

Abstract
Subarachnoid hemorrhage is a common manifestation of traumatic brain injury. A clinical deterioration in Glasgow Coma Scale score without an accompanying radiological worsening is suggestive of vasospasm. However, hyperemia could be another possibility which can easily be considered with corroborating transcranial Doppler (TCD) features. This case report reiterates the value of TCD in such instances.
Keywords: Hyperemia, traumatic brain injury, traumatic subarachnoid hemorrhage
INTRODUCTION
Subarachnoid hemorrhage (SAH) is one of the most common radiological features of traumatic brain injury (TBI) occurring in 30%–40% of moderate–severe head injuries.[1,2] Vasospasm and resulting cerebral ischemia as well as cerebral hyperemia can cause delayed neurological recovery and poor outcome.[3,4,5] We illustrate a case where differentiating the two entities enabled a good neurological recovery.
CASE REPORT
A 56-year-old male suffered a moderate head injury following an alleged road traffic accident and presented to the Neuro Intensive Care Unit with a Glasgow Coma Scale (GCS) score of 11/15. The computerized tomography (CT) scan of brain showed bilateral frontal and right temporal contusion with left Sylvian and temporal SAH. He was treated with antiedema measures, namely, mannitol 1 g/kg and hypertonic saline (3%) at 30 ml/h infusion. It was continued till 48 h posttrauma with a serum sodium target of >140 meq/L. CT scan was repeated when GCS did not improve after 48 h. It showed a relative decrease in cerebral edema compared to the earlier scan. In view of this, antiedema measures were continued for further 2 days. However, there was no improvement in GCS. A transcranial Doppler (TCD) done at this time was suggestive of cerebral hyperemia [Figure 1] with a Lindegaard ratio (LR) of 4. The possibility of vasospasm in view of traumatic SAH was ruled out with a normal digital subtraction angiography (DSA) [Figure 2] done on the 5th posttrauma day. Conservative management was continued and the patient started improving clinically to GCS score of 13/15 on day 7. TCD showed much reduced hyperemia at this point [Figure 3]. He was discharged on the 10th posttrauma day with a GCS score of 15/15.
Figure 1.
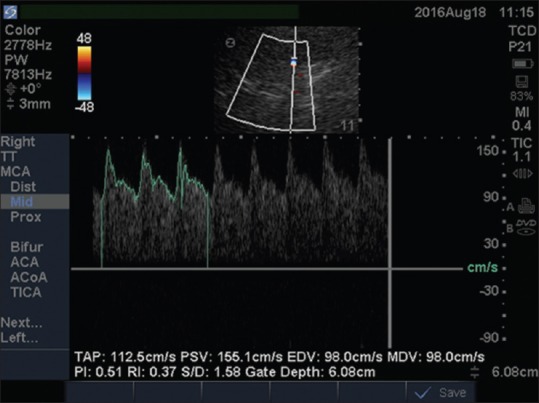
Transcranial Doppler flow with hyperemia of brain
Figure 2.
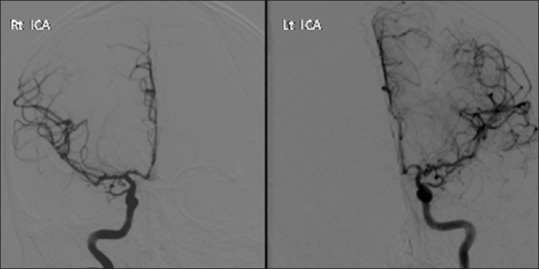
Angiographic image of bilateral internal carotid arteries ruling out vasospasm
Figure 3.
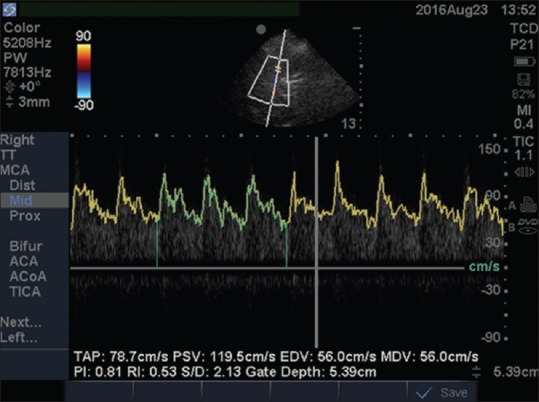
Transcranial Doppler flow when hyperemia reduced
DISCUSSION
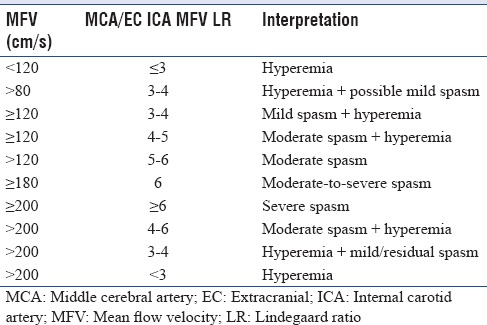
TCD can be an important bedside tool in the management of head injury. In patients with unanticipated delay in improvement of GCS, TCD can play a vital role. The LR calculated as the ratio of mean flow of middle cerebral artery (MCA) and mean flow of extracranial internal carotid artery helps diagnose or rule out vasospasm as a cause.[6] The mean flow velocities of MCA coupled with LR differentiates vasospasm from hyperemia [Table 1].[6,7]
Table 1.
Transcranial Doppler grading criteria for middle cerebral artery vasospasm
As in our case with LR of 4, a definitive DSA was needed to rule out vasospasm.
The significance of hyperemia on the management and clinical outcome of TBI is still unknown. The effect of hyperemia on intracranial pressure (ICP) is a key to predicting clinical outcome. Kelly et al. found hyperemia associated with raised ICP to be a predictor of poor outcome and needing aggressive treatment while mild hyperemia without raised ICP was linked to favorable outcome.[5] In our case, also, mild–moderate hyperemia suggested by LR of 4 and pulsatility index of 0.8 relating to low ICP had a good outcome.
The Doppler waveform suggestive of hyperemia was described by Chan et al. as an absent diastolic notch similar to our recording.[8] The clinical implications of the above-mentioned findings are of uncertain significance. However, as observed in our patient, the resolution of hyperemia coincided with clinical improvement and may just be the temporal profile of the injury.
The popularity of TCD as a bedside tool is hampered by the limitation that it is extremely operator dependent. The angle of insonation and detailed knowledge of cerebral vascular anatomy and its variant limits the interpretation. The acoustic window may not be accessible in 10%–15% patients.[9]
CONCLUSION
This case report highlights the importance of evaluating with TCD for an unexplained persistent low GCS. The differentiation of hyperemia from vasospasm is paramount in management. Cerebral hyperemia may be one of the causes of nonimproving GCS in the early phases of TBI. TCD is a valuable tool in establishing this diagnosis. Once diagnosed, this entity may not need any further treatment other than close neurological observation.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Stiell IG, Wells GA, Vandemheen K, Clement C, Lesiuk H, Laupacis A, et al. The Canadian CT head rule for patients with minor head injury. Lancet. 2001;357:1391–6. doi: 10.1016/s0140-6736(00)04561-x. [DOI] [PubMed] [Google Scholar]
- 2.Roberts I, Yates D, Sandercock P, Farrell B, Wasserberg J, Lomas G, et al. Effect of intravenous corticosteroids on death within 14 days in 10008 adults with clinically significant head injury (MRC CRASH trial): Randomised placebo-controlled trial. Lancet. 2004;364:1321–8. doi: 10.1016/S0140-6736(04)17188-2. [DOI] [PubMed] [Google Scholar]
- 3.Martin NA, Doberstein C, Alexander M, Khanna R, Benalcazar H, Alsina G, et al. Posttraumatic cerebral arterial spasm. J Neurotrauma. 1995;12:897–901. doi: 10.1089/neu.1995.12.897. [DOI] [PubMed] [Google Scholar]
- 4.Miller JD, Dearden NM, Piper IR, Chan KH. Control of intracranial pressure in patients with severe head injury. J Neurotrauma. 1992;9(Suppl 1):S317–26. [PubMed] [Google Scholar]
- 5.Kelly DF, Kordestani RK, Martin NA, Nguyen T, Hovda DA, Bergsneider M, et al. Hyperemia following traumatic brain injury: Relationship to intracranial hypertension and outcome. J Neurosurg. 1996;85:762–71. doi: 10.3171/jns.1996.85.5.0762. [DOI] [PubMed] [Google Scholar]
- 6.Lindegaard KF, Nornes H, Bakke SJ, Sorteberg W, Nakstad P. Cerebral vasospasm diagnosis by means of angiography and blood velocity measurements. Acta Neurochir (Wien) 1989;100:12–24. doi: 10.1007/BF01405268. [DOI] [PubMed] [Google Scholar]
- 7.Alexandrov AV. Cerebrovascular Ultrasound in Stroke Prevention and Treatment. Elmsford, NY: Blackwell; 2004. [Google Scholar]
- 8.Chan KH, Dearden NM, Miller JD, Midgley S, Piper IR. Transcranial Doppler waveform differences in hyperemic and nonhyperemic patients after severe head injury. Surg Neurol. 1992;38:433–6. doi: 10.1016/0090-3019(92)90111-y. [DOI] [PubMed] [Google Scholar]
- 9.Purkayastha S, Sorond F. Transcranial Doppler ultrasound: Technique and application. Semin Neurol. 2012;32:411–20. doi: 10.1055/s-0032-1331812. [DOI] [PMC free article] [PubMed] [Google Scholar]