

Abstract
The acceptance for innovation by Rogers
![]()
The International Diabetes Federation estimated that there are approximately 415 million people with diabetes in 2015 worldwide, and this number is expected to increase to 642 million by 20401. Almost half of the people with diabetes remain undiagnosed and are from developing countries. Early interventions, such as screening or lifestyle regulation for diabetes at the asymptomatic stage, are effective preventive strategies for diabetes and its complications. However, the incidence and prevalence rates of diabetes are increasing worldwide, particularly in minority groups. Therefore, the traditional diabetes prevention model certainly has some limitations; innovative strategies should thus be developed for diabetes.
Diffusion of innovation (DOI) theory can provide a brief model to disseminate novel diabetes prevention strategies2. DOI theory has been applied in different fields to understand how people translate new ideas, such as new treatment skills, disease knowledge or educational strategies, into real world applications. To improve effective outcomes by disseminating intervention strategies, DOI theory encourages the application of high‐technology media and mass media with rapid transmission characteristics to meet the demand of health needs, such as diabetes care.
Tracing back to the concept of this theory, ‘diffusion of innovation’ can be divided into two parts: innovation and diffusion. ‘Innovation’ refers to modern, novel ideas or thoughts; practices, products, services or devices useful to applicants; or novel programming advantageous to an individual or group. Innovation not only includes the adoption of novelty, but also involves the modification of the attitudes and behavior of individuals or groups. An innovation is neither objectivly identified by whether the new or old depends on the time, nor the invention of something first used. When groups or individuals subjectively accept or recognize something as ‘new,’ this constitutes innovation. ‘Diffusion’ is the process by which an innovation is communicated within a specific period. By sharing information through particular channels, individuals can disseminate innovativeness to their social networks to reach a certain level of consensus.
From ecological aspects, DOI theory is a macrolevel theory in which community‐level innovations are adopted to change a population's health behavior. In the other part, DOI theory aims to understand how an advantageous innovation can be rapidly disseminated or diffused. Diffusion of the innovation can occur through planned or occasional transmission. For example, multidisciplinary sharecare programs for people with diabetes are a type of planned promotion of information. For instance, a family‐based diabetes prevention strategy includes families, doctors, nurses, dieticians and physical therapists for the integration of healthcare services to ensure the quality of diabetes care3. By analyzing the past experience and characteristics of adopters, and how related factors affect their decision‐making process regarding innovation adoption, we can evaluate their acceptance rate and satisfaction level or other unexpected consequences. In general, decision‐making by individuals is more rapid than that by an organization or a group. Therefore, to increase the acceptance rate, we should change the decision‐making type to focus on the opinion of society leaders first by using their authority to influence the innovation rate. For example, public health nurses and diabetes educators can persuade people in a community to undergo diabetes screening regularly, regulate their diet intake and engage in exercise. Early detection of asymptomatic hyperglycemia can ensure early treatment. Alternatively, health‐care professionals can motivate the public to accept a new lifestyle modification program to reduce the incidence of diabetes. The main objectives of innovative strategies are to not only provide knowledge, but ensure diffusion of the innovation and its acceptance by the population for a sustained long‐term effect.
According to Rogers4, personal characteristics influence whether people adopt an innovation rapidly. Based on the innovativeness degree of the adopters’ characteristics, adopters can be divided into five categories that follow an S‐curve (Figure 1). The first 2.5% of individuals in a system who adopt an innovation are called ‘innovators.’ They are the pioneers with the most courage to accept the innovation. The next 13.5%, called ‘early adopters,’ are the stakeholders in a social system and usually lead people to change. They seek information and advice from the pioneers, and their acceptance behavior is the most appropriate endorsement of innovators. The third group, named the ‘early majority,’ occupies the area between 1 standard deviation and the median under the curve; people in this group have higher alert and interests in new ideas, but adopt these ideas after others’ successful experiences. They mainly learn from their close associates, and rely on personal communication channels to diffuse the innovation. They are more risk‐averse than early adopters, and they will take a longer time to evaluate all possibilities before accepting the innovation. The fourth group, named the ‘late majority,’ adopts the innovation after the left half of the population under the curve. They are usually more conservative, cautious and suspicious, even though the innovation has been safely tried by most of the early majority and early adopters. The main reasons for the delay in adoption are the uncertainties and caution caused by the limitation of resources or inadequate information. The last group is named ‘laggards.’ They are conservatives or vulnerable groups with the fewest resources, limited information and unstable incomes, or are isolated from the social support system. They fall behind due to the neglect of social system.
Figure 1.
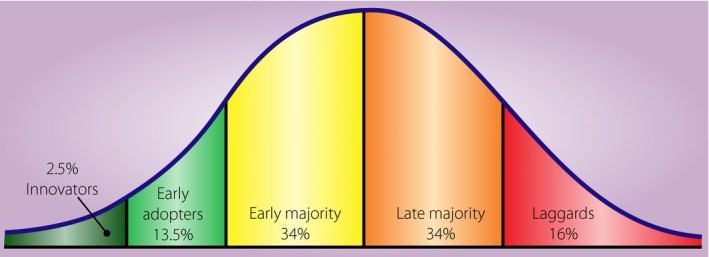
The order to accept the innovation: Innovators (<2.5%, dark green), Early adopters (2.5~16%, light green), Early majority (16~50%, yellow), Late majority (50~84%, orange) and Laggards (84~100%, red).
Rogers4 considered adoption to be a complex psychosocial process. Therefore, the barriers to adoption processes should be considered. For example, even with evidence that healthy habits and environmental conditions majorly improve health, some patients still do not change their existing unhealthy habits to adopt a suggested lifestyle modification. This inability to change is a barrier of the adoption process. People have their own living environment in a social circumstance. Through daily social networking, they continually interact with others to exchange information, experiences and ideas; thus, frequent interaction leads to the dissemination of new ideas.
Adopters are empowered through self‐efficacy. Self‐efficacy refers to an individual's belief in his/her capacity to execute actions to achieve personal health goals. People with higher self‐efficacy show a higher motivation for personal change. Furthermore, Rogers4 suggested that five factors influence whether an innovation will be successfully adopted and diffused from person to person: relative advantage, compatibility, complexity, trialability and observability. Compared with traditional ideas, innovations should have advantages, such as cost‐effectiveness or time‐saving properties, and should be compatible with legacy knowledge, as well as lower complexity and easy testability and observability in usual life. Mass media and news events can be used to increase the visibility and prominence of innovations, or interpersonal communication can be used to disseminate innovations successfully in the society.
In recent decades, DOI theory has been widely applied to public health and medical care for achieving effective disease prevention. General physicians conventionally diagnose and treat diseases. In Australia, they were encouraged to become innovative health promoters within the model of continuity of care. With this DOI concept, the prevalence of tobacco use reduced from 40% in 1983 to 15.9% in 20105. With an increasing number of electronic tools, DOI will become much easier. In Canada, physicians, nurses and patients responded well to innovative diabetes education, and social mobilization contributed the most to successful diffusion of the innovation program2.
In conclusion, DOI theory emphasizes applying social marketing techniques and social networking as communication channels to rapidly disseminate an innovation. Health professionals should not only provide conventional educational strategies, but also implement innovative strategies for diabetes care considering patients’ needs.
Disclosure
The authors declare no conflict of interest.
Acknowledgment
This research was supported partly by the Ministry of Science and Technology (MOST‐104‐2314‐B‐002 ‐155).
References
- 1. International Diabetes Federation . IDF Diabetes Atlas, 7th edn International Diabetes Federation, 2015. Available from: http://www.diabetesatlas.org/. [Google Scholar]
- 2. De Civita M, Dasgupta K. Using diffusion of innovations theory to guide diabetes management program development: an illustrative example. J Public Health 2007; 29: 263–268. [DOI] [PubMed] [Google Scholar]
- 3. Greenhalgh T, Robert G, Macfarlane F, et al Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Q 2004; 82: 581–629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Rogers EM. Diffusion of Innovations, 4th edn New York: Simon and Schuster, 2010. [Google Scholar]
- 5. McManus A. Health promotion innovation in primary health care. Australas Med J 2013; 6: 15–18. [DOI] [PMC free article] [PubMed] [Google Scholar]