proactively develop contingencies for medication unavailability and provide updated medication availability and treatment alternatives to the interprofessional health care team during shortages. A pharmacist may also facilitate the prescription, procuration, and dispensing of oral suppression therapy needed for qualifying neonates prior to discharge. Pharmacist involvement in an interprofessional health care team treating neonatal HSV infections not only addresses issues associated with a neonate's primary problem—the pharmacist also monitors maintenance medications, supplementation, and nutrition.
Conclusion
Neonatal HSV disease, although rare, is a serious, life-threatening condition. As discussed here, decreasing the delay in initiation of acyclovir treatment can improve outcomes. Advocating for early empiric acyclovir initiation in appropriate patients, initiating suppression therapy for qualifying patients, recommending alternative medications during drug shortages, and monitoring therapies are roles for pharmacists in neonatal populations with HSV infection.
Abbreviations
- AAP
American Academy of Pediatrics
- ACOG
American Congress of Obstetricians and Gynecologists
- CNS
central nervous system
- CSF
cerebrospinal fluid
- HSV
herpes simplex virus
- HSV-1
HSV type 1
- HSV-2
HSV type 2
- PCR
polymerase chain reaction
Footnotes
Disclosures The authors declare no conflicts or financial interest in any product or service mentioned in the manuscript, including grants, equipment, medications, employment, gifts, and honoraria.
Copyright Published by the Pediatric Pharmacy Advocacy Group. All rights reserved. For permissions, email: matthew.helms@ppag.org.
REFERENCES
- 1. Herpes simplex. : Kimberlin DW, Brady MT, . Red-Book: 2015 Report of the Committee on Infectious Diseases. 30th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2015: 432– 445. [Google Scholar]
- 2. James SH, Kimberlin DW.. Neonatal herpes simplex virus infection: epidemiology and treatment. Clin Perinatol. 2015; 42( 1): 47– 59. [DOI] [PubMed] [Google Scholar]
- 3. Looker KJ, Margaret AS, May MT, . et al. Global and regional estimates of prevalent and incident herpes simplex virus type 1 infections in 2012. PLoS ONE. 2015; 10( 10): e0140765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Looker KJ, Magaret AS, Turner KME, . et al. Global estimates of prevalent and incident herpes simplex virus type 2 infections in 2012. PLoS ONE. 2015; 10( 1): e114989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Pfister KM, Schleiss MR, Reed RC, . et al. Non-immune hydrops fetalis caused by herpes simplex virus type 2 in the setting of recurrent maternal infection. J Perinatol. 2013; 33( 10): 817– 820. [DOI] [PubMed] [Google Scholar]
- 6. Mercolini F, Verdi F, Eisendle K, . et al. Congenital disseminated HSV-1 infection in preterm twins after primary gingivostomatitis of the mother. Z Gerburtshilfe Neonatol. 2014; 218( 6): 261– 264. [DOI] [PubMed] [Google Scholar]
- 7. Parra J, Cneude F, Huin N, . et al. Mammary herpes: a little known mode of neonatal herpes contamination. J Perinatol. 2013; 33( 9): 736– 737. [DOI] [PubMed] [Google Scholar]
- 8. Pinninti SG, Kimberlin DW.. Management of neonatal herpes simplex virus infection and exposure. Arch Dis Child Fetal Neonatal Ed. 2014; 99( 3): F240– F244. [DOI] [PubMed] [Google Scholar]
- 9. Kotzbauer D, Frank G, Dong W, . et al. Clinical and laboratory characteristics of disseminated herpes simplex virus infection in neonates. Hosp Pediatr. 2014; 4( 3): 167– 171. [DOI] [PubMed] [Google Scholar]
- 10. Long SS, Pool TE, Vodzak J, . et al. Herpes simplex virus infection in young infants during 2 decades of empiric acyclovir therapy. Pediatr Infect Dis J. 2011; 30( 7): 556– 561. [DOI] [PubMed] [Google Scholar]
- 11. Cantey JB, Klein AM, Sanchez PJ.. Herpes simplex virus DNAemia preceding neonatal disease. J Pediatr. 2015; 166( 5): 1308– 1309. [DOI] [PubMed] [Google Scholar]
- 12. Wolfert SI, de Jong EP, Vossen AC, . et al. Diagnostic and therapeutic management for suspected neonatal herpes simplex virus infection. J Clin Virol. 2011; 51( 1): 8– 11. [DOI] [PubMed] [Google Scholar]
- 13. Stanberry LR. Herpes simples virus. : Kliegman RM, Stanton BF, St Geme JW, . et al, eds. Nelson's Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier; 2016. [Google Scholar]
- 14. Curfman AL, Glissmeyer EW, Ahmad FH, . et al. Initial presentation of neonatal herpes simplex virus infection. J Pediatr. 2016; 172: 121– 126. [DOI] [PubMed] [Google Scholar]
- 15. Al Aswad M, Suryadevara M.. Neonatal herpes simplex virus presenting with isolated liver failure. IDCases. 2014; 1( 2): 14– 16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Kimberlin DW, Baley J; Committee on Infectious Diseases; Committee on Fetus and Newborn. . Guidance on management of asymptomatic neonates born to women with active genital herpes lesions. Pediatrics. 2013; 131( 2): e635– e645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Pinninti SG, Kimberlin DW.. Preventing HSV in the newborn. Clin Perinatol. 2014; 41( 4): 945– 955. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Cantey JB, Mejias A, Wallihan R, . et al. Use of blood polymerase chain reaction testing for diagnosis of herpes simplex virus infection. J Pediatr. 2012; 161( 2): 357– 361. [DOI] [PubMed] [Google Scholar]
- 19. Melvin AJ, Mohan KM, Schiffer JT, . et al. Plasma and cerebrospinal fluid herpes simplex levels at diagnosis and outcome of neonatal infection. J Pediatr. 2015; 166( 4): 827– 833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Kimura H, Futamura M, Kito H, . et al. Detection of viral DNA in neonatal herpes simplex virus infections: frequent and prolonged presence in serum and cerebrospinal fluid. J Infect Dis. 1991; 164( 2): 289– 293. [DOI] [PubMed] [Google Scholar]
- 21. Diamond C, Mohan K, Hobson A, . et al. Viremia in neonatal herpes simplex virus infections. Pediatr Infect Dis J. 1999; 18( 6): 487– 489. [DOI] [PubMed] [Google Scholar]
- 22. Foley E, Clarke E, Beckett V, . et al. Management of genital herpes in pregnancy. https://www.rcog.org.uk/globalas-sets/documents/guidelines/management-genital-herpes.pdf. Accessed December 19, 2016.
- 23. ACOG Committee on Practice Bulletins. . ACOG Practice Bulletin: clinical management guidelines for obstetrician-gynecologists: no. 82 June 2007: management of herpes in pregnancy. Obstet Gynecol. 2007; 109( 6): 1489– 1498. [DOI] [PubMed] [Google Scholar]
- 24. Workowski KA, Bolan GA.. Sexually transmitted diseases treatment guidelines 2015. MMWR Recomm Rep. 2015; 64( RR-03): 1– 137. [PMC free article] [PubMed] [Google Scholar]
- 25. Pinninti SG, Angara R, Feja KN, . et al. Neonatal herpes disease following maternal antenatal antiviral suppressive therapy: a multicenter case series. J Pediatr. 2012; 161( 1): 134– 138. [DOI] [PubMed] [Google Scholar]
- 26. Breastfeeding and the use of human milk: American Academy of Pediatrics Section on Breastfeeding. Pediatrics. 2012; 129( 3): e827– e841. [DOI] [PubMed] [Google Scholar]
- 27. VanderPluym C, Tawfik G, Hervas-Malo M, . et al. Empiric acyclovir for neonatal herpes simplex virus infection. J Matern Fetal Neonatal Med. 2012; 25( 8): 1278– 1282. [DOI] [PubMed] [Google Scholar]
- 28. Acosta EP, Flexner C.. Antiviral agents (nonretroviral). : Brunton LL, Chabner BA, Knollmann BC, . Goodman & Gilman's: The Pharmacological Basis of Therapeutics. 12th ed. New York, NY: McGraw-Hill; 2011. [Google Scholar]
- 29. Kimberlin DW, Lin CY, Jacobs RF, . et al. Safety and efficacy of high-dose intravenous acyclovir in the management of neonatal herpes simplex virus infections. Pediatrics. 2001; 108( 2): 230– 238. [DOI] [PubMed] [Google Scholar]
- 30. Kato K, Hara S, Kawada J, Ito Y.. Recurrent neonatal herpes simplex virus infection with central nervous system disease after completion of a 6-month course of suppressive therapy: case report. J Infect Chemother. 2015; 21( 12): 879– 881. [DOI] [PubMed] [Google Scholar]
- 31. Cies JJ, Moore WS, Miller K, . et al. Therapeutic drug monitoring of continuous-infusion acyclovir for disseminated herpes simplex virus infection in a neonate receiving concurrent extracorporeal life support and continuous renal replacement therapy. Pharmacotherapy. 2015; 35( 2): 229– 233. [DOI] [PubMed] [Google Scholar]
- 32. Sampson MR, Bloom BT, Lenfestey RW, . et al. Population pharmacokinetics of intravenous acyclovir in preterm and term infants. Pediatr Infect Dis J. 2014; 33( 1): 42– 49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Kimberlin DW, Whitley RJ, Wan W, . et al. Oral acyclovir suppression and neurodevelopment after neonatal herpes. N Eng J Med. 2011; 365( 14): 1284– 1292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Miller AS, Bennett JS.. Challenges in the care of young infants with suspected neonatal herpes simplex virus. Hosp Pediatr. 2015; 5( 2): 106– 108. [DOI] [PubMed] [Google Scholar]
- 35. Shah SS, Aronson PL, Mohamad Z, . et al. Delayed acyclovir therapy and death among neonates with herpes simplex virus infection. Pediatrics. 2011; 128( 6): 1153– 1160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Allen UD, Robinson JL; Canadian Paediatric Society, Infectious Diseases and Immunization Committee. . Prevention and management of neonatal herpes simplex virus infections. Paediatr Child Health. 2014; 19( 4): 201– 206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Bache M, Andrei G, Bindl L, . et al. Antiviral drug-resistance typing reveals compartmentalization and dynamics of acyclovir-resistant herpes simplex virus type-2 (HSV-2) in a case of neonatal herpes. J Pediatr Infect Dis Soc. 2014; 3( 2): e24– e27. [DOI] [PubMed] [Google Scholar]
- 38. Frobert E, Burrel A, Ducastelle-Lepretre S, . et al. Resistance of herpes simplex viruses to acyclovir: an update from a ten-year survey in France. Antiviral Res. 2014; 111: 36– 41. [DOI] [PubMed] [Google Scholar]
- 39. James SH, Prichard MN.. Current and future therapies for herpes simplex virus infections: mechanism of action and drug resistance. Curr Opin Virol. 2014; 8: 54– 61. [DOI] [PubMed] [Google Scholar]
- 40. Whitley RJ. The use of antiviral drugs during the neonatal period. Clin Perinatol. 2012; 39( 1): 69– 81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Intravenous acyclovir shortage recommendations for pediatrics. http://redbook.solutions.aap.org/selfserve/ssPage.aspx?SelfServeContentId=acyclovir-shortage.November2012. Accessed December 19, 2016.