

Abstract
A 69-year-old woman was admitted to hospital, complaining of fatigue and dry cough. Her renal function deteriorated rapidly, and the laboratory findings showed elevated myeloperoxidase-specific anti-neutrophil cytoplasmic antibody (ANCA). Renal biopsy examination revealed crescentic glomerulonephritis (pauci-immune type), and linear opacities and a honeycomb appearance in both lower lobes was evident on the chest computed tomography scan. The patient was diagnosed as having ANCA-associated glomerulonephritis complicated with mild interstitial pneumonia (IP). Treatment with methylprednisolone pulse therapy improved both her renal function and IP, but her lung lesions worsened during the course of tapering the prednisolone doses. After careful observation, her IP improved gradually without specific treatment. Worsening or improvement of her lung lesions was accompanied by changes in the serological markers of IP, namely, surfactant protein-A, surfactant protein-D, and KL-6. We found that monitoring these markers was helpful in diagnosing and managing IP in our patient with ANCA-associated vasculitis.
Keywords: Anti-neutrophil cytoplasmic antibody, Interstitial pneumonia, Surfactant protein-A, Surfactant protein-D, KL-6
Introduction
Myeloperoxidase (MPO)-specific anti-neutrophil cytoplasmic antibody (ANCA)-associated glomerulonephritis is a rapidly progressive and often irreversible disease of unknown etiology. Vasculitis plays a major role in the pathogenesis of the disease, and the lungs are another target organ in MPO–ANCA-associated vasculitis [1]. Recent studies have revealed that serum levels of surfactant protein-A (SP-A), surfactant protein-D (SP-D) and KL-6 reflect the disease activity of interstitial pneumonia (IP) [2–4]. However, there are few reports on the monitoring of these markers in patients with ANCA-associated vasculitis. Here we report a 69-year-old woman with ANCA-associated glomerulonephritis complicated with IP, whose clinical course was monitored with serum SP-A, SP-D and KL-6.
Case report
A 69-year-old woman was referred to hospital for evaluation of renal dysfunction in November 200X. Her chief complaints were fatigue and dry cough. The woman had a history of hypertension, which had been treated for 13 years. She had no history of renal dysfunction or urinalysis abnormality. She developed dry cough and wheezing 2 months before referral, and her family doctor diagnosed her as having bronchial asthma. She was shown to have hematuria, proteinuria and renal insufficiency with a serum creatinine level of 1.9 mg/dL (168 μmol/L) for the first time in October 200X, and her renal function deteriorated rapidly. Ultimately she was referred to the hospital and was admitted in December 200X. The physical examination on admission showed an elderly women who had a height of 148 cm, weight of 50 kg, blood pressure of 152/70 mmHg and a regular pulse at 78/min. No lymphadenopathy was apparent. Further physical examinations revealed mild conjunctival pallor, fine crackles at both lower lungs, and ecchymosis at her right pedal. Laboratory tests revealed leukocytosis (white cell count 11,570/μL) and normochromic normocytic anemia (hemoglobin 8.0 g/dL). An elevated erythrocyte sedimentation rate (102 mm/h), and elevated level of C-reactive protein (CRP 6.3 mg/dL) were observed. Renal dysfunction was noted, with a blood urea nitrogen level of 60 mg/dL, and serum creatinine level of 3.5 mg/dL (309 μmol/L), and urinalysis revealed proteinuria (1.8 g/day) and microscopic hematuria. Her estimated glomerular filtration rate was 10.8 mL/min/1.73 m2. MPO–ANCA concentration was found to be elevated to 56 EU. Anti-glomerular basement membrane antibody and proteinase-3-specific ANCA were not detected. Arterial blood gas analysis on admission was normal, with a pH value of 7.38, partial pressure of O2 in the blood (PaO2) of 87.7 torr and PaCO2 of 37.1 torr in room air.
The chest radiograph showed reticular opacities in both lower lung fields. Linear opacities and a honeycomb appearance was apparent in both lower lobes on the chest computed tomography (CT) scan (Fig. 1). Light microscopic examination of 12 glomeruli of the kidney biopsy specimen revealed 11 glomeruli with crescent formation and one glomerulus with hyalinosis (Fig. 2). Moderate interstitial lymphocyte infiltration was seen, and no staining for immunoglobulin or complement was observed. The patient was diagnosed as having ANCA-associated glomerulonephritis (pauci-immune type) complicated with mild IP.
Fig. 1.

Chest computed tomography revealing linear opacities and honeycomb appearance in the both lower lobes
Fig. 2.
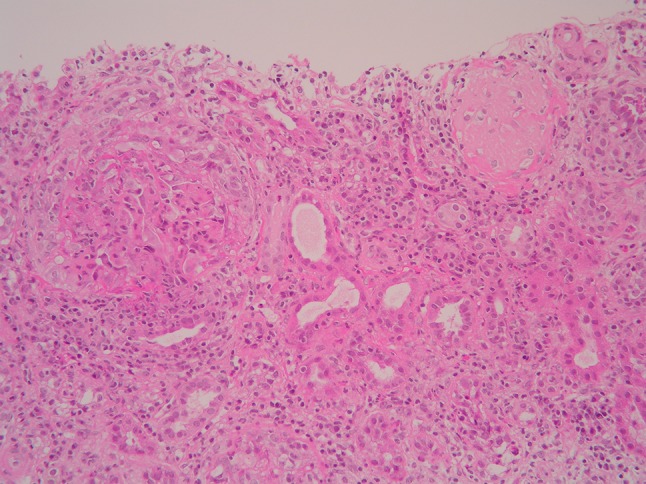
Light micrograph of a kidney biopsy specimen. Crescent formation and hyalinosis in the glomeruli are present (hematoxylin and eosin staining; ×200)
To improve her renal function, the patient was initally treated with methylprednisolone pulse therapy, which was followed by oral prednisolone after renal biopsy. The clinical course of the patient is shown in Fig. 3. The serum creatinine level rose to a peak of 4.2 mg/dL (371 μmol/L) before eventually beginning to decline. Her MPO–ANCA titer was found to have decreased to within the normal range after two course of methylprednisolone pulse therapy. Her renal function improved incompletely, with a serum creatinine level of 2.0 mg/dL (177 μmol/L). However, she began to experience low-grade fever and mild dyspnea when her prednisolone doses were tapered to 25 mg/day. On physical examination, the fine crackles at both lower lungs were increased. Arterial blood gas analysis showed hypoxemia (pH 7.39, PaO2 67.6 torr, PaCO2 34.6 torr in room air), and her serum concentration of CRP was elevated to 4.7 mg/dL. However, her renal function remained stable, and her serum MPO–ANCA concentration was below the detection limit. The chest CT revealed ground-glass opacities in both lungs, suggesting the deterioration of IP (Fig. 4a). Gallium-67 scintigraphy results were positive for both her lungs, a finding which was not observed just after her admission. The serum levels of SP-A, SP-D and KL-6 were 161 ng/mL, 139 ng/mL and 1,490 IU/mL, respectively, which was a marked increase compared to the levels on admission (102 ng/mL, 27 ng/mL and 408 IU/mL, respectively). The sputum culture test did not indicate bacterial infection. Bronchoalveolar lavage (BAL) examination showed a total cell count of 2.8 × 104/mL, of which 48 % were histiocytes, 44 % were lymphocytes (CD4/CD8 ratio 0.88), 6 % were neutrophils and 2 % were eosinophils. There was no evidence of Pneumocystis spp. or hemosiderin-laden macrophages on her BAL examination. The patient was observed carefully without additional immunosuppressive therapy because the clinical course was not so fulminant and she had already treated with prednisolone. Her symptoms improved gradually. The levels of SP-A, SP-D and KL-6 decreased in parallel with improvements in her symptom and lung lesions. At this time her prednisolone doses were tapered very carefully. Her IP and renal function remained stable, and she was discharged on hospital day 146 (Fig. 4b).
Fig. 3.

Clinical course of the patient. mPSL Methyl-prednisolone, PSL prednisolone, SP-A surfactant protein-A, SP-D surfactant protein-D, Cre serum creatinine concentration, MPO–ANCA myeloperoxidase-specific anti-neutrophil cytoplasmic antibody, CT computed tomography
Fig. 4.

a Chest CT scan revealing ground-glass opacities in the both lungs, suggesting the deterioration of interstitial pneumonia. b Chest CT scan showing improvement of her interstitial pneumonia
Discussion
Antineutrophil cytoplasmic antibody-associated glomerulonephritis is a form of rapidly progressive glomerulonephritis (RPGN) that has an extremely high mortality rate [5]. Particularly in Japan, MPO–ANCA-associated glomerulonephritis has been confirmed to be a major type of RPGN [6]. Vasculitis plays a major role in the pathogenesis of the MPO–ANCA-associated glomerulonephritis, although it has not yet been fully clarified how ANCA induce vasculitis [7, 8]. The lungs and kidneys are the main target organs in MPO–ANCA-associated vasculitis [1, 5]. Various forms of pulmonary involvement have been reported. Interstitial pneumonia (IP), as well as pulmonary hemorrhage, is a frequent and a lifethreatening complication in patients with MPOANCA-associated glomerulonephritis in Japan. [5].
In our patient, treatment with corticosteroid prevented the deterioration of her renal function and further improved it. However, her IP worsened during the course of tapering the prednisolone doses. Although it is possible that certain microorganisms, such as viruses, fungus, and Pneumocystis spp. had participated in the worsening of her lung lesion, bacteriological examinations of sputa and BAL fluid did not demonstrate pathogenic microorganisms. It is known that diffuse alveolar hemorrhage is mainly due to alveolar capillaritis; however, the pathogenesis of IP remains unclear [1]. Recurrent occult alveolar hemorrhage has been suggested as a putative mechanism leading to pulmonary fibrosis in patients with ANCA-associated vasculitis [9]. Alternatively, the authors of several studies have suggested that MPO antibodies may cause pulmonary tissue injury through the release of products of activated neutrophils [10]. In our patient, occult alveolar hemorrhage was not suggested based on the results of her BAL examination. It is possible that the tapering of prednisolone doses caused exacerbation of the IP, although the pathogenesis of her IP remains unknown. We did consider increasing the prednisolone doses or administering other immunosuppressant for treating her IP. However, we decided to observe her condition carefully without additional immunosuppressive therapy because the clinical course was not so fulminant and infections can be a cause of fatal complications, especially in elderly patients. As a result, her IP improved with continuation of 25 mg/day of prednisolone.
Recent studies have revealed that serum levels of SP-A, SP-D and KL-6 reflect the disease activity of IP. SP-A and SP-D are collagenous glycoproteins with multiple functions in the lung. Serum levels of SP-A and SP-D have been reported to be increased in patients with alveolar proteinosis, idiopathic pulmonary fibrosis and acute respiratory distress syndrome [2, 3]. Takahashi et al. [3, 11] reported that serum levels of SP-A and SP-D are useful biomarkers for idiopathic pulmonary fibrosis and interstitial lung disease complicated by progressive systemic sclerosis. On the other hand, KL-6 is a mucinous glycoprotein, expressed on type 2 pneumocytes and bronchial epithelial cells, and the serum level of KL-6 has been reported as a serum indicator of IP [4]. In patients with ANCA-associated vasculitis, Iwata et al. [12] reported that the measurement of serum KL-6 levels may be a good monitoring system for the diagnosis and follow-up of IP. However, there are few reports on the simultaneous monitoring with serum SP-A, SP-D and KL-6 in patients with ANCA-associated IP [13].
On admission, our patient had serum levels of SP-A, SP-D and KL-6 that were almost within the normal range. We speculate that the patent’s IP was inactive on admission, although her chest radiograph and CT suggested mild IP. The serum levels of these markers rose when the patient’s IP deteriorated. In accordance with improvement of her clinical symptoms and lung lesions, the serum level of SP-D first decreased and then SP-A and KL-6 levels decreased. These data suggest that the SP-D level may have been a sensitive marker of IP disease activity in our patient. Takahashi et al. [9] demonstrated that SP-D is more useful than SP-A in detecting interstitial lung disease in patients with progressive systemic sclerosis. Since the serum MPO–ANCA remained negative in our patient when her IP deteriorated, the serum MPO–ANCA level may not be a reliable marker for monitoring disease activity in the lungs.
This case report suggests that monitoring with serum SP-A, SP-D and KL-6 may be helpful when interstitial lung lesions develop or worsen in a patient with ANCA-associated vasculitis during the course of immunosuppressive therapy. Further studies involving more patient data are needed to clarify the clinical importance of these markers in ANCA-associated IP.
Conflict of interest
None.
References
- 1.Bosch X, Mirapeix E, Font J, Cervera R, Ingelmo M, Khamashta MA, et al. Anti-myeloperoxidase autoantibodies in patients with necrotizing glomerular and alveolar capillaritis. Am J Kidney Dis. 1992;20:231–239. doi: 10.1016/s0272-6386(12)80695-0. [DOI] [PubMed] [Google Scholar]
- 2.Mason RJ, Greene K, Voelker DR. Surfactant protein A and surfactant protein D in health and disease. Am J Physiol. 1998;275(1 Pt 1):L1–L13. doi: 10.1152/ajplung.1998.275.1.L1. [DOI] [PubMed] [Google Scholar]
- 3.Takahashi H, Fujishima T, Koba H, Murakami S, Kurokawa K, Shibuya Y, et al. Serum surfactant proteins A and D as prognostic factors in idiopathic pulmonary fibrosis and their relationship to disease extent. Am J Respir Crit Care Med. 2000;162:1109–1114. doi: 10.1164/ajrccm.162.3.9910080. [DOI] [PubMed] [Google Scholar]
- 4.Ohnishi H, Yokoyama A, Kondo K, Hamada H, Abe M, Nishimura K, et al. Comparative study of KL-6, surfactant protein-A, surfactant protein-D, and monocyte chemoattractant protein-1 as serum markers for interstitial lung disease. Am J Respir Crit Care Med. 2002;165:378–381. doi: 10.1164/ajrccm.165.3.2107134. [DOI] [PubMed] [Google Scholar]
- 5.Yamada H. ANCA: associated lung fibrosis. Semin Respir Crit Med. 2011;32:322–327. doi: 10.1055/s-0031-1279828. [DOI] [PubMed] [Google Scholar]
- 6.Yamagata K, Usui J, Saito C, Yamaguchi N, Hirayama K, Mase K, et al. ANCA-associated systemic vasculitis in Japan: clinical features and prognosis. Clin Exp Nephrol. 2012;16:580–588. doi: 10.1007/s10157-012-0598-2. [DOI] [PubMed] [Google Scholar]
- 7.Muller Kobold AC, van der Geld YM, Limburg PC, Tervaert JW, Kallenberg CG. Pathophysiology of ANCA-associated glomerulonephritis. Nephrol Dial Transplant. 1999;14:1366–1375. doi: 10.1093/ndt/14.6.1366. [DOI] [PubMed] [Google Scholar]
- 8.Xiao H, Heeringa P, Hu P, Liu Z, Zhao M, Aratani Y, et al. Antineutrophil cytoplasmic autoantibodies specific for myeloperoxidase cause glomerulonephritis and vasculitis in mice. J Clin Invest. 2002;110:955–963. doi: 10.1172/JCI0215918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Tzelepis GE, Kokosi M, Tzioufas A, Toya SP, Boki KA, Zormpala A, et al. Prevalence and outcome of pulmonary fibrosis in microscopic polyangiitis. Eur Respir J. 2010;36:116–121. doi: 10.1183/09031936.00110109. [DOI] [PubMed] [Google Scholar]
- 10.Foucher P, Heeringa P, Peterson AH, Huitema MG, Brouwer E, Tervaert JW, et al. Antimyeloperoxidase-associated lung disease. An experimental model. Am J Respir Crit Care Med. 1999;160:987–994. doi: 10.1164/ajrccm.160.3.9807139. [DOI] [PubMed] [Google Scholar]
- 11.Takahashi H, Kuroki Y, Tanaka H, Saito T, Kurokawa K, Chiba H, et al. Serum levels of surfactant proteins A and D are useful biomarkers for interstitial lung disease in patients with progressive systemic sclerosis. Am J Respir Crit Care Med. 2000;162:258–263. doi: 10.1164/ajrccm.162.1.9903014. [DOI] [PubMed] [Google Scholar]
- 12.Iwata Y, Wada T, Furuichi K, Kitagawa K, Kokubo S, Kobayashi M, et al. Serum levels of KL-6 reflect disease activity of interstitial pneumonia associated with ANCA-related vasculitis. Intern Med. 2001;40:1093–1097. doi: 10.2169/internalmedicine.40.1093. [DOI] [PubMed] [Google Scholar]
- 13.Fujita S, Hirayama K, Ogawa Y, Shimohata H, Kobayashi M. Mizoribine reduces serum KL-6 levels in ANCA-associated vasculitis. Clin Exp Nephrol. 2010;14:203–204. doi: 10.1007/s10157-009-0250-y. [DOI] [PubMed] [Google Scholar]