

Abstract
Background:
Brucellosis is a zoonotic pathogen responsible for great economic losses in most sub-Saharan nations. Although Ghana has successfully implemented the “One Health” initiative for the control of some emerging infectious zoonotic diseases with pandemic potential like Avian Influenza, there is very limited data available on brucellosis especially human brucellosis prevalence. He objective of his study is to determine the seroprevalence of human and bovine brucellosis as well as the predisposing factors at the community level in the North Tongu District of Ghana.
Materials and Methods:
Rose Bengal Plate test (RBPT) was used to analyze blood samples from 178 cattle farmers, and 315 cattle. The positive samples were further confirmed with cELISA. Predisposing factors were determined by questionnaires administered to cattle farmers. All sample sites were geo-referenced.
Results:
Human and bovine brucellosis seroprevalence using RBPT were 10.1% and 22.9% respectively. Eighty six percent (62/72) of bovine cases were confirmed with ELISA. Delivery assistants were more likely to be infected (p=0.043) with odds ratio of 2.7. Out of the human cases (18), males constituted 88.9%. Ages 11-20 years recorded 77.7% seropositivity whilst cattle drovers represented 44.5% (8/18) of positives. Significant risk factors in cattle were herd size (p=0.037), history of retained placenta (0.000) and abortion (0.005).
Conclusion:
Bovine and human brucellosis is prevalent in North Tongu district, Ghana. Close contact with parturient cows was a major predisposing factor for human infection. Early referral of positive persons to the Hospital for confirmation and treatment is required to comply with the “One Health” initiative on brucellosis and other zoonoses.
Keywords: Brucellosis, cattle, handlers, Tongu, Volta, Ghana
Introduction
It is estimated that about 61% of the known 1,415 human pathogens are zoonotic, Taylor et al; (2001), which calls for a close collaboration between human and animal health. The concept of ‘One Medicine,’ which is often defined as the science of all human and animal health issues or diseases has been a global issue for several decades, yet its uptake is still generally low especially in developing countries where it could have made the most impact, Schelling et al., (2003).
In Africa, brucellosis remains a largely neglected disease with little attention to its control and prevention (Ibironke et al., 2008). Apart from South Africa, vaccination is rarely conducted and if done, it has been on ad hoc basis rather than a co-ordinated National Program (McDermont and Arimi, 2002). Despite the presumptively high prevalence of brucellosis in all major livestock production systems in sub-Saharan Africa, its presence often remains unrecognized due to lack of reliable data. The risk of disease transmission to human population is generally determined by the presence of brucellosis in livestock and professional engagements at the level of animal raising, especially relating to sanitary conditions at the working place, food production, and hygiene. The risk factors for brucellosis have been investigated in detail in different countries (Gotuzzo et al., 1987, Al-Shamahy et al., 2000, Bikas et al., 2003), but due to differences in cultural and farming practices in various areas, more research is required to improve our understanding.
The economic implications of brucellosis in cattle can be huge, affecting mainly breeding animals with associated losses due to abortion, stillbirths, unexpected deaths and reduced milk production. In humans on the other hand, the interference in reproduction or infertility created is far beyond any economic losses because it can hardly be measured in medical care (Nicoletti, 1982).
Human brucellosis has been poorly studied in Africa. Seroprevalence of 3.8% has been reported in nomadic pastoralists from Chad (Schelling et al., 2003). Occupational contacts, like butchers, slaughterhouse workers, milkers, and cow attendants were found to have an infection rate of 1% in a study in eastern Sudan (El-Ansary et al., 2001). Similarly, slaughterhouse workers in Djibouti were found to have a higher positive rate of 6.5% (Chantal et al., 1996) while high-risk groups from Eritrea had a seroprevalence between 3.0% and 7.1% (Omer et al., 2000) and 5.2% in eastern Nigeria (Baba et al., 2001). However, hospital based studies among febrile patients in a large hospital in Kampala, Uganda, yielded as high as 13.3% (Mutanda, 1998).
In 2004, out of the 44 African countries listed on the International Organization of Epizootics (OIE) website, 36 reported occurrence of brucellosis including Ghana. Only two studies have been published on the subject in Ghana, precisely in Akwapim South in 1992 and 2000 which did not report on prevalence of human brucellosis (Turkson, 1992; Kubuafor et al.., 2000). From 2006 to 2008, less than 1 % of the cattle population in Ghana was vaccinated with Brucella abortus RB51 vaccine. The low coverage of vaccination can obviously not protect cattle against brucellosis (Roth et al., 2003). In the North Tongu District, although there is no published study on the seroprevalence of bovine and human brucellosis, the proximity at which cattle and farmers live with their animals due to fear of cattle rustling, the common practice of herding of cattle by children (cowboys) and the consumption of fresh unpasteurized milk by farmers and their families makes it very logical to assume that the prevalence will be quite high. This study was therefore conducted to determine the prevalence of bovine and human brucellosis and the predisposing factors that influence this infection in the North Tongu district to provide the compelling evidence that can be used to generate the required intelligence to inform management decisions and guide policy.
Materials and methods
Study Design
A cross-sectional study was carried out from February to June 2011 to determine the sero-prevalence of human and bovine brucellosis in North Tongu District. Two separate surveys were done using set questionnaires on human exposure and another on cattle. There was a laboratory investigation involving 178 humans and 315 cattle.
Study Site
The North Tongu District which is the study site was initially called Adidome District and is one of the 18 administrative districts in the Volta Region of Ghana. It lies within latitude 5047 North to 60 North and longitude 005 East. The total area of the district is 1460 km square, which is about 7.1% of the Volta Region. It is divided into two unequal parts by the Volta River, stretching from the lower Volta gorge near Akosombo in the north to Awadiwe Island located north of the lower Volta Bridge at Sogakope. Geographically, it shares borders with South Tongu to the south-east, Dangbe East and West Districts to the south-west and with Asuogyaman District to the west. To the north and east, the district is bordered by Ho Municipality and by Akatsi District respectively (Figure 1).
Figure 1.
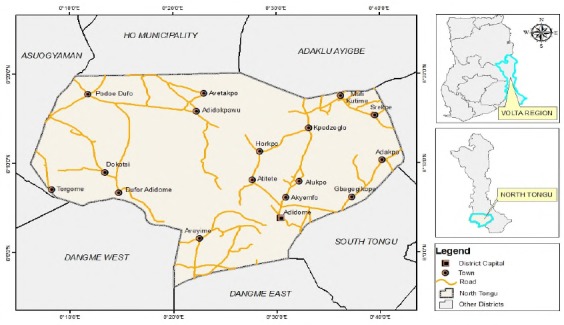
Map showing North Tongu District and its neighboring Districts
The district lies within the tropical savanna grassland zone. It has shrubs and grassland suitable for cattle grazing which makes the district one of the largest cattle producing areas in the country. About 69% of the active population is engaged in agriculture of which over 80% rear livestock alongside crop farming (North Tongu District Profile). Cattle production is mainly done on the extensive system where animals are herded by local cattle boys or Fulani for grazing and watering in the morning and returned at late afternoon. There are communal grazing fields and dams where cattle from or herds from several kraals converge.
Variables
Dependent Variables
Seropositivity in Humans
Seropositivity in Cattle
Independent Variables
The independent variables were expressed in four parameters, three for humans and one for cattle. In humans, we had socio-demographics which included age groups, educational level and occupation. The other two were knowledge of farmers on the disease in both animals and humans and the risk factors that contribute to infection. Individual cattle data was also collected in the form of demographics and risk factors which might determine any relationship with outcome or seropositivity.
Sampling
Study Population
This comprises all persons and all cattle in the North Tongu district. Human population is 130,388 (Statistical Service, 2010) and a cattle population of 34,564 (Veterinary Statistics, VSD 2005).
Inclusion Criteria
Persons aged 1 year and above who consented to the study or persons ascended to the study by parents or guardians were our human study population while cattle aged 6 months and above were included in our study population.
Exclusion Criteria
Pregnant women, breastfeeding mothers and people with physical and mental challenges that are unable to give consent were excluded from the study. Calves less than 6 months of age were also excluded from the study because they are not weaned and are not served.
Sampling Procedure
Cattle and Humans
Random sampling was used to select the kraals as well as the cattle. A population size was obtained from the cumulative number of cattle in each kraal. The random number table was then used to select the sample size of 250 cattle from the kraals. The selected random numbers, each of which was not to be greater than the sampling frame, were then used to select the kraals to which they belonged. The cattle in a selected kraal were counted serially and the one that corresponded to the selected random number was picked for the study. All persons living in households with the selected kraals who fall within the inclusion criteria and consented or ascended for were sampled until we got the total number assigned for the study.
Sample Collection
Blood Sample
For the identification of the animals, owners’ experience using descriptive names for cattle was adopted this appears to be reliable since they depict the colour, size and other identifying feature. Blood was collected from the jugular vein and radial vein of cattle (5ml) and human (3ml) respectively after the area was disinfected with 70% alcohol. The blood samples were centrifuged at 2500 rpm for 10 min, after which they were transferred into eppendorf vials to be kept at -20°C until analysis.
Laboratory Method
The laboratory diagnosis was performed using Rose Bengal Plate Test (RBPT) and Competitive Enzyme-linked Immuno-Sorbent Assay (cELISA). The RBPT is a rapid slide agglutination procedure used for the direct detection of Brucella antibodies in both human and animal sera. All cattle sera positive to RBPT (n = 72) were subjected to c-ELISA as a confirmatory test to eliminate any positive reaction due to vaccination or cross reaction. (OIE 2012)
Data Analysis
Data was entered and cleaned in Epidata. For socio-demographic categorical data (e.g sex), summary tables of counts and percentages were presented using Pearson’s chi square tests or Fisher’s exact tests (where cells/counts were small). For socio-demographic continuous data (e.g age), summary tables of means, standard deviations were presented. Pearson’s chi square test and Fisher’s exact test were used to establish associations between demographic data and dependent variables. Tabulations of frequencies and graphical presentations were done using Statistical Package for Social Sciences (SPSS) Version 17.0. All statistical tests were conducted as two-tailed and declared significant for p-value < 0.05.
Ethical Considerations
The study protocol was reviewed and approved by the ethical review board of the Ghana Health Service and the Veterinary Services Directorate of the Ministry of Food and Agriculture, Ghana. This protocol was followed and permission sought from the District Health Management Team (DHMT) and the District Assembly. Permission was granted by traditional rulers and the community members for interaction with community members. Verbal and written consent was duly sought from the study participants and there was the opportunity to opt in or out of the study at any given time. All human samples collected had assigned numbers and not names of study participants to ensure confidentiality. Data was stored in computer with password and used only by authorized persons.
Results
Bovine brucellosis seroprevalence with the use of RBPT (72/315) for North Tongu District was 22.9%. Meanwhile, human brucellosis with the use of RBPT (18/175) was 10.1%. All positive bovine sera were tested in cELISA kit for the confirmation recording 86.1% (62/72). About 89% (16/18) of the positive human participants were males. Age groups most affected were 11-15 and 16-20 with 44.4% and 33.3% respectively. Out of 28 kraals sampled, 19 had at least one positive case with a herd prevalence of 67.9%. The c ELISA test confirmed 14 out of the 19 kraals that tested positive using RBPT. Within herd prevalence ranged as high as 80 to 100% in two kraals whereas five kraals recorded 30-50% and the rest fell below 30%.
Table 1 indicates increased seroprevalence in the cattle grouped in various kraals. Cattle grouped from 1-100 had 20.3% and this increased slightly in kraals with 201-300 cattle (21.9%). The figure was more than double (50%) in 301-400 animals in kraals and the second highest seroprevalence was in kraals above 400 cattle (29.5%). A larger herd size was a risk factor to seropositivity in this study. This association was statistically significant with p-value =0.037.
Table 1.
Influence of herd size on the seroprevalence of brucellosis in North Tongu district of Volta Region, Ghana.
| Herd size | Result | Total sample | S prevalence | P- value | |
|---|---|---|---|---|---|
| Positive | Negative | ||||
| 1- 100 | 26 | 102 | 128 | 20.3 | |
| 101-200 | 13 | 65 | 78 | 16.7 | 0.037 |
| 201 -300 | 7 | 25 | 32 | 21.9 | |
| 301 -400 | 8 | 8 | 16 | 50.0 | |
| 401- 500 | 18 | 43 | 61 | 29.5 | |
| Total | 72 | 243 | 315 | ||
Table 2 shows the association between seroprevalence and important risk factors in this study. Out of 73 cattle with history of abortion, 29 (39.7%) were found to be positive of the disease showing that cattle with history of abortion are almost 3 times more likely to be positive of bovine brucellosis (OR=2.9). This association was statistically significant with p-value<0.005. Twenty-nine cattle were known to have had retained placenta out of which 68.9% (20/29) were positive cases. Cows that had ever retained placenta were about 4 times more likely to have B. abortus (OR=3.9). According to Fisher’s Exact Test this was statistically significant with p-value=0.005 as shown in Table 2.
Table 2.
Seroprevalence in cattle with history of abortion and retained placenta
| Variable | Response | Results | Total Respondent | Prevalence | P-value | |
|---|---|---|---|---|---|---|
| Abortion | Positive | Negative | 0.00 | |||
| Yes | 29 | 44 | 73 | 39.7 | ||
| No | 43 | 244 | 217 | 19.8 | ||
| Total | 72 | 188 | 290 | |||
| Retained placenta | Yes | 20 | 9 | 29 | 68.9 | 0.005 |
| No | 52 | 209 | 261 | 19.9 | ||
| Total | 72 | 218 | 290 | |||
Table 3 shows 16.4% of participants who assisted cows during deliveries were affected with the disease. Persons who assist cows during deliveries where the bacteria is often shed are about 3 times more likely to be infected (OR=2.7). Furthermore, this association was statistically significant with Fisher’s Exact Test (p=0.043).
Table 3.
Seroprevalence in participants who attended to cows during deliveries
| Delivery Attendants | Results | Total Respondents | Prevalence | P- Value | |
|---|---|---|---|---|---|
| Positive | Negative | 0.043 | |||
| Yes | 10 | 51 | 61 | 16.4 | |
| No | 8 | 109 | 117 | 6.8 | |
| Total | 18 | 160 | 178 | ||
Note: 88.9% of the affected are males
Discussion
This study described the prevalence of brucellosis in cattle and their handlers in North Tongu District. All sera samples examined in this study were subjected to the RBPT as screening and the cELISA as confirmatory test, as recommended by OIE (2001). A high degree of agreement between both tests is normally expected, Hadad and Jamalludeen (1992). In our study, however, 86.2% of the positive samples in RBPT were confirmed in cELISA test which has higher sensitivity and specificity as recommended by OIE (2001). The cELISA is considered suitable for eliminating most serological reactions of vaccinated animals (OIE 2001). The experience of individual investigator could be considered in the estimation of the agglutination reaction; hence there could be an overestimation during the test. On the other hand, cross-reactions with other bacteria could have led to false positive reactions (Oloffs et al, 1998). According to OIE (2012), the RBPT provides more likely false positive results than to miss brucellosis, hence the need for confirmatory test cELISA, which was carried out and this led to a reduction in the number of positive samples (OIE 2012). The overall seroprevalence of bovine brucellosis in this study with RBPT and cELISA was 22.9% and 19.7% respectively. This reflects either past or present exposure to Brucella organisms, because vaccination against brucellosis has not been practiced in North Tongu District in the past 10 years. These figures fall within what was reported by McDermott and Arimi (2002) that bovine brucellosis in the sub-Saharan Africa ranged from as low as 3.3% in the Central African Republic to as high as 40.1% in neighboring Togo. However, these figures are quite higher than the 9.3% and 6.6% reported by Turkson et al (1992) and Kubuafor et al (2000) in Ghana. Considering that these studies (Turkson et al 1992, Kubuafor et al 2000) took place in the Eastern Region where the cattle population was not as large as that of the Volta Region and at a time when fewer people were involved in buying and selling of cattle for breeding in the southern sector compared to today. It is also possible that current figures may be equally high all over in the southern sector.
In this study, most of the herds (67.9%) were found to have at least one seropositive case which suggests that without any control measures in place to curb the spread of infection, the intra herd rate of infections is more likely to increase with time, either with an exponential epizootic shape or with slow enzootic shape depending on the prevailing epidemiological situations (Nicolleti, 1980). The association of infection rate in this study with the cattle grouped from 1-100 up to 500 heads has statistical support (P <0.037). In general, it appears that the herd level infection rate rises in parallel with the increment in farm size. Asfaw et al. (1998) reported infection rates of 17.6%, 100% and 100% for small, medium and large farms, respectively in Ethiopia. This relationship is rationalized by the intense animal contact within the herd and especially following abortion episodes (Nicoletti, 1980; Walker, 1999). Despite the wide variability in what constitutes a large herd, it is generally accepted that an increase in herd size is usually accompanied by increase in stoking size Omer et al., (2000). Hellman et al. (1984), equally agree that a higher level of infection rate of bovine brucellosis is usually found in large herds compared to small herds. Cattle rearing in North Tongu District are noted to mainly rely on communal grazing fields and community watering points which is likely to increase contacts thereby a potential for spread of bovine brucellosis.
Human brucellosis seroprevalence of 10.1% reported in our study is higher than the reported figures of 1% from Sudan (El-Ansary et al., 2001) and 3.8% from Chad (Schelling et al., 2003). Since previous studies on this subject in Ghana did not report on human brucellosis prevalence, there is no baseline data to establish any form of local comparison. Although the 13.3% reported among febrile patients in a hospital in Kampala (Mutanda, 1998) appears to be high, there is no corresponding hospital based data locally in Ghana for further analysis. This poor state of data on brucellosis even within the human health set up could be explained by the poor knowledge and diagnostic capacity worsened by the possibility of clinical misdiagnoses with other more common several febrile illnesses. In order to maximize the concept of One Health initiative, veterinary health service and human health service providers will need to collaborate more in the field of research, diagnostic acumen and containment measures (Folitse et al., 2014)
On the predisposing factors, this study has shown that the infection rate is higher among mature animals as 4-6 years and over 6 years age groups recorded 37.5% and 52.8% respectively. Although, this coincides with results from other workers (Weidmann, 1991, Walker, 1999) who reported brucellosis as a tropical livestock disease of the sexually mature animals, with the predilection site being the reproductive tract, especially the gravid uterus. Such views have been shared by Ahmed and Munir, (1995) who further reported that the antibody titer against Br. abortus appears to be associated with age, since low values have been reported more in young stock than in the adults.
Unlike in cattle, humans between the ages of 11-20 years were most affected and more specifically those between 11-15 years. The generally poor understanding and assessment of risk among such very young children could predispose them to high risk behavior or practices. Children of such age should be at school by all accepted standards and therefore it comes as no surprise to find differing reports from Al-Nassir (2011) where persons in their third to fifth decades of life were most commonly affected. However, it should be noted that cattle herding in North Tongu District and for that matter Ghana is mainly carried out by children of schooling age who are believed to listen to advice rather than the older ones and this may have accounted for this finding (Tasiame Personal communication). Furthermore, these children are known to engage in in milking, consumption of unpasteurized milk even directly from the teats of cows and assist during deliveries. The sex most affected in humans was males (88.9%) although this could be related to the general male dominance in most of the cattle handling ventures and most of the high risk contacts. This as well conforms to worldwide human brucellosis pattern where males are commonly affected than females with a ratio of 5:2-3 in endemic areas (Al-Nassir, 2011).
In cattle, however, this study shows a higher prevalence in females than males which could probably be due to the relatively smaller number of male cattle (25) sampled compared to females (290). This may also be due to the predilection sites of Brucella spp which are mainly the uterus, placenta, udder and associated lymph nodes even though males can also be affected
The study indicated that persons directly involved in the day to day activities of cattle rearing had high prevalence rates. Cattle herdsmen recorded 44.4% (8/18) of all affected persons and students who also assist their parents in caring for the cattle also recorded 33.3% (6/18). Milking of cows played a major role whereby 72.2% (13/18) of affected persons were engaged in this activity. Similarly, these persons did not practise hand washing before and after milking the cows representing 83.3% (15/18). About 94% of infected persons consumed milk yet only 27.8% boiled the milk before drinking. In many countries it has been observed that there is a very close positive correlation between incidence of brucellosis in animals and incidence of the disease in humans (Bikas et al, 2003). Furthermore, studies of risk factors have concluded that several behavioural items like dairy products consumption, milking and animal delivery practices play a very important role in the spread of the disease (Refai, 2002).
It was found out that 55.6% of human cases assisted cows during deliveries which are one of the areas where the bacteria are mostly excreted into the environment. Kozukeev, (2003) also indicated cases of human brucellosis occurred in persons who owned cattle and assisted during deliveries and who consumed unprocessed dairy products. He also found that knowledge of the mode of brucellosis transmission appeared to be protective against disease transmission. In our study, knowledge of community members about the disease was very poor (Kozukeev, 2003).
Out of 18 cases of persons positive for brucellosis by RBPT, the clinical manifestation in 12 individuals complained of intermittent fever, chills and joint pains. This is in agreement with Agasthya et al, (2007) in a study of risk factor groups of brucellosis where some of the positive cases showed same signs. Megersa et al, (2011) also asserted to the fact that such cases are mostly considered as febrile diseases and treated empirically.
In our study, retained placenta and abortion history were statistically significant with seropositivity with P values of 0.005 and 0.000 respectively. These findings conform to other studies by Tesfaye et al, (2011) and Matope et al, (2010).
Conclusions
This is the first serological evidence of human brucellosis in North Tongu district, Ghana. Age, sex and closeness with parturient cows were identified as predisposing factor for human infection at the community level. History of abortion, retained placenta and herd size were significant risk factors of bovine brucellosis whilst assisting cows during deliveries was the main risk factor for human brucellosis which were all statistically significant. Positive cattle correlated with infected persons in the same households confirming the fact that animals are the main reservoirs of the disease. Community knowledge about risk factors of the disease in cattle and humans was very poor.
Recommendations
A coordinated eradication program based on the principles of One Health should be instituted by government. We also recommend a joint sensitization from physicians and veterinarians about the disease especially in risk prone areas. Routine or regular requests for laboratory diagnosis as is being done for other endemic disease like typhoid fever and malaria should be undertaken to enhance proper diagnosis. There is the need for further studies of the disease especially in human populations since this is the first research reporting human brucellosis in Ghana.
Acknowledgement
The author is grateful to the Accra Veterinary Laboratory and its staff for assistance in the analysis of samples and to Field Epidemiology and Laboratory Training Program, School of Public health, Legon for direction.
References
- 1.Agasthya A.S, Isloor S, Prabhudas K. Brucellosis in high risk group individuals. Med Microbiol. 2007;25:28–31. doi: 10.4103/0255-0857.31058. [DOI] [PubMed] [Google Scholar]
- 2.Al-Nassir Brucellosis. 2011 Accessed on http://emedicine.medscape.com/article/213430-overview#00199. 25/07/2011 .
- 3.Al-Shamahy H.A, Whitty C.J, Wright S.G. Risk factors for human brucellosis in Yemen: a case control study. Epidemiol Infect. 2000;125:309–13. doi: 10.1017/s0950268899004458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Asfaw Y, Molla B, Zessin H.K, Tegene A. The Epidemiology of bovine brucellosis in intra and periurban dairy production systems in and around Addis Ababa. Bull. Anim. Health Prod. Afr. 1998;46:217–224. [Google Scholar]
- 5.Baba M.M, Sarkindared S.E, Brisibe F. Serological evidence of brucellosis among predisposed patients with pyrexia of unknown origin in the North Eastern Nigeria. Cent Eur J Public Health. 2001;9(3):158–61. [PubMed] [Google Scholar]
- 6.Bikas C, Jelastopulu E, Leotsinidis M, Kondakis S. Epidemiology of human brucellosis in a rural area of North-Western Peloponnese in Greece. Eur J Epidemiol. 2003;18:267–274. doi: 10.1023/A:1023368420840. doi:10.1023/A:1023368420840. [DOI] [PubMed] [Google Scholar]
- 7.Chantal J, Bessiere M.H, Le Guenno B, Magnaval J.F, Dorchies P. Serologic screening of certain zoonoses in the abattoir personnel in Djibouti. Bull. Soc. Pathol. Exot. 1996;89:353–357. [PubMed] [Google Scholar]
- 8.El-Ansary E.H, Mohammed B.A, Hamad A.R, Karom A.G. Brucellosis amonganimals and human contacts in eastern Sudan. Saudi Med. J. 2001;22:577–579. [PubMed] [Google Scholar]
- 9.Folitse R.D, Opoku-Agyemang T, Emikpe BO, Eyarefe O.D, Atawalna J. One Health Delivery of Veterinary Education: The case of Kwame Nkrumah University of Science and Technology School of Veterinary Medicine. African Journal of Medicine and Medical sciences. 2014;43(Suppl) [PubMed] [Google Scholar]
- 10.Gotuzzo E, Seas C, Guerra J.G, Carrillo C, Bocanegra T.S, Calvo A, Castaneda O, Alarcon G.S. Brucellar arthritis: a study of 39 Peruvian families. Ann. Rheum Dis. 1987;46:506–9. doi: 10.1136/ard.46.7.506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hadad J. J, Jamalludeen N. M. A. Brucella strains isolated from cattle inNinevah province, Iraq. Iraqi Journal of Veterinary Sciences. 1992;5(2):165–170. [Google Scholar]
- 12.Hellman E, Staak C, Bauman M. Bovine brucellosis among two different cattle populations in Baher el ghazal province of Southern Sudan. Trop. Med Parasitol. 1984;35:123–126. [PubMed] [Google Scholar]
- 13.Ibironke M, McCrindle M, Fasina O, Godfroid J. Evaluation of problems and possible solutions linked to the surveillance and control of bovine brucellosis in sub-Saharan Africa, with special emphasis on Nigeria. Inferm Infecc Microbiol Clin. 2008;8:19–24. [PubMed] [Google Scholar]
- 14.Kozukeev B, Ajeilat S, Maes E, Favorov M. Risk Factors for Brucellosis - Leylek and Kadamjay Districts, Batken Oblast, Kyrgyzstan, January—November 2003. 2003 [PubMed] [Google Scholar]
- 15.Kubuafor D.K, Awumbila B, Akanmori B.D. Seroprevalence of brucellosis in cattle and humans in the Akwapim-South district of Ghana: public health implications. Acta Trop. 2000;76:45–48. doi: 10.1016/s0001-706x(00)00088-7. [DOI] [PubMed] [Google Scholar]
- 16.Matope G, Bhebhe G, Muma J, Lund A, Skjerve E. Herd-level factors for Brucella seropositivity in cattle reared in smallholder dairy farms of Zimbabwe. 2010 doi: 10.1016/j.prevetmed.2010.01.003. Accessed at http://lib.bioinfo.pl/pmid:2011687025/07/2011 . [DOI] [PubMed]
- 17.McDermott J.J, Arimi S.M. Brucellosis in sub-Saharan Africa: epidemiology, control and impact. Vet. Microbiol. 2002;90:111–134. doi: 10.1016/s0378-1135(02)00249-3. [DOI] [PubMed] [Google Scholar]
- 18.Megersa B, Biffa D, Niguse F, Rufael T, Asmare K, Skjerve E. Cattle brucellosis in traditional livestock husbandry practice in Southern and Eastern Ethiopia, and its zoonotic implication. 2011 doi: 10.1186/1751-0147-53-24. Accessed at http://lib.bioinfo.pl/pmid:21473760 on 25/07/2011 . [DOI] [PMC free article] [PubMed]
- 19.Mutanda L.N. Selected laboratory tests in febrile patients in Kampala, Uganda. East Afr. Med. J. 1998;75:68–72. [PubMed] [Google Scholar]
- 20.Nicoletti P. The epidemiology of bovine brucellosis. In: Brandly C. A, Corneleius G.A, editors. Advance in Vet. Sci. Comparative Med. New York: Academic Press Inc; 1980. 1980. pp. 68–69. [PubMed] [Google Scholar]
- 21.Nicoletti P. Diagnosis and vaccination for the control of brucellosis in the Near East. FAO Animal Production and Heath Paper. No. 83, Rome, Italy. 1982 [Google Scholar]
- 22.O.I.E. World Organisation for Animal Health. 2001 [Google Scholar]
- 23.OIE Terrestrial Manual. Bovine brucellosis, chapter 2.4.3. 2012 [Google Scholar]
- 24.Oloffs A, Baumann M.P.O, Afema J, Nakavuma J. Experiences with a strategy to investigate bovine brucellosis in a rural area in Southwest Uganda. Revue delevage Med.vet. Pays trop. 1998;51(2):101–105. [Google Scholar]
- 25.Omer M.K, Assefaw T, Skjerve E, Holstd G, Woldehiwot Z. Risk factor for Brucella species. Infection in dairy cattle farms in Asmara, state of Eritrea. Preventive Vet. Med. 2000;46:257–265. doi: 10.1016/s0167-5877(00)00152-5. [DOI] [PubMed] [Google Scholar]
- 26.Refai M. Incidence and control of brucellosis in the Near East region. Vet Microbiol. 2002;90:81–110. doi: 10.1016/s0378-1135(02)00248-1. doi:10.1016/S0378-1135(02)00248-1. [DOI] [PubMed] [Google Scholar]
- 27.Roth F, Zinsstag J, Orkhon D, Chimed-Ochir G, Hutton G, Cosivi O, Carrin G, Otte J. Human health benefits from livestock vaccination for brucellosis: case study. 2003 [PMC free article] [PubMed] [Google Scholar]
- 28.Schelling E, Diguimbaye C, Daoud S, Nicolet J, Boerlin M, Tanner P, Zinsstag J. Brucellosis and Q-fever seroprevalences of nomadic pastoralists and their livestock in Chad. 2003 doi: 10.1016/j.prevetmed.2003.08.004. Accessed at http://www.ncbi.nlm.nih.gov/pubmed/14623412 on 28/07/2011 . Statistical Service, 2010. [DOI] [PubMed]
- 29.Taylor L.H, Latham S.M, Woolhouse M.E.J Risk factors for human disease emergence. Philosophical Transactions of the Royal Society of London Series B- Biological Sciences. 2001;356:983–989. doi: 10.1098/rstb.2001.0888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Tesfaye G, Tsegaye W, Chanie M, Abinet F. Seroprevalence and associated risk factors of bovine brucellosis in Addis Ababa dairy farms. 2011 doi: 10.1007/s11250-011-9798-0. Accessed at http://lib.bioinfo.pl/pmid:21331496 on 25/07/2011 . [DOI] [PubMed]
- 31.Turkson P.K. Epidemiology of bovine brucellosis in the coastal savanna zone of Ghana. 1992 doi: 10.1016/0001-706x(92)90005-i. doi:10.1016/0001-706X(92)90005-I. [DOI] [PubMed] [Google Scholar]
- 32.Veterinary Statistics, Veterinary Service Department. 2005 [Google Scholar]
- 33.Walker R.L. Brucella. In: Dwight C.H, Chunge Z.Y, editors. Vet. Microbiol. Massachusetts, Black Wells Sci. 1999. pp. 196–203. [Google Scholar]
- 34.Weidmann H. Survey of means now available for combating brucellosis in cattle production in the tropics. Animal research and Development. 1991;33:100–111. Tuebingen Inst. Sci. Coop. [Google Scholar]