

Abstract
Extracorporeal shockwave therapy (ESWT) is a new non-invasive method to induce tissue regeneration and repair the damaged osteoarthritis (OA) of knee. Previous studies suggested subchondral bone as the key target for OA treatment. However, the relationship of the effect and different locations of subchondral bone is unknown. The purpose of the study was to investigate whether the subchondral bone of medial tibia as the target for ESWT in early OA knee treatment and compared with various locations on lateral tibia and femur condyles. Application of ESWT on the medial tibial subchondral bone ameliorated 38% in gross pathological OA changes (compared to OA, P < 0.001), 94 % in OARSI score (compared to OA, P < 0.001) and 45% in cartilage defect (compared to OA, P < 0.001), 17% in bone mineral density (compared to OA, P < 0.001) than lateral tibia and femur. In micro-CT analysis, ESWT on medial tibial subchondral bone increased bone volume (61% vs 44% in tibia and 62% vs 53% in femur, P < 0.05), yield stress (6 MPa vs 4 MPa in tibia and 4 MPa vs 2 MPa in femur, P < 0.05) and decreased bone porosity (38% vs 53% in tibia and 37% vs 46% in femur, P < 0.05) than OA. The TUNEL, PCNA and osteocalcin significantly influenced the levels of molecular expression in different locations of ESWT application. Our results confirm that application of ESWT to the medial tibial subchondral bone has more effective therapy for OA knee than lateral locations of joint knee.
Keywords: Shockwave, media tibia, subchondral bone, cartilage, osteoarthritis
Introduction
The pathophysiological changes of osteoarthritis of the knee can occur in synovial fluid, joint capsule, subchondral bone, and other joint tissues [1,2]. Synovial inflammation plays an important role in OA knee, particularly in the early stage [3]. As osteoarthritis progresses, the level of proteoglycans decreases, and results in softening of the cartilage, decreased elasticity and further compromising joint surface integrity osteoarthritic joint [4]. The loss of cartilage results in narrowing of joint space. Erosion of the damaged cartilage causes the underlying bone is exposed as osteoarthritic joint progresses. Continuously, the subchondral bone responses with vascular invasion and increases cellularity to becoming eburnation at pressure area. Finally, the damaged subchondral bone may undergo cystic degeneration, which is caused from osseous necrosis or the intrusion of synovial fluid [5]. Until now, there is no cure for osteoarthritis, although treatments can reduce pain and improve joint movement.
As previous description, osteoarthritis joint is a progressive in cartilage loss and joint space narrowing [3]. The central pathological feature of OA has long been considered a cartilage disease that involves in the destruction and loss of articular cartilage [6-9]. However, It is now accepted that the whole knee is involved, including synovial inflammation, cartilage damage and subchondral bone alterations [10]. Recently, the role of subchondral bone in the pathophysiology of the disease has been suggested in some studies that subchondral sclerotic bone increases in OA changes and is associated with the disease progression [7,11,12]. According to the animal model of osteoarthritis, the subchondral bone remodeling level has been significantly emphasized [13]. These observations suggested a role of subchondral bone changes to regulate cartilage metabolism. It may be a critical therapeutic target to control the initiation and progression of osteoarthritic changes of the knee [11,14-17].
ESWT is a new, noninvasive treatment modality for musculoskeletal disorders. The Food and Drug Administration (FDA) of the Unite States had approved ESWT to treat pain on heels and muscles in the year 2000 [18]. Recently, ESWT was reported to have prevention, improvement and regression in osteoarthritis of various joints in animals and human studies [19-24]. ESWT can be the most effective treatment for osteoarthritis. Our previous study demonstrated that ESWT had chondroprotective effects in the OA knee [25]. We also showed that established OA changes regressed after ESWT in knee of the rats [26]. In addition, the site-specific effects of ESWT were demonstrated in OA rat knees [27]. In this study, we applied ESWT on the medial tibia condyle of the knee for the treatment of OA disease in animal model. However, we still did not know which location of OA knee was the best target for ESWT application.
In the present study, we compared the effectiveness of ESWT on medial tibia condyle and the lateral tibia and femur locations of OA knee. Furthermore, we found that ESWT application on lateral tibia and femur sites of knee did not prevent the cartilage and bone damage in OA rats. The purpose of our study was to investigate the best target site of OA knee for ESWT in the initiation of osteoarthritic changes of the knee in animal model.
Material and methods
Study design
The fifty-six 8-week-old Sprague-Dawley rats were purchased and used in the study (from BioLASCO, Taipei, Taiwan). The rats were housed at 23 ± 1°C with a 12 h light and dark cycle and were given food and water at the Center for Laboratory Animals in Kaohsiung Chang Gung Memorial Hospital. The Animal Care Committee of the Center for Laboratory Animals in Kaohsiung Chang Gung Memorial Hospital approved this IACUC protocol of animal study followed guidelines for the use of animals in the laboratories abiding by the principles of 4 R’s (replacement, reduction, refinement and rehabilitation). The IACUC chairperson is Professor Yur-Ren Kuo and reference number is 2012041001.
Following was the study designs and the experiments (Figure 1A, 1B). The rats were randomly divided into seven groups with 8 rats in each group (Figure 1A). Group 1 was the sham that received sham arthrotomy of left knee without anterior cruciate ligament transection (ACLT) and medial meniscectomy (MM). Group 2 was the OA that received ACLT and MM of left knees, but without ESWT. Group 3 was the T(M) group that received ACLT and MM of left knee and treated with ESWT to medial (M) tibia (T) condyle. Group 4 was the F(L) group that received ACLT and MM of left knee and treated ESWT to distal lateral (L) femur (F) condyle. Group 5 was the T(L) group that received ACLT and MM of left knee and treated ESWT to the proximal lateral tibia plateaus. Group 6 was the F+T(L) group that received ACLT and MM of left knee and treated ESWT to proximal lateral tibia plateaus and distal lateral femur condyles. Group 7 was the F(M+L) group that received ACLT and MM of left knee and treated ESWT to medial and lateral femur.
Figure 1.
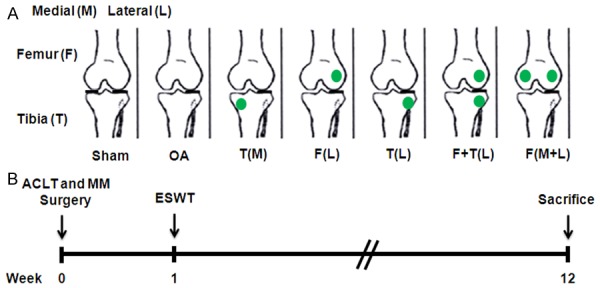
The locations of shockwave application and the study design. A. The knee sketch outlined the locations (green color dots) of shockwave application in different groups of animals (n = 8 in each groups). B. Graphic scheme depicted the study design of the experiment including knee surgery, shockwave application and sacrifice of animals.
Anterior cruciate ligament transection and medial meniscectomy
In order to create an OA model, the left knee of rat was transected with a scalpel by using medial parapatellar mini-arthrotomy, the anterior cruciate ligament. Then medial meniscectomy was performed through removing the entire medial meniscus. The knee joint was irrigated and the incision was closed. Prophylactic antibiotics with ampicillin 50 mg/Kg were given for 5 days after surgery. Postoperatively, a veterinarian cared for the animals. We observed the surgical site and the activities of all animals every day.
Shockwave application
The dose was optimized for ESWT on OA knee of rats as in previous studies [25-27]. In ESWT groups [T(M), F(L), T(L), F+T(L) and F(M+L)], ESWT was applied when the surgical wound healed at 1 week after surgery. The animals were anesthetized with 1:1 volume mixture of Rompun (5 mg/kg) and Zoletil (20 mg/kg) while receiving ESWT. Ultrasound guide (Toshiba Medical Systems Corporation, Tokyo, Japan) was used for localizations of ESWT application. The source of shockwave was from an OssaTron (Saunwave, Alpharetta, GA). Application of 800 impulses of shockwave at 0.22 mJ/mm2 energy flux density was given to the assign locations as described above. After ESWT, the animals were returned to the housing cage and were cared for by a veterinarian. The animals were euthanized at 12 weeks and the harvested knee specimens were examined and analyzed.
Gross pathological analysis
The gross pathological findings of OA changes of the knee (n = 8) were observed and semi-quantified by magnification scope (Carl Zeiss, Oberkochen, Germany). The severity of joint-surface damage was categorized and scored as follows: (a) Intact surface or normal appearance = 0 point, (b) rough surface with minimal fibrillation or a slight yellowish discoloration = 1 point, (c) cartilage erosion extending into superficial or middle layers = 2 points, (d) cartilage erosion extending into the deep layers = 3 points, (e) complete cartilage erosion with subchondral bone exposed = 4 points [28].
OARSI scores and cartilage degradation
The degenerative changes of the cartilage were stained with Safranin O and scored with the Osteoarthritis Research Society International (OARSI) cartilage OA grading system [29]. The scores were obtained on a 0 to 24 scale by multiplying the index of grade and stage. For cartilage area measurement, eight non-consecutive sections at 100 μm intervals were measured per knee joint. The whole cartilages were delimited and area was automatically calculated by ImageJ software [30].
Bone mineral density
The bone mineral density (BMD) with region of interest in medial proximal tibia and distal femur condyle was performed using dual energy X-ray absorptiometry (Hologic QDR 4500W, Hologic, Bedford, MA) to scan in all knees before the animals were sacrificed. BMD was used to assess the changes in bone density around the knee in different conditions.
Micro-CT analysis
The proximal part of tibia and distal part of femur were scanned by a micro-CT scanner (Skyscan 1076; Skyscan, Luxembourg, Belgium) with isotropic voxel size of 36 × 36 × 36 μm3 as previously described [31,32]. In brief, the X-ray voltage was set at 100 kV, and the current, at 100 μA. X-ray projections were obtained at 0.75 degrees angular step with a scanning angular range of 180 degrees. Reconstructions of the image slices were performed with NRecon software (Skyscan), and the process generated a series of planar transverse gray value images. Skyscan CT-Analyser Software (Skyscan) selected volume of interest (VOI) of bone morphometry with a semiautomatic contouring method. Three-dimensional cross-sectional images were generated by CTVol v2.0 software (Skyscan). The micro-CT parameters of percentage in bone volume and porosity, trabecular thickness and number in subchondral compartment regions were determined [31,32].
Mechanical compression tests
The block specimens containing cartilage and trabecular bone were excised from the central weight-bearing regions of medial femur condyles and tibia plateaus according to previous methods with little modification [32,33]. In brief, the bones were excised marked and cut into blocks by a bone cutter (Roboz, Gaithersburg, MA, USA) and trimmed by an electric grinder pen (Chi-tai Inc., Kaohsiung, Taiwan) at the volume of 105 mm3 (7 mm for length × 3 mm for width × 5 mm for height) were subjected to the mechanical compression test. The osteochondral blocks were placed between the upper and lower platens until crash and then analyzed by a compression test machine and the upper plate was set to move at strain rate at 0.5 per min. (MTS, Synergie 200, Eden Prairie, MN, USA) and the yield stress (MPa) of bone blocks were determined by the associated software (TestWorks4, MTS).
Immunohistochemical analysis
The harvested knee specimens were fixed in 4% PBS buffered formaldehyde for 48 hours and decalcified in 10% PBS-buffered EDTA solution. Decalcified tissues were embedded in paraffin wax. The specimens were cut longitudinally into 5-μm-thick sections and transferred to polylysine-coated slides (Thermo Fisher Scientific, Waltham, MA, USA). The TUNEL analysis was accomplished by In Situ Cell Death Detection Kits (Roche Diagnostic, Mannheim, Germany) followed by a manufacture instruction provided. TUNEL color stains were performed by using NBC/BCIP substrate (Sigma-Aldrich, St. Louis, MO, USA). The immunohistochemical stains were done by following the protocol provided in the immunostaining kit (Abcam, Cambridge, MA, USA). In brief, tissue sections were deparaffinized in xylene, hydrated in graded ethanol, and treated with peroxide block and protein-block reagents. Sections of the specimens were immunostained with specific antibodies for PCNA (Thermo Fisher) at 1:300 dilution and osteocalcin (GeneTax, Irvine, CA, USA) at 1:200 for overnight to identify the cell proliferation and osteogenesis biomarkers. The immunoreactivity in specimens was demonstrated by using a goat anti-rabbit horseradish peroxidase-conjugated and 3’,3’-diaminobenzendine, which were provided in the kit. The immunoactivities were quantified from five random areas in three sections of the same specimen by using a Zeiss Axiolmager M2 microscope (Carl Zeiss, Gottingen, Germany). All images of each specimen were captured by using a cool CCD camera (Media Cybernetics, Silver Spring, MD, USA). Images were analyzed by manual counting and confirmed by using an Image-Pro Plus image-analysis software (Media Cybernetics).
Statistical analysis
SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) was used in statistical analysis. Data were expressed as mean ± SD. One-way ANOVA and Tukey tests were used to compare sham versus T(M), F(L), T(L), F+T(L) and F(M+L) (designated as *P < 0.05 and **P < 0.001). One-way ANOVA and Tukey tests were also used to compare OA versus T(M), F(L), T(L), F+T(L) and F(M+L) (designated as #P < 0.05 and ##P < 0.001). The intra-group evaluations of T(M) versus F(L), T(L), F+T(L) and F(M+L) were determined by Student -t Test (designated as ※※P < 0.05 and ※※P < 0.001).
Results
ESWT improves the pathologic lesions
The gross pathology and pathological lesion score were measured in the experiments (Figure 2). Photographs of the knee showed macroscopic pathological osteoarthritic lesions of distal femur and proximal tibia for pathological analysis (Figure 2A). The results showed that all ESWT groups had significantly different lesion scores as compared to sham (P < 0.001). Whereas T(M) and F(M+L) had significantly better scores as compared with OA (2.000 ± 0.201 and 2.244 ± 0.169 vs 3.219 ± 0.140, P < 0.001) than other locations (2.844 ± 0.169 to 3.156 ± 0.156, without significant). In ESWT groups, the graphic illustrations of T(M) group showed significantly lower lesion scores as compared to other ESWT groups (Figure 2B). The results indicated that ESWT on T(M) (2.000 ± 0.201, P < 0.001) position which was major in subchondral bone of medial tibia reduced lesions formation and tissue damage than F(L) (3.156 ± 0.156), T(L) (3.094 ± 0.158), F+T(L) (2.844 ± 0.169) and F(M+L) (2.244 ± 0.169) in OA knee.
Figure 2.
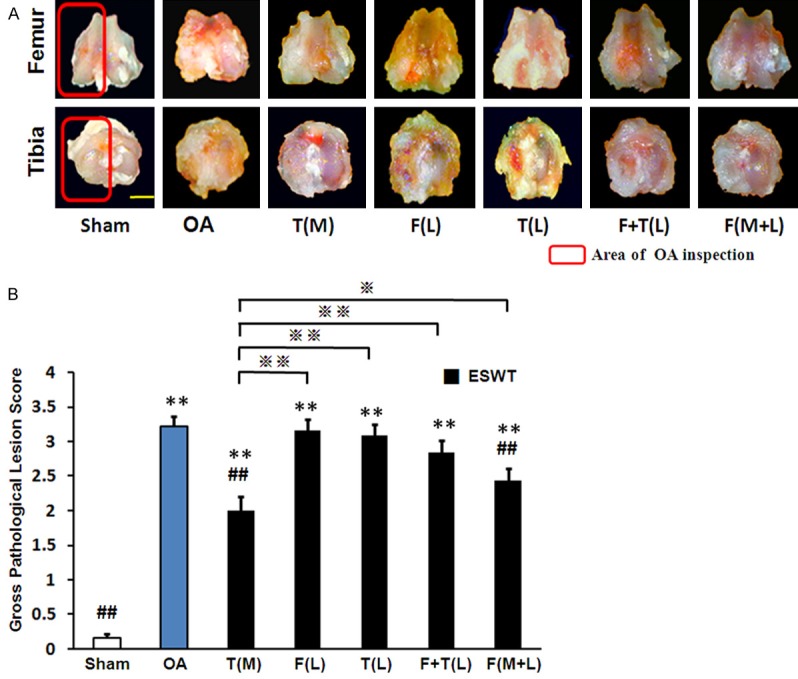
The photographs showed macroscopic pathological osteoarthritic lesions of knee including the areas of osteophyte formation. A. The knee photos demonstrated the gross pathological osteoarthritic lesions in distal femur and proximal tibia. The scale bar represented 5 mm. B. the panel showed the gross pathological lesion score. The T(M) group showed significantly lower lesion scores as compared to OA and other ESWT groups. Red rectangle indicated OA inspection. **P < 0.001 compared with sham. #P < 0.05, ##P < 0.001 compared with OA. ※P < 0.05, ※※P < 0.001 compared with T(M). All rats were n = 8.
Comparing cartilage degeneration and subchondral bone changes after shockwave treatment on different locations of knee
Articular cartilage degeneration is an important progression in the OA disease. We measured the level of cartilage lesions after ESWT on different treated locations of OA knee. We surveyed the cartilage injuries by OARSI score and sectional cartilage area (Figure 3). The surface of articular cartilage and change of subchondral bone were compared in sham, OA and ESWT groups after shockwave treatment on different locations (Figure 3A). The cartilage damage, subchondral bone loss and cyst formation were obviously in OA, F(L), T(L) and F+T(L) groups by Safranin-O staining. We used OARSI score system and cartilage area assessment to measure the damage of cartilage in OA knee after shockwave treatment (Figure 3B, 3C). The T(M) and F(M+L) groups were low OARSI score (1.188 ± 0.834 and 5.583 ± 2.577 vs 18.751 ± 4.158 and 0.250 ± 0.463, P < 0.001) and increase in cartilage area (0.588 ± 0.140 and 0.659 ± 0.118 vs 0.228 ± 0.143 and 0.847 ± 0.076, P < 0.001) as compared to OA and sham groups. Therefore, ESWT on T(M) and F(M+L) reduced cartilage degeneration, bone loss and cyst formation than other sites of OA knee.
Figure 3.
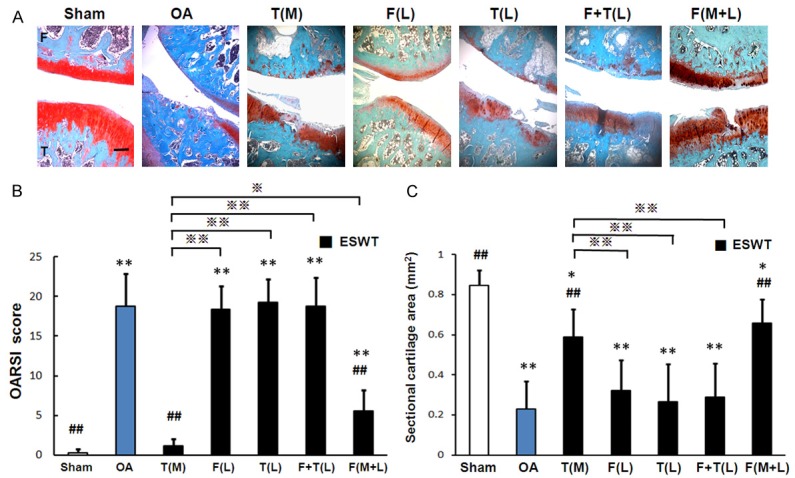
The microphotographs of the knee showed cartilage degradation of the knee in different groups. A: Microphotographs of cartilage and subchondral bone demonstrated cartilage damage in OA changes. The scale bar represented 200 μm. B and C: Showed graphic illustrations of OARSI score and cartilage area in histopathological examination. The T(M) and F(M+L) groups showed significant decrease in OARSI score and increase in cartilage area as compared with sham, OA and other ESWT groups. *P < 0.05, **P < 0.001 compared with sham. #P < 0.05, ##P < 0.001 compared with OA. ※P < 0.05, ※※P < 0.001 compared with T(M). All rats were n = 8.
Micro-CT and BMD analysis by ESWT in early OA of rat joint
In order to observe the changes of subchondral bone at the onset of sham, OA, and OA with various locations by shockwave, micro-CT scan were proceed on distal femur and proximal tibia in different groups (Figure 4A). The transverse planes of distal femur and proximal tibia were used to monitor the actual situation of bone remodeling by micro-CT examinations (Figure 4A). The fractured bone and cyst formation were observed in OA, F(L), T(L) and F+T(L) groups in femur and tibia, however, the data were in contrast with T(M) and F(M+L). The edges of bone became thicker in distal femur but were not in proximal tibia in all ESWT groups.
Figure 4.
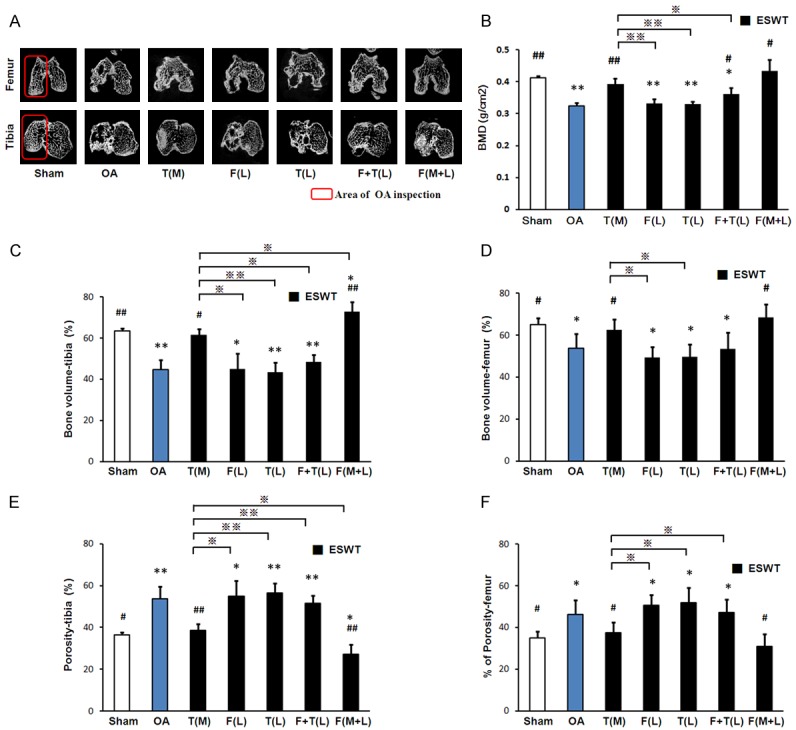
Micro-CT scan of distal femur and proximal tibia and BMD measuring in different groups. A: The result showed photomicrographs of the knee in sagittal and transverse views from micro-CT. The subchondral bone medial compartment of each group was marked (red box). The scale bar represented 1 mm and rats n = 8. B: The BMD values were measured from the region of interest in knee. C-F: Showed the graphic illustrations of bone volume and bone porosity of tibia and femur in different groups. T(M) and F(M+L) groups showed significant increases in bone volume, and decrease in bone porosity as compared with sham, OA and other ESWT groups. *P < 0.05, **P < 0.001 compared with sham. #P < 0.05, ##P < 0.001 compared with OA. ※P < 0.05, ※※P < 0.001 compared with T(M). All rats were n = 8.
Further, BMD was measured from each experimental group by DEXA scan at 12 weeks after ESWT (Figure 4B). BMD was significantly improved in T(M) and F(M+L) groups (0.393 ± 0.018 and 0.434 ± 0.035, P < 0.001) comparing with OA in contrast to a decrease in groups of OA, F(L), T(L) and F+T(L) comparing with sham (0.325 ± 0.01, 0.333 ± 0.013, 0.329 ± 0.009, 0.362 ± 0.019 vs 0.413 ± 0.005, P < 0.001 and P < 0.05). Using the pair sample t test analysis, BMD was significantly higher on T(M) and F(M+L) positions after ESWT than ESWT on F(L), T(L) and F+T(L) positions. It showed that shockwave treatment on T(M) and F(M+L) positions improved BMD significantly.
The locations of ESWT application affected the subchondral bone changes
The graphic illustrations of bone volume and bone porosity in different groups were shown in Figure 4C-F. T(M) and F(M+L) groups (P < 0.05) showed significant increase in bone volume and decrease in bone porosity as compared to sham and OA groups in tibia and femur. Notable, the area of sclerotic bone lesion in F(M+L) group was larger than T(M) group (Figure 4A). Amongst ESWT groups, T(M) and F(M+L) groups demonstrated the most striking changes than other groups in subchondral bone and suppressed aberrant bone formation. The results indicated that ESWT on T(M) and F(M+L) locations improved the subchondral bone remodeling and ameliorated the bone damage.
The bone strength in subchondral bone improvement by ESWT
ESWT improved the bone volume and bone microstructure to maintain the bone architecture. The bone strength was measured and compared after ESWT on different treated locations of OA knee (Figure 5). In bone strength test, the yield stress (Figure 5A, 5B) of the femur (2.766 ± 0.791, 2.658 ± 0.677, 2.986 ± 0.674, 3.173 ± 0.795 and 4.269 ± 0.575, 5.287 ± 0.581 vs 4.712 ± 0.606, P < 0.05 and without significant) and tibia (4.317 ± 0.689, 4.062 ± 0.631, 4.037 ± 0.499, 4.287 ± 0.653 and 6.018 ± 0.604, 6.555 ± 0.826 vs 5.741 ± 0.367, P < 0.05 and without significant) significantly decreased in OA, F(L), T(L) and F+T(L) but increasing in T(M) and F(M+L) relative to sham. Amongst ESWT groups, T(M) and F(M+L) significantly improved the yield stress than other groups. Further, the bone strength of F(M+L) was significantly better than T(M) in femur (P < 0.05) but no difference as noticed in tibia. Our data demonstrated that ESWT can improve architectural changes and apparent-level strength of subchondral bone in OA knee after ESWT on T(M) and F(M+L) positions.
Figure 5.
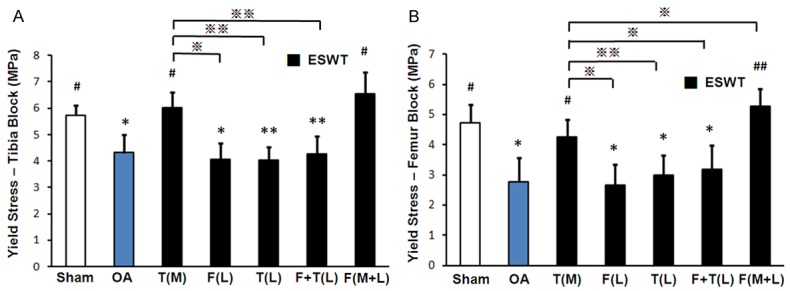
Bone strength tests included load at yield and yield stress of inertia with ESWT. The yield stress of inertia in tibia (A) and femur (B) demonstrated significantly higher values in T(M) and F(M+L) groups than OA and other ESWT groups. *P < 0.05, **P < 0.001 compared with sham. #P < 0.05, ##P < 0.001 compared with OA. ※P < 0.05, ※※P < 0.001 compared with T(M). n = 8.
The lateral locations for application of ESWT influence the expression of favorable factors
Immunohistochemical analysis of TUNEL and PCNA were shown in subchondral bone and cartilage as well as osteocalcin measured in subchondral bone from femur and tibia in groups of sham, OA, and OA with various treatment sites by ESWT (Figure 6). The representative images of microscopic features (right) and quantification (left) were shown in Figure 6. TUNEL activity was significantly decreased after ESWT in T(M) groups (13.97 ± 4.121, P < 0.001) rather than F(M+L) group (39.144 ± 6.589), OA (80.335 ± 7.675) and ESWT groups (78.172 ± 10.558, 76.008 ± 13.452 and 74.308 ± 12.478) (Figure 6A). The PCNA and osteocalcin were dramatically increased in the T(M) and F(M+L) groups (PCNA: 56.941 ± 8.403 and 18.499 ± 10.649, P < 0.001 and P < 0.005; osteocalcin: 20.637 ± 1.290 and 28.648 ± 1.191, P < 0.001 and P < 0.05) as compared to sham, OA and other ESWT groups (Figure 6B, 6C). The effectiveness of lateral locations for application of ESWT were not satisfying than T(M). These results suggested that correct location for ESWT application was very important in modulation and promotion of the key factors for joint repair in OA knee.
Figure 6.
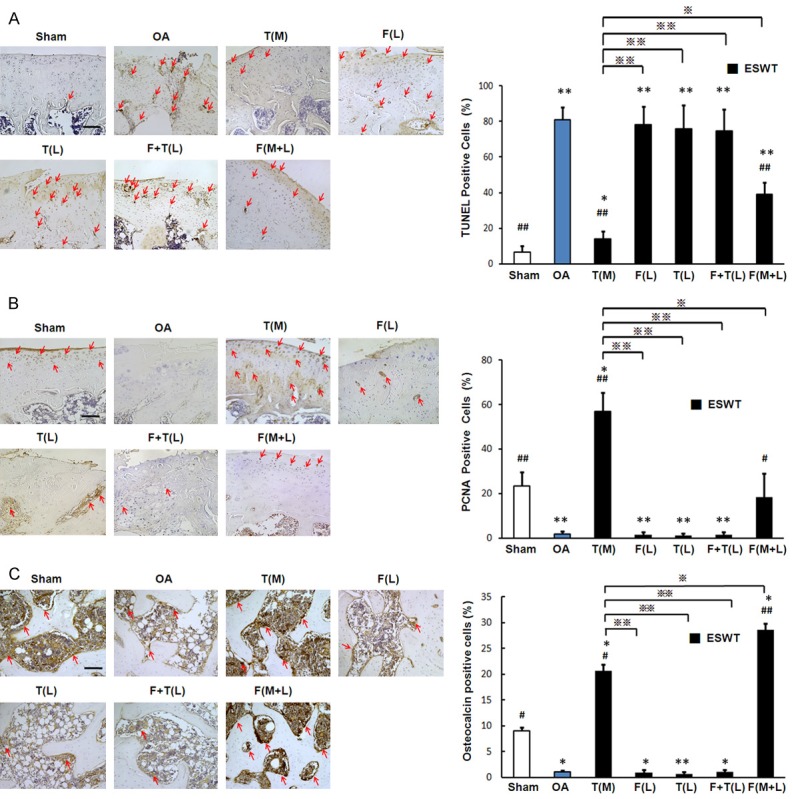
Immunohistochemical analysis for molecular changes on lateral locations by ESWT. Immunohistochemical stains (left) and quantification (right) were showed the effect of TUNEL assay (A) and the expression levels of PCNA (B) and osteocalcin (C) after ESWT on different locations. TUNEL and PCNA were surveyed in cartilage and subchondral bone as well as osteocalcin was surveryed in subchondral bone from femur and tibia. *P < 0.05, **P < 0.001 compared with sham. #P < 0.05, ##P < 0.001 compared with OA group. ※P < 0.05, ※※P < 0.001 compared with T(M). The red arrowhead indicated the expression pattern. The scale bar for TUNEL and PCNA are 50 μm and osteocalcin is 200 μm. All rats were n = 8.
Discussion
The present study demonstrated that subchondral bone was the key target to regulate the inflammatory, bone remodeling, cartilage protection and metabolic markers in response to ESWT in OA knee. We compared the effects on medial tibial subchondral bone to other laterial locations of joint with ESWT on OA treatment. To the best of our knowledge, these findings are the first to document the detailed site specific effects of ESWT in vivo. Pathological and biological responses of ESWT on different locations of knee provide a novel insight into the changes of cartilage and bone remodeling as well as mechanisms underlying the effect of ESWT when it is used for OA knee.
For many years, researchers hypothesized that subchondral bone may play an important role in the development of OA pathology [14]. Prior studies demonstrated that the changes in subchondral bone characteristics might play an important role in the development of osteoarthritis of the knee [14,16,34]. Other studies emphasized the fact that subchondral bone might be the main target for treatment of pain and disease progression in osteoarthritis knee [17]. The results of the current study showed that application of shockwave to the subchondral bone was effective to ameliorate the knee from developing osteoarthrisis of the knee after ACLT and MM in rats. Furthermore, application of ESWT to the subchondral bone of the medial tibia condyle of the knee resulted in the most chondroprotective effects as compared to other locations that may prevent the knee from developing osteoarthritis in ACLT and MM animal knee models.
The major findings in this study confirmed that ESWT is chondroprotective, and the effects appear to be treatment location sensitive. Overall, application of ESWT to the medial tibia showed the best chondroprotective results as compared to other locations of the knee in this experiment. The results of this study were in agreement with the previous studies that ESWT could effectively ameliorate the progress of early osteoarthritis in correct location of knee [25,32,35-37]. However, the exactly location-sensitive effects of ESWT in osteoarthritis of the knee were not previously reported. Our findings provided the basic data in the use of animal model in research and offer the guidance in clinical application when ESWT was chosen for knees with early osteoarthritis.
Bone remodeling and homeostasis are the key progress in OA disease and treatment [38]. In the current study, we observed that ESWT regulated the bone volume and porosity in subchondral bone as well as correlated with the expression of osteocalcin from various locations. The bone mineral homeostasis of T(M) group is the better than F(M+L) group and others comparing with sham. However, it is unknown how different locations of ESWT application influence to bone homeostasis. More evidences suggested that numerous factors are involved in the maintenance of bone homeostasis including growth factors, humoral factors, cytokines, osteoblast and osteoclast [39-41]. Many factors are reported to induce by ESWT after treatment in osteogenic factors such as TGF-β, IGF1, BMP2, osteocalcin, and alkaline phosphatase [42].
The exact mechanism of ESWT remains unknown. Prior studies showed that ESWT may act as a mechanotransduction that produced biological responses to the target tissues by stimulation of the ingrowth of neovascularization, that in turn, results in tissue regeneration and repair such as osteoarthritis of the knee [43]. Other studies also reported that ESWT reduced pain and improved function of the knee by suppression of substance P positive nerve fibers from dorsal neuron ganglion to the knee and calcitonin-gene related peptide around the knee [20]. The results of the current study confirmed that application of ESWT to the subchondral bone of the medial tibia yields the most effects in the initiation of osteoarthritis of the knee.
ESWT is effective for knee osteoarthritis prevention. In our current study, the effects of ESWT application on the medial tibia of subchondral bone was better than lateral and other locations in early OA knee of rat. ESWT on subchondral bone significantly improved cartilage damage area, BMD value, bone microarchitecture and bone strength. ESWT also reduced apoptosis, increased chondrocyte proliferation, and regulated bone remodeling through osteocalcin. In particular, further investigations into the cartilage and bone homeostasis of ESWT on medial tibia of subchondral bone in OA knee treatment are necessary.
Acknowledgements
We are grateful to the Reproductive Medicine Laboratory, Genomic and Proteomic Core Laboratory and Stem Cell Research Core Laboratory Facilities, Department of Medical Research, Kaohsiung Chang Gung Memorial Hospital for the supporting of this work. Funds are received support for the research study presented in this article. The funding sources are from Chang Gung Medical Foundation (CMRPG8B1291, 1292, CRRPG8B1293, CMRPG8D1501, 1502 and CLRPG8E0131).
Disclosure of conflict of interest
None.
References
- 1.Weinans H, Siebelt M, Agricola R, Botter SM, Piscaer TM, Waarsing JH. Pathophysiology of peri-articular bone changes in osteoarthritis. Bone. 2012;51:190–196. doi: 10.1016/j.bone.2012.02.002. [DOI] [PubMed] [Google Scholar]
- 2.Goldring SR, Goldring MB. Clinical aspects, pathology and pathophysiology of osteoarthritis. J Musculoskelet Neuronal Interact. 2006;6:376–378. [PubMed] [Google Scholar]
- 3.Johansen PE, Sylvest O. Synovial-fluid changes in “degenerative joint disease”, rheumatoid arthritis and “traumatic arthritis”. Scand J Rheumatol. 1961;7:240–248. doi: 10.3109/rhe1.1961.7.issue-1-4.43. [DOI] [PubMed] [Google Scholar]
- 4.Buckwalter JA, Mankin HJ, Grodzinsky AJ. Articular cartilage and osteoarthritis. Instr Course Lect. 2005;54:465–480. [PubMed] [Google Scholar]
- 5.Li G, Yin J, Gao J, Cheng TS, Pavlos NJ, Zhang C, Zheng MH. Subchondral bone in osteoarthritis: insight into risk factors and microstructural changes. Arthritis Res Ther. 2013;15:223. doi: 10.1186/ar4405. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lane NE, Nevitt MC. Osteoarthritis, bone mass, and fractures: how are they related? Arthritis Rheumatol. 2002;46:1–4. doi: 10.1002/1529-0131(200201)46:1<1::aid-art10068>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 7.Oettmeier R, Abendroth K. Osteoarthritis and bone: osteologic types of osteoarthritis of the hip. Skeletal Radiol. 1989;18:165–174. doi: 10.1007/BF00360962. [DOI] [PubMed] [Google Scholar]
- 8.Ratcliffe A, Seibel MJ. Biochemical markers of osteoarthritis. Curr Opin Rheumatol. 1990;2:770–776. doi: 10.1097/00002281-199002050-00014. [DOI] [PubMed] [Google Scholar]
- 9.Hayami T, Funaki H, Yaoeda K, Mitui K, Yamagiwa H, Tokunaga K, Hatano H, Kondo J, Hiraki Y, Yamamoto T, Duong le T, Endo N. Expression of the cartilage derived anti-angiogenic factor chondromodulin-I decreases in the early stage of experimental osteoarthritis. J Rheumatol. 2003;30:2207–2217. [PubMed] [Google Scholar]
- 10.Funck-Brentano T, Cohen-Solal M. Subchondral bone and osteoarthritis. Curr Opin Rheumatol. 2015;27:420–426. doi: 10.1097/BOR.0000000000000181. [DOI] [PubMed] [Google Scholar]
- 11.Dedrick DK, Goulet R, Huston L, Goldstein SA, Bole GG. Early bone changes in experimental osteoarthritis using microscopic computed tomography. J Rheumatol Suppl. 1991;27:44–45. [PubMed] [Google Scholar]
- 12.Harada S, Rodan GA. Control of osteoblast function and regulation of bone mass. Nature. 2003;423:349–355. doi: 10.1038/nature01660. [DOI] [PubMed] [Google Scholar]
- 13.Karsdal MA, Bay-Jensen AC, Lories RJ, Abramson S, Spector T, Pastoureau P, Christiansen C, Attur M, Henriksen K, Goldring SR, Kraus V. The coupling of bone and cartilage turnover in osteoarthritis: opportunities for bone antiresorptives and anabolics as potential treatments? Ann Rheum Dis. 2014;73:336–348. doi: 10.1136/annrheumdis-2013-204111. [DOI] [PubMed] [Google Scholar]
- 14.Radin EL, Rose RM. Role of subchondral bone in the initiation and progression of cartilage damage. Clin Orthop Relat Res. 1986:34–40. [PubMed] [Google Scholar]
- 15.Hayami T, Pickarski M, Zhuo Y, Wesolowski GA, Rodan GA, Duong le T. Characterization of articular cartilage and subchondral bone changes in the rat anterior cruciate ligament transection and meniscectomized models of osteoarthritis. Bone. 2006;38:234–243. doi: 10.1016/j.bone.2005.08.007. [DOI] [PubMed] [Google Scholar]
- 16.Burr DB. The importance of subchondral bone in osteoarthrosis. Curr Opin Rheumatol. 1998;10:256–262. doi: 10.1097/00002281-199805000-00017. [DOI] [PubMed] [Google Scholar]
- 17.Dieppe P. Subchondral bone should be the main target for the treatment of pain and disease progression in osteoarthritis. Osteoarthritis Cartilage. 1999;7:325–326. doi: 10.1053/joca.1998.0182. [DOI] [PubMed] [Google Scholar]
- 18.Buchbinder R, Green SE, Youd JM, Assendelft WJ, Barnsley L, Smidt N. Shock wave therapy for lateral elbow pain. Cochrane Database Syst Rev. 2005:CD003524. doi: 10.1002/14651858.CD003524.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Frisbie DD, Kawcak CE, McIlwraith CW. Evaluation of the effect of extracorporeal shock wave treatment on experimentally induced osteoarthritis in middle carpal joints of horses. Am J Vet Res. 2009;70:449–454. doi: 10.2460/ajvr.70.4.449. [DOI] [PubMed] [Google Scholar]
- 20.Ochiai N, Ohtori S, Sasho T, Nakagawa K, Takahashi K, Takahashi N, Murata R, Moriya H, Wada Y, Saisu T. Extracorporeal shock wave therapy improves motor dysfunction and pain originating from knee osteoarthritis in rats. Osteoarthritis Cartilage. 2007;15:1093–1096. doi: 10.1016/j.joca.2007.03.011. [DOI] [PubMed] [Google Scholar]
- 21.Mueller M, Bockstahler B, Skalicky M, Mlacnik E, Lorinson D. Effects of radial shockwave therapy on the limb function of dogs with hip osteoarthritis. Vet Rec. 2007;160:762–765. doi: 10.1136/vr.160.22.762. [DOI] [PubMed] [Google Scholar]
- 22.Dahlberg J, Fitch G, Evans RB, McClure SR, Conzemius M. The evaluation of extracorporeal shockwave therapy in naturally occurring osteoarthritis of the stifle joint in dogs. Vet Comp Orthop Traumatol. 2005;18:147–152. [PubMed] [Google Scholar]
- 23.Revenaugh MS. Extracorporeal shock wave therapy for treatment of osteoarthritis in the horse: clinical applications. Vet Clin North Am Equine Pract. 2005;21:609–625. vi. doi: 10.1016/j.cveq.2005.09.001. [DOI] [PubMed] [Google Scholar]
- 24.Zhao Z, Jing R, Shi Z, Zhao B, Ai Q, Xing G. Efficacy of extracorporeal shockwave therapy for knee osteoarthritis: a randomized controlled trial. J Surg Res. 2013;185:661–666. doi: 10.1016/j.jss.2013.07.004. [DOI] [PubMed] [Google Scholar]
- 25.Wang CJ, Weng LH, Ko JY, Sun YC, Yang YJ, Wang FS. Extracorporeal shockwave therapy shows chondroprotective effects in osteoarthritic rat knee. Arch Orthop Trauma Surg. 2011;131:1153–1158. doi: 10.1007/s00402-011-1289-2. [DOI] [PubMed] [Google Scholar]
- 26.Wang CJ, Weng LH, Ko JY, Wang JW, Chen JM, Sun YC, Yang YJ. Extracorporeal shockwave shows regression of osteoarthritis of the knee in rats. J Surg Res. 2011;171:601–608. doi: 10.1016/j.jss.2010.06.042. [DOI] [PubMed] [Google Scholar]
- 27.Wang CJ, Sun YC, Siu KK, Wu CT. Extracorporeal shockwave therapy shows site-specific effects in osteoarthritis of the knee in rats. J Surg Res. 2013;183:612–619. doi: 10.1016/j.jss.2013.02.006. [DOI] [PubMed] [Google Scholar]
- 28.Laverty S, Girard CA, Williams JM, Hunziker EB, Pritzker KP. The OARSI histopathology initiative-recommendations for histological assessments of osteoarthritis in the rabbit. Osteoarthritis Cartilage. 2010;18(Suppl 3):S53–65. doi: 10.1016/j.joca.2010.05.029. [DOI] [PubMed] [Google Scholar]
- 29.Pritzker KP, Gay S, Jimenez SA, Ostergaard K, Pelletier JP, Revell PA, Salter D, van den Berg WB. Osteoarthritis cartilage histopathology: grading and staging. Osteoarthritis Cartilage. 2006;14:13–29. doi: 10.1016/j.joca.2005.07.014. [DOI] [PubMed] [Google Scholar]
- 30.Pastoureau P, Leduc S, Chomel A, De Ceuninck F. Quantitative assessment of articular cartilage and subchondral bone histology in the meniscectomized guinea pig model of osteoarthritis. Osteoarthritis Cartilage. 2003;11:412–423. doi: 10.1016/s1063-4584(03)00050-5. [DOI] [PubMed] [Google Scholar]
- 31.Bellido M, Lugo L, Roman-Blas JA, Castaneda S, Caeiro JR, Dapia S, Calvo E, Largo R, Herrero-Beaumont G. Subchondral bone microstructural damage by increased remodelling aggravates experimental osteoarthritis preceded by osteoporosis. Arthritis Res Ther. 2010;12:R152. doi: 10.1186/ar3103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wang CJ, Huang CY, Hsu SL, Chen JH, Cheng JH. Extracorporeal shockwave therapy in osteoporotic osteoarthritis of the knee in rats: an experiment in animals. Arthritis Res Ther. 2014;16:R139. doi: 10.1186/ar4601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Oxlund H, Andreassen TT. Simvastatin treatment partially prevents ovariectomy-induced bone loss while increasing cortical bone formation. Bone. 2004;34:609–618. doi: 10.1016/j.bone.2003.12.014. [DOI] [PubMed] [Google Scholar]
- 34.Burr DB, Schaffler MB. The involvement of subchondral mineralized tissues in osteoarthrosis: quantitative microscopic evidence. Microsc Res Tech. 1997;37:343–357. doi: 10.1002/(SICI)1097-0029(19970515)37:4<343::AID-JEMT9>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 35.Wang CJ, Hsu SL, Weng LH, Sun YC, Wang FS. Extracorporeal shockwave therapy shows a number of treatment related chondroprotective effect in osteoarthritis of the knee in rats. BMC Musculoskelet Disord. 2013;14:44. doi: 10.1186/1471-2474-14-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Wang CJ, Sun YC, Wu CT, Weng LH, Wang FS. Molecular changes after shockwave therapy in osteoarthritic knee in rats. Shock Waves. 2013;26:45–51. [Google Scholar]
- 37.Wang CJ, Sun YC, Wong T, Hsu SL, Chou WY, Chang HW. Extracorporeal shockwave therapy shows time-dependent chondroprotective effects in osteoarthritis of the knee in rats. J Surg Res. 2012;178:196–205. doi: 10.1016/j.jss.2012.01.010. [DOI] [PubMed] [Google Scholar]
- 38.Burr DB, Gallant MA. Bone remodelling in osteoarthritis. Nature reviews. Rheumatology. 2012;8:665–673. doi: 10.1038/nrrheum.2012.130. [DOI] [PubMed] [Google Scholar]
- 39.Hauschka PV, Mavrakos AE, Iafrati MD, Doleman SE, Klagsbrun M. Growth factors in bone matrix. Isolation of multiple types by affinity chromatography on heparin-Sepharose. J Biol Chem. 1986;261:12665–12674. [PubMed] [Google Scholar]
- 40.Pfeilschifter J, Mundy GR. Modulation of type beta transforming growth factor activity in bone cultures by osteotropic hormones. Proc Natl Acad Sci U S A. 1987;84:2024–2028. doi: 10.1073/pnas.84.7.2024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Rodan GA. Bone homeostasis. Proc Natl Acad Sci U S A. 1998;95:13361–13362. doi: 10.1073/pnas.95.23.13361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Cheng JH, Wang CJ. Biological mechanism of shockwave in bone. Int J Surg. 2015;24:143–146. doi: 10.1016/j.ijsu.2015.06.059. [DOI] [PubMed] [Google Scholar]
- 43.Wang CJ, Wang FS, Yang KD, Weng LH, Hsu CC, Huang CS, Yang LC. Shock wave therapy induces neovascularization at the tendonbone junction. A study in rabbits. J Orthop Res. 2003;21:984–989. doi: 10.1016/S0736-0266(03)00104-9. [DOI] [PubMed] [Google Scholar]