

Abstract
Cosmetic tattooing has become a risk factor for several adverse reactions related to inks, procedures, and associated clinical conditions. Development of a sarcoid reaction to the inserted tattoo pigment in the skin is not common. We report a 45 year-old patient with history of dyspnea and mild cough since two years who had subsequently developed reddish, scaly lesions in her 15-year old tattoo done near her right eyebrow. Skin biopsy of the tattoo lesion revealed cutaneous sarcoidosis which led to further investigations and a diagnosis of pulmonary sarcoidosis. The present case highlights the fact that cutaneous sarcoidosis can develop in a long-standing tattoo. Also such a patient should be screened for systemic sarcoidosis disease.
KEY WORDS: Cosmetic tattoo, cutaneous sarcoidosis, lungs, pulmonary sarcoidosis
Introduction
Sarcoidosis is a multisystem granulomatous disorder that is manifested by the formation of granulomas without central necrosis. The origin of this disorder is not clear. Sarcoidosis occurs worldwide, with a female predominance. People aged between 20 and 39 years are more susceptible to this disease.[1] Most cases manifest with cough and dyspnea because of the involvement of the lungs.[1] This disease can affect any part of the body, but the lungs and mediastinal lymph nodes and the skin, heart, eyes, and joints are mostly involved in a majority of patients.[2] Chest imaging and multidetector computed tomography are usually performed to confirm the final diagnosis of this disorder.[1,3] Nevertheless, the skin lesions may be the only sign of sarcoidosis. Hence, taking a skin biopsy may aid in prompt diagnosis of the disease, particularly of scars or sites of trauma, such as that caused by tattooing.[4] Permanent makeup is a type of cosmetic tattoo, in which the colorants (pigments) are deposited in the dermis after piercing the skin using tiny solid needles. Adverse effects such as local inflammation, infection, and allergic reactions on the skin and even systemic adverse effects such as sarcoidal reactions are common.[5] The important histopathological finding of sarcoidosis is the existence of noncaseating granulomas devoid of prominent infiltrates of lymphocytes or plasma cells.[6] This pattern may be seen in other disorders.[4] Sarcoidal granulomas in cosmetic tissues are a sign of cutaneous sarcoidosis and may be associated with systemic sarcoidosis. We describe a case of cutaneous sarcoidosis in a long-lasting cosmetic tattoo reaction, which led to the diagnosis of pulmonary sarcoidosis.
Case Report
A 45-year-old female was referred to the dermatology clinic of our hospital with a 15-month history of lesions on her tattoo. Her tattoos had red, scaly patches. She previously had a black tattoo for 10 years, without any adverse event. Her medical and family histories were unremarkable, except for development of chronic exertional dyspnea and a mild cough 9 months before the development of the skin lesions. She had no history of joint pain or other cutaneous skin lesion. On examination of the tattoo, the tail of her tattoo was slightly raised with fine scaling [Figure 1]. The results of a skin biopsy demonstrated nonnecrotizing granulomas with few lymphocytes around the granuloma and negative results on acid-fast Bacillus and fungal stains [Figure 2]. In addition, the chest imaging revealed perihilar lymphadenopathy and few small nodules in both lungs [Table 1]. Interstitial markings, especially in the peripheral part of the lungs, were increased and peribronchial cuffing was detected [Figure 3].
Figure 1.
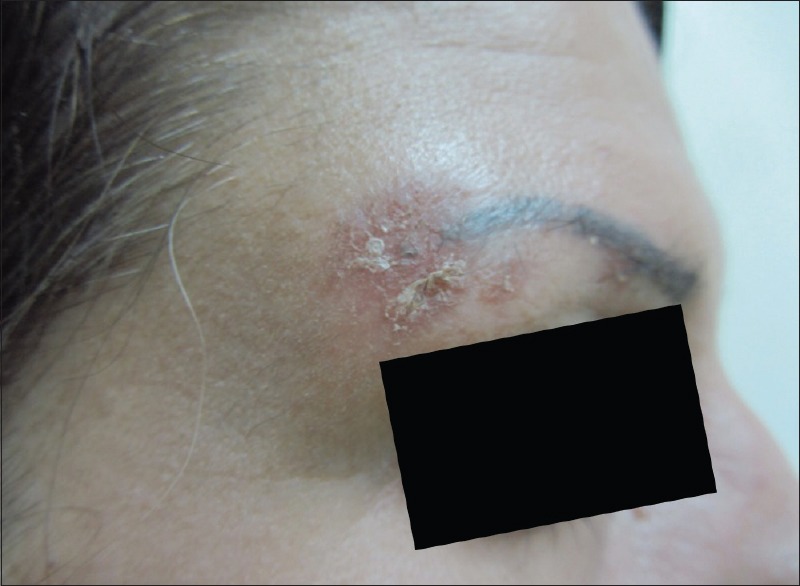
Cutaneous sarcoidosis lesion in the cosmetic eyebrow tattoo
Figure 2.
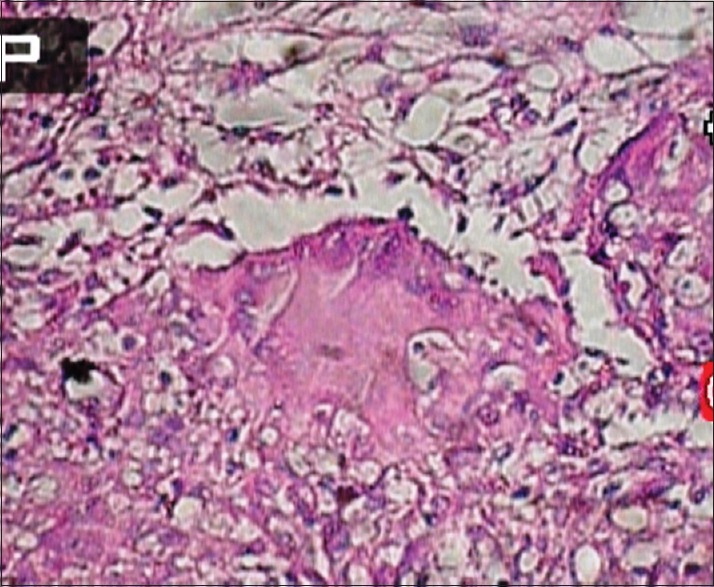
Histopathology of skin biopsy taken from cutaneous lesion showing infiltration of few lymphocytes around the nonnecrotizing granulomas indicative of cutaneous sarcoidosis
Table 1.
Radiographic stages of pulmonary sarcoidosis
| Stage | Chest X-ray findings |
|---|---|
| I | Bilateral hilar adenopathy |
| II | Bilateral hilar adenopathy and diffuse reticulonodular opacities |
| III | Reticulonodular pattern |
| IV | Fibrosis |
Figure 3.
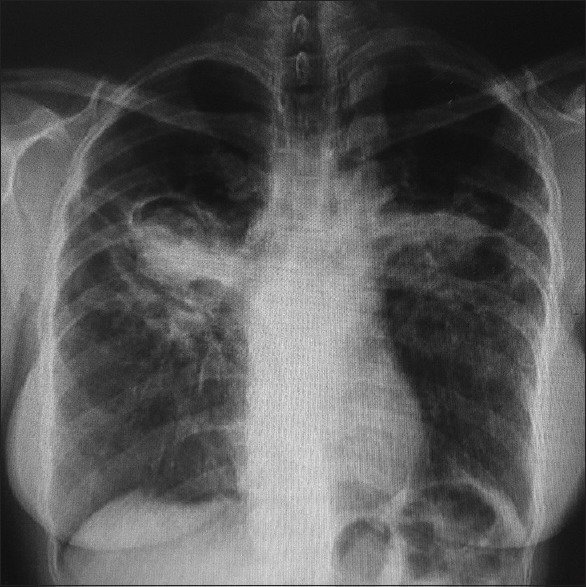
Chest x-ray of patient showing bilateral hilar lymphadenopathy and few diffuse reticulonodular opacities in both lung fields
Investigations for sarcoidosis, as well as for ophthalmologic and respiratory consultations, were conducted. Blood tests revealed an abnormally high level of angiotensin-converting enzyme (ACE). The ACE level was 65 U/L (normal range up to 50 U/L). A high-resolution computed tomographic scan revealed a diffuse increase in the interstitial markings (stage II pulmonary sarcoidosis) and mediastinal adenopathy. A diagnosis of pulmonary sarcoidosis was supported by the presence of cutaneous sarcoidal granulomas. The patient was treated with oral prednisone 25 mg/day for 12 weeks. The dose of prednisone was tapered to 10 mg/day for maintenance therapy (for 6 weeks). The patient was administered a potent topical steroid for her cutaneous sarcoidosis lesion on her eyebrow for 6 weeks; followed by pimecrolimus 1% cream as maintenance treatment (for 6 weeks). On follow-up at 24 weeks the skin lesion had significantly improved; with the scaling and erythema being negligible.
Discussion
Generally, tattoo pigments are well tolerated by the skin. Cosmetic tattooing has, however, become a risk factor for several adverse reactions related to inks, procedures, and settings.[5] These range from simple infections at the site; transmission of infection, for example, syphilis, tuberculosis, and hepatitis; to allergic reactions to the pigments used, usually mercury.[5] Both infectious and noninfectious adverse reactions have been observed in otherwise healthy people with significant morbidity.[5] “Sarcoid” reactions to pigment placement in the skin are not uncommon, but the development of tattoo granulomata as a presenting feature of sarcoidosis is rare.[5] Tattoo sarcoidosis occurs in two different clinical settings. A tattoo may become involved after several years as a part of idiopathic sarcoidosis usually in the absence of other cutaneous or systemic lesions. In contrast, the tattoo pigment may elicit granulomatous hypersensitivity and induce systemic sarcoidosis.[7] While the involvement of a scar or tattoo in systemic sarcoidosis is rare, tattoo sarcoidosis has been reported as a presenting sign of systemic sarcoidosis.[8] The latency period between the act of tattooing and the development of cutaneous symptoms varies.[8] In the current case, the patient manifested with dyspnea and a mild cough, 9 months before the development of the cutaneous sarcoidosis lesion. Hence it is likely that pulmonary sarcoidosis developed before the cutaneous sarcoidosis lesion. There was a interval of 15 years between the cosmetic tattooing of the eyebrow and the diagnosis of cutaneous and pulmonary sarcoidosis, reflecting the complexity of this association. This latency period may vary from 1 to >30 years.[9]
In conclusion, the present case highlights the fact that cutaneous sarcoidosis can develop in a long-standing tattoo. Also such a patient should be screened for systemic sarcoidosis disease.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Aksoy SY, Özdemir E, Sentürk A, Türkölmez S. A case of sarcoidosis diagnosed by positron emission tomography/computed tomography. Indian J Nucl Med. 2016;31:198–200. doi: 10.4103/0972-3919.183608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Moccia LG, Castaldo S, Sirignano E, Napolitano M, Barra E, Sanduzzi A. Sarcoidosis with prevalent and severe joint localization: A case report. Multidiscip Respir Med. 2016;11:27. doi: 10.1186/s40248-016-0064-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Akira M, Kozuka T, Inoue Y, Sakatani M. Long-term follow-up CT scan evaluation in patients with pulmonary sarcoidosis. Chest. 2005;127:185–91. doi: 10.1378/chest.127.1.185. [DOI] [PubMed] [Google Scholar]
- 4.Miida H, Ito M. Tuberculoid granulomas in cutaneous sarcoidosis: A study of 49 cases. J Cutan Pathol. 2010;37:504–6. doi: 10.1111/j.1600-0560.2009.01337.x. [DOI] [PubMed] [Google Scholar]
- 5.Kluger N. Cutaneous and systemic complications associated with tattooing. Presse Med. 2016;45:567–76. doi: 10.1016/j.lpm.2016.02.016. [DOI] [PubMed] [Google Scholar]
- 6.Ball NJ, Kho GT, Martinka M. The histologic spectrum of cutaneous sarcoidosis: A study of twenty-eight cases. J Cutan Pathol. 2004;31:160–8. doi: 10.1111/j.0303-6987.2004.00157.x. [DOI] [PubMed] [Google Scholar]
- 7.Antonovich DD, Callen JP. Development of sarcoidosis in cosmetic tattoos. Arch Dermatol. 2005;141:869–72. doi: 10.1001/archderm.141.7.869. [DOI] [PubMed] [Google Scholar]
- 8.Landers MC, Skokan M, Law S, Storrs FJ. Cutaneous and pulmonary sarcoidosis in association with tattoos. Cutis. 2005;75:44–8. [PubMed] [Google Scholar]
- 9.Hanada K, Chiyoya S, Katabira Y. Systemic sarcoidal reaction in tattoo. Clin Exp Dermatol. 1985;10:479–84. doi: 10.1111/j.1365-2230.1985.tb00609.x. [DOI] [PubMed] [Google Scholar]