

Abstract
Segmental colitis associated with diverticulosis (SCAD) is an inflammatory process that affects colonic luminal mucosa in segments that are also affected by diverticulosis. Its prevalence varies between 1.15% and 11.4% amongst those suffering from diverticular disease (DD). Being closely associated with DD, it is slightly commoner in males and usually presents in the sixth decade of life. Although the exact pathogenesis of SCAD is unknown, it is probably heterogeneous and includes mechanisms that also play a part in inflammatory bowel disease (IBD). The clinical presentation is non-specific and similar to that of other pathologies involving the sigmoid colon, and its diagnosis is based on endoscopic findings in correlation with histology. Currently, there are no guidelines for its management, which is usually based on the administration of salicylates and antibiotics, with surgery being reserved for refractory cases. The rarity of SCAD may be multifactorial: whereas milder forms go undiagnosed or are attributed to DD, more severe forms can be misdiagnosed as IBD. This latter distinction is an important one to make, since SCAD and IBD differ as regards their natural history and prognosis, while very often no long-term medications are required in SCAD.
Keywords: Diverticular disease, inflammatory bowel disease, segmental colitis associated with diverticulosis
Introduction
Diverticular disease (DD) is a common condition that is associated with a western lifestyle [1]. Its prevalence increases with age and, depending on the diagnostic methods employed, can be as high as 45% in those over 70 years of age, but it can also affect younger people under 40 years old [2]. Inflammatory bowel disease (IBD) is less common, with the highest reported prevalence in the US and Europe being 0.5% and 0.8% respectively [3]. Whereas IBD’s onset is typically between 20 and 40 years of age, a second peak seen in older age accounts for 10% to 15% of cases [4]. Unsurprisingly, the two conditions often coexist; however, DD may also give rise to complex inflammatory changes of its own that can closely mimic IBD. Diverticular colitis, or segmental colitis associated with diverticulosis (SCAD), has been described as a separate clinical entity for the past few decades, with early reports of a possible association between DD and IBD dating back to the 1960s [5]. Prior to this, DD was only considered as an inflammatory condition when inflammation of a diverticulum (diverticulitis) or adjacent subserosal tissues (peridiverticulitis) was present.
SCAD can be defined as active chronic inflammation in colonic segments affected by DD, namely the occurrence of luminal mucosal inflammation, whether or not there is evidence of inflammation within and/or around the diverticula themselves.
Epidemiology
Given the frequency of diverticulosis, this form of inflammation seems to be comparatively unusual. Because of the general lack of awareness and overlap with other conditions, the exact prevalence of SCAD is difficult to determine. The reported prevalence varies between 0.25% and 1.4% in the general population and 1.15% to 11.4% amongst those suffering from DD. Being closely associated with DD, it is not surprising that the mean age at diagnosis in all of these studies was in the early to mid 60s [6,7]. There also seems to be a slightly higher male preponderance, with one meta-analysis showing that 58.7% of 486 diagnosed cases were men [8]. Whereas the male to female ratio in IBD is similar, gender ratios in DD seem to vary depending on the age group under study, showing a transition from male to female preponderance with increasing age [9,10].
Pathogenesis
The exact pathogenesis of SCAD remains unclear, but it is most likely to be multifactorial. Various potential mechanisms have been described, including mucosal prolapse, fecal stasis, and localized ischemia [11]. Fig. 1 summarizes the interaction of the various proposed pathophysiological mechanisms.
Figure 1.
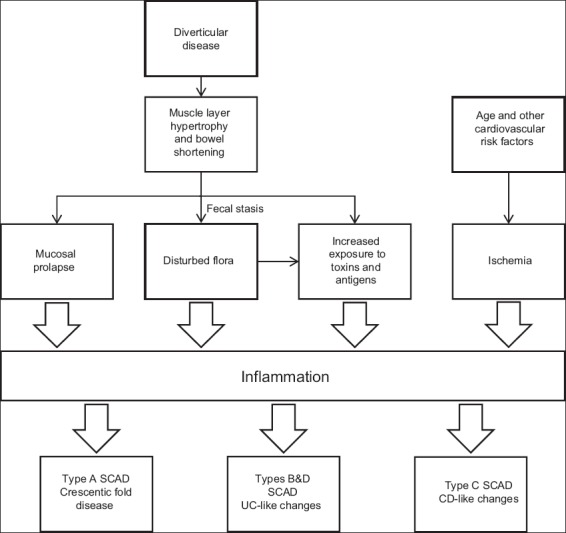
Schematic diagram of pathophysiology in SCAD
SCAD, segmental colitis associated with diverticulosis.
Diverticulosis is accompanied by muscle hypertrophy and bowel shortening, which in turn lead to mucosal redundancy. The pressure effects applied to the excessive mucosa lead to polypoid lesions and inflammatory changes characteristic of mucosal prolapse [12].
Overlap with ulcerative colitis (UC)
By no means can all cases of SCAD be attributed to mucosal prolapse alone, since the pathological changes described can vary from mild non-specific inflammation to intense active inflammation with crypt abscesses, crypt distortion and pronounced chronic inflammation, closely mimicking active chronic UC. Suggested mechanisms for this similarity have included relative ischemia of the sigmoid colon and changes in bacterial flora related to stasis [13]. Areas exposed to fecal stasis, such as the rectum, but also blind-ending structures such as the cecum, are prone to be exposed to increased fecal bacterial mucinase activity. This has been linked to the pathogenesis of UC, but it could also be an underlying mechanism in SCAD, because of the fecal stasis that occurs in diverticular segments [14].
Not only can the condition closely mimic the histological changes of UC, but also SCAD can precede the onset of conventional UC with rectal involvement, although this progression has so far been described only in case reports [15,16]. Further adding to the confusion is the fact that UC with relative rectal sparing has become a fairly recognized entity, though uncommon [17].
Overlap with crohn’s disease (CD)
Whereas clinical evidence suggests that CD and diverticulosis coexist more often than would be expected by chance, pathological evidence suggests otherwise, and this association may in fact be an exaggeration [14]. Older patients diagnosed with CD are more likely to suffer from distal colitis and proctitis rather than the small bowel and proximal large bowel involvement seen in younger patients [18]. CD can also preferentially affect areas of DD, in some patients even giving rise to diverticulitis. At times the distinction between the two is only possible at the time of surgery or on histological examination of the resected specimen [19].
Patients with diverticulosis are generally in an older age group and are likely to have coexistent atheromatous disease. The impact of relative ischemia and changes in bacterial flora due to diverticulosis may cause the CD-like inflammatory response in the sigmoid colon. Indeed, the fact that patients with coexistent DD and CD in surgical case series seem to have a good prognosis, with no evidence of CD recurrence elsewhere, raises the legitimate question of whether a proportion of these patients had DD with pathological mimicry of CD. All three pathological hallmarks of CD, i.e., transmural inflammation, epithelioid cell granulomas and fissuring or fistula formation, can in fact be seen as a result of DD alone. In an effort to make the distinction in individuals suspected of having both CD and DD, the remainder of their gastrointestinal tract should be investigated for evidence of CD elsewhere [20].
Diagnosis and classification
Laboratory investigations (full blood count, erythrocyte sedimentation rate, C-reactive protein, stool inflammatory markers, e.g., calprotectin) and cross-sectional imaging are non-specific and only offer some help in ruling out differentials such as malignancy, and infective or ischemic colitis, since these can present with similar lower gastrointestinal symptoms to SCAD. A thorough drug history is also important in order to rule out colitis due to non-steroidal anti-inflammatory drugs. The mainstay of SCAD diagnosis is endoscopy. The endoscopist needs to inform the pathologist of any index of suspicion based on clinical presentation and endoscopic findings.
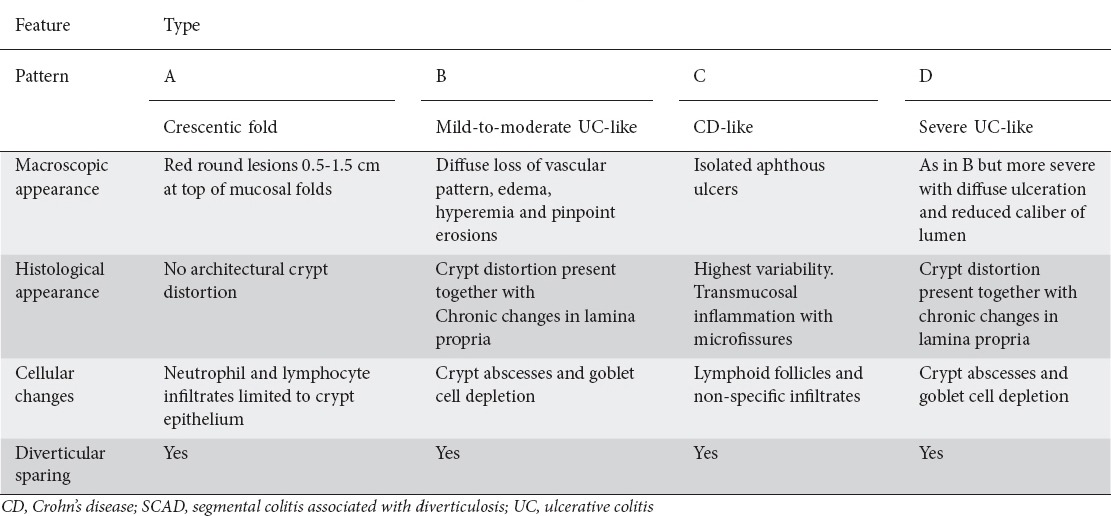
Based on endoscopic features, SCAD has been classified into four different subtypes (Table 1) [21]. In this hallmark study, histological changes correlated well with the different macroscopic findings observed and it is safe to assume that different mechanisms underpin the changes seen in the different categories. Sparing of the diverticular orifices from inflammation is a unifying feature between all SCAD subtypes; this might help distinguish the condition from IBD, especially since all of the histological parameters typically observed in IBD can be present in SCAD, though to a milder extent [22]. Those with a UC-like pattern, i.e. types B and D, have histological changes usually seen in UC with chronic changes in the lamina propria, including basal plasmacytosis, goblet cell depletion, distortion of crypt architecture, cryptitis, crypt abscesses, and crypt hemorrhage. Patients with a CD-like pattern demonstrate the highest intragroup histological variability. Only half of them have the chronic transmucosal inflammation usually associated with CD, the rest having florid lymphoid follicles in the lamina propria and nonspecific inflammatory infiltrates [21]. Even though no patients in this group had noncaseating granulomas, which is one of the hallmarks of CD, this finding alone cannot be used to distinguish between the two, since it is increasingly recognized that histological changes in adult CD can vary greatly, with less than one fourth of newly diagnosed cases having evidence of granulomatous inflammation [23,24].
Table 1.
Segmental colitis associated with diverticulosis subtypes and distinguishing features
Clinical features
SCAD can present with rectal bleeding that is either fresh or altered, chronic diarrhea or cramping abdominal pain, and up to a third of patients have more than one symptom at the time of diagnosis. Systemic features, such as leukocytosis, fever and weight loss, are rare [25]. Whereas diarrhea is commoner in type A disease, patients with type C and D are more likely to experience rectal bleeding. Unlike the relapsing and remitting nature of IBD, the clinical course of SCAD is thought to be more benign, with a significant proportion recovering completely, at times without the need of any treatment and without recurrence [26]. Out of the four categories, types A and C run the most benign course, whereas patients with type B or D SCAD are at a higher risk of relapse. Hence, medical treatment in the latter two subtypes should be strongly considered [27].
Treatment
The optimal treatment for SCAD is still undefined and is largely based on case series and indirect experience from treatment of IBD. First line treatment is usually medical and traditionally this has included the use of antibiotics, salicylates, or a combination of the two together with a high-fiber diet. In contrast to IBD, immunosuppressant medications, including corticosteroids, are rarely required in SCAD [28]. It is the authors’ opinion that if the disease is running an aggressive course with no response to conventional first line therapy, this should raise suspicion of whether one is in fact dealing with a case of misdiagnosed IBD.
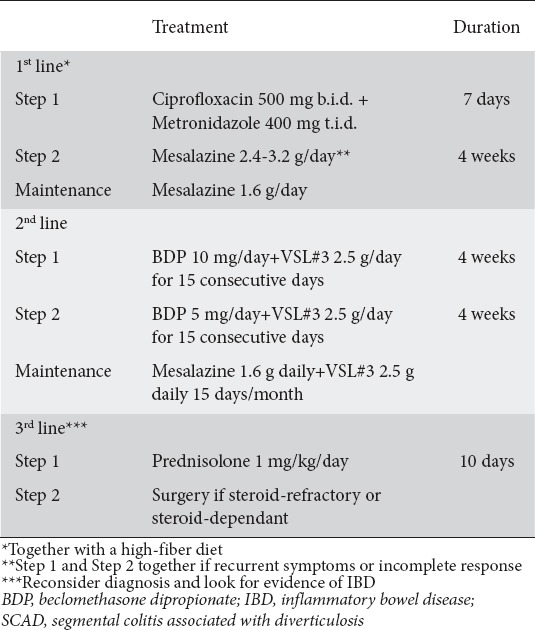
Based on an analysis of 57 patients from the two largest series at the time, Rampton suggested treating patients in whom SCAD is not severe enough to warrant surgery with a first line of high-fiber diet and/or antibiotics such as metronidazole 400 mg t.i.d with ciprofloxacin 500 mg b.i.d for a week. Second-line treatment would then comprise aminosalicylates in conventional doses, as used in IBD [29].
More recently, in a small, open-label and unblinded study that evaluated 12 consecutive patients, Tursi et al concluded that acute mild to moderate diverticular colitis can be treated with a combination of beclomethasone dipropionate (BDP) and the probiotic VSL#3. The treatment regimen consisted of BDP 10 mg/day for 4 weeks and VSL#3 2.5 g/day for 15 consecutive days. This was followed by BDP 5 mg/day for a further 4 weeks plus VSL#3 2.5 g/day for a further 15 days per month. VSL#3 was administered for only 15 days per month, since this is long enough to guarantee persistence of bacteria in the gastrointestinal tract for about 2 weeks after discontinuation of treatment. Results were promising, with 10 patients out of 12 already achieving symptomatic remission at week 4 [30].
In another study by the same author, patients with SCAD were treated with either BDP/VSL#3 or oral mesalazine at 2.4 g/day for 4 weeks, depending on whether they had more (types B and D) or less (types A and C) severe disease subtypes. Maintenance of remission was with mesalazine 1.6 g/day, with the addition of VSL#3 in the former group. Whereas all patients with types A, B and C achieved remission, 3 of 4 patients with type D did not respond to induction and required systemic steroids in the form of prednisolone 1 mg/kg/day for 10 days. Patients with SCAD types B and D were also at a higher risk of relapse [27].
Surgery is usually reserved for cases that are refractory to medical treatment, though it is always possible that these cases represent IBD that was initially misdiagnosed as SCAD [31]. As in IBD, tumor necrosis factor (TNF)-α has been shown to be overexpressed in DD, particularly when inflammation is also present [32]. Even though this means that anti-TNF medications could be used for induction of remission in refractory cases, to date this has only been reported once in the literature [33]. Table 2 summarizes the above information in a stepwise treatment algorithm.
Table 2.
Treatment algorithm for segmental colitis associated with diverticulosis
Concluding remarks
The rarity of SCAD in everyday practice and in the literature probably stems from the fact that milder forms go undiagnosed, whereas more severe forms can be misdiagnosed as IBD or diverticulitis. Increased awareness about the condition and better liaison between the endoscopist and pathologist would help in making an accurate diagnosis more frequently. Even though cases of SCAD misdiagnosed as IBD will probably respond to conventional IBD treatment, it is still important to make the distinction between the two, since the natural history and prognosis of the two conditions vary significantly. Very often, no long-term medications are required in SCAD.
Since most literature on the topic comes from western countries where DD is primarily left-sided, SCAD is usually thought of as inflammation of the sigmoid colon with sparing of the rectum and proximal colon [22]. DD in Asian countries is predominantly right sided; however, there are no data on whether such patients with right colonic diverticulosis are still prone to developing the same patterns of segmental colitis. Contrasting these two populations could lead to a better understanding of the underlying pathogenesis.
Whether SCAD exists as a separate entity or whether it belongs on a spectrum with IBD is still unclear. Cases with overlapping findings, or those with SCAD preceding florid IBD, present an interesting opportunity to better understand the pathogenesis of both conditions. Better understanding of the disease and its optimal management will only be possible with increased awareness amongst clinicians. A multicenter collaboration with prospective patient recruitment would provide a solid basis for further research into the causes, behavior and optimal treatment of this multifaceted disease.
Biography
Mater Dei Hospital, Malta; University of Ioannina, Ioannina, Greece
Footnotes
Conflict of interest: None
References
- 1.Hjern F, Johansson C, Mellgren A, Baxter NN, Hjern A. Diverticular disease and migration—the influence of acculturation to a Western lifestyle on diverticular disease. Aliment Pharmacol Ther. 2006;23:797–805. doi: 10.1111/j.1365-2036.2006.02805.x. [DOI] [PubMed] [Google Scholar]
- 2.Minardi AJ, Jr, Johnson LW, Sehon JK, Zibari GB, McDonald JC. Diverticulitis in the young patient. Am Surg. 2001;67:458–461. [PubMed] [Google Scholar]
- 3.Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142:46–54. doi: 10.1053/j.gastro.2011.10.001. [DOI] [PubMed] [Google Scholar]
- 4.Del Val JH. Old-age inflammatory bowel disease onset: A different problem? World J Gastroenterol. 2011;17:2734–2739. doi: 10.3748/wjg.v17.i22.2734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Schmidt GT, Lennard-Jones JE, Morson BC, Young AC. Crohn’s disease of the colon and its distinction from diverticulitis. Gut. 1968;9:7–16. doi: 10.1136/gut.9.1.7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tursi A. Segmental colitis associated with diverticulosis: complication of diverticular disease or autonomous entity? Dig Dis Sci. 2011;56:27–34. doi: 10.1007/s10620-010-1230-5. [DOI] [PubMed] [Google Scholar]
- 7.Imperiali G, Meucci G, Alvisi C, et al. Segmental colitis associated with diverticula: a prospective study. Gruppo di Studio per le Malattie Infiammatorie Intestinali (GSMII) Am J Gastroenterol. 2000;95:1014–1016. doi: 10.1111/j.1572-0241.2000.01943.x. [DOI] [PubMed] [Google Scholar]
- 8.Mann NS, Hoda KK. Segmental colitis associated with diverticulosis: systematic evaluation of 486 cases with meta-analysis. Hepatogastroenterology. 2012;59:2119–2121. doi: 10.5754/hge11043. [DOI] [PubMed] [Google Scholar]
- 9.Burisch J, Pedersen N, Čuković-Čavka S, et al. EpiCom-group. East-West gradient in the incidence of inflammatory bowel disease in Europe: the ECCO-EpiCom inception cohort. Gut. 2014;63:588–597. doi: 10.1136/gutjnl-2013-304636. [DOI] [PubMed] [Google Scholar]
- 10.Weizman AV, Nguyen GC. Diverticular disease: Epidemiology and management. Can J Gastroenterol. 2011;25:385–389. doi: 10.1155/2011/795241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ludeman L, Shepherd NA. What is diverticular colitis? Pathology. 2002;34:568. doi: 10.1080/0031302021000035974. [DOI] [PubMed] [Google Scholar]
- 12.Kelly JK. Polypoid prolapsing mucosal folds in diverticular disease. Am J Surg Pathol. 1991;15:871–878. doi: 10.1097/00000478-199109000-00007. [DOI] [PubMed] [Google Scholar]
- 13.Gore S, Shepherd NA, Wilkinson SP. Endoscopic crescentic fold disease of the sigmoid colon: the clinical and histopathological spectrum of a distinctive endoscopic appearance. Int J Colorectal Dis. 1992;7:76–81. doi: 10.1007/BF00341290. [DOI] [PubMed] [Google Scholar]
- 14.Shepherd NA. Diverticular disease and chronic idiopathic inflammatory bowel disease: associations and masquerades. Gut. 1996;38:801–802. doi: 10.1136/gut.38.6.801. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hokama A, Kinjo F, Tomiyama R, et al. Progression of diverticular colitis to ulcerative colitis. Inflamm Bowel Dis. 2005;11:618. doi: 10.1097/01.mib.0000163950.16112.61. [DOI] [PubMed] [Google Scholar]
- 16.Maeshiro T, Hokama A, Kinjo T, Fujita J. Diverticular colitis of the ascending colon preceding the onset of ulcerative colitis. BMJ Case Rep 2014. 2014 doi: 10.1136/bcr-2014-204361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Robert ME, Skacel M, Ullman T, Bernstein CN, Easley K, Goldblum JR. Patterns of colonic involvement at initial presentation in ulcerative colitis: a retrospective study of 46 newly diagnosed cases. Am J Clin Pathol. 2004;122:94–99. doi: 10.1309/XLXK-J84C-3JCW-3RCH. [DOI] [PubMed] [Google Scholar]
- 18.Berman IR, Corman ML, Coller JA, Veidenheimer MC. Late onset Crohn’s disease in patients with colonic diverticulitis. Dis Colon Rectum. 1979;22:524–529. doi: 10.1007/BF02586997. [DOI] [PubMed] [Google Scholar]
- 19.Meyers MA, Alonso DR, Morson BC, Bartram C. Pathogenesis of diverticulitis complicating granulomatous colitis. Gastroenterology. 1978;74:24–31. [PubMed] [Google Scholar]
- 20.Shepherd NA. Pathological mimics of chronic inflammatory bowel disease. J Clin Pathol. 1991;44:726–733. doi: 10.1136/jcp.44.9.726. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Tursi A, Elisei W, Brandimarte G, et al. The endoscopic spectrum of segmental colitis associated with diverticulosis. Colorectal Dis. 2010;12:464–470. doi: 10.1111/j.1463-1318.2009.01969.x. [DOI] [PubMed] [Google Scholar]
- 22.Tursi A, Inchingolo CD, Picchio M, Elisei W, Mangiola F, Gasbarrini G. Histopathology of segmental colitis associated with diverticulosis resembles inflammatory bowel diseases. J Clin Gastroenterol. 2015;49:350–351. doi: 10.1097/MCG.0000000000000268. [DOI] [PubMed] [Google Scholar]
- 23.Rubio CA, Orrego A, Nesi G, Finkel Y. Frequency of epithelioid granulomas in colonoscopic biopsy specimens from paediatric and adult patients with Crohn’s colitis. J Clin Pathol. 2007;60:1268–1272. doi: 10.1136/jcp.2006.045336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Freeman HJ. Granuloma-positive Crohn’s disease. Can J Gastroenterol. 2007;21:583–587. doi: 10.1155/2007/917649. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Harpaz N, Sachar DB. Segmental colitis associated with diverticular disease and other IBD look-alikes. J Clin Gastroenterol. 2006;40(Suppl 3):S132–S135. doi: 10.1097/01.mcg.0000225505.67547.90. [DOI] [PubMed] [Google Scholar]
- 26.Freeman HJ. Natural history and long-term clinical behavior of segmental colitis associated with diverticulosis (SCAD syndrome) Dig Dis Sci. 2008;53:2452–2457. doi: 10.1007/s10620-007-0173-y. [DOI] [PubMed] [Google Scholar]
- 27.Tursi A, Elisei W, Giorgetti GM, et al. Segmental colitis associated with diverticulosis: a 5-year follow-up. Int J Colorectal Dis. 2012;27:179–185. doi: 10.1007/s00384-011-1296-3. [DOI] [PubMed] [Google Scholar]
- 28.Koutroubakis IE, Antoniou P, Tzardi M, Kouroumalis EA. The spectrum of segmental colitis associated with diverticulosis. Int J Colorectal Dis. 2005;20:28–32. doi: 10.1007/s00384-004-0615-3. [DOI] [PubMed] [Google Scholar]
- 29.Rampton DS. Diverticular colitis: diagnosis and management. Colorectal Dis. 2001;3:149–153. doi: 10.1046/j.1463-1318.2001.00242.x. [DOI] [PubMed] [Google Scholar]
- 30.Tursi A, Brandimarte G, Giorgetti GM, Elisei W. Beclomethasone dipropionate plus VSL#3 for the treatment of mild to moderate diverticular colitis: an open, pilot study. J Clin Gastroenterol. 2005;39:644–645. doi: 10.1097/01.mcg.0000170741.82004.70. [DOI] [PubMed] [Google Scholar]
- 31.Imperiali G, Terpin MM, Meucci G, Ferrara A, Minoli G. Segmental colitis associated with diverticula: a 7-year follow-up study. Endoscopy. 2006;38:610–612. doi: 10.1055/s-2006-924985. [DOI] [PubMed] [Google Scholar]
- 32.Ierardi E, Meucci G, Hassan C, et al. Tumour necrosis factor alpha in segmental colitis associated with diverticula. Dig Dis Sci. 2008;53:1865–1868. doi: 10.1007/s10620-007-0086-9. [DOI] [PubMed] [Google Scholar]
- 33.Hassan C, Zullo A, Ierardi E, Burattini O, De Francesco V, Morini S. Tumour necrosis factor alpha downregulation and therapeutic response to infliximab in a case of segmental colitis associated with diverticula. Gut. 2006;55:589–590. doi: 10.1136/gut.2005.084756. [DOI] [PMC free article] [PubMed] [Google Scholar]