

Dear Editor,
Skin tumours of the nasal ala are common and surgery is the treatment of choice. Nasal ala reconstruction is challenging due to the reduced mobility and unique features of its thick and sebaceous skin. The natural arc of the ala and its boundary with the cheek are difficult features to reproduce. One should bear in mind the functional and cosmetic risks of nasal ala reconstruction. A distorted nasal contour may impair the nasal valve; the alar rim may notch or elevate; facial symmetry may be disrupted by blunting of the alar crease, trapdooring, bridging of the nasofacial sulcus and poor colour and texture match.
Our aim is to review and compare the functional and cosmetic results of different local flaps used to correct intermediate-thickness defects on the nasal ala after surgical excision of cutaneous tumours. We present representative patients who were treated at our Dermatological Surgery Unit from June 2015 to September 2016.
The choice of the flap was adapted to the patients' physiognomy and the defects' size: tunnelled island pedicle melolabial flap [Figure 1]; jigsaw puzzle advancement flap [Figure 2]; spiral flap [Figure 3]; dog-ear island pedicle flap [Figure 4] and banner melolabial transposition flap [Figure 5]. Surgery was performed under loco-regional anaesthesia, in an outpatient basis, followed by prophylactic antibiotic therapy. There were neither immediate complications nor subsequent flap necrosis. The tumours were completely excised.
Figure 1.

Female, 86-year-old, nodular ulcerated basal cell carcinoma in the nasal ala: tunnelled island pedicle melolabial flap. (a) Surgical plan, (b) primary defect, (c) secondary defect after tunnelling of the flap, (d) immediate post-operative, (e and f) result after healing (10 months after surgery)
Figure 2.

Male, 76-year-old, nodular basal cell carcinoma on the nasal ala: jigsaw puzzle advancement flap. (a) surgical plan, (b) primary and secondary defects, (c) anchoring sutures secure the flap in place; (d) immediate post-operative, (e) result after healing (3 months after surgery)
Figure 3.

Female, 76-year-old, nodular basal cell carcinoma on the nasal ala: spiral flap, a combination of advancement and rotation. (a) Surgical plan, (b) immediate post-operative, (c) result after healing (2 months after surgery)
Figure 4.

Female, 76-year-old, basal cell carcinoma on the nasal ala: dog-ear island flap, combining two flaps: cheek advancement and rotated island pedicle. (a) Surgical plan, (b) primary defect, (c) immediate post-operative, (d) day 7 post-operative, (e) result after healing (1 month after surgery)
Figure 5.

Male, 83-year-old, two nodular basal cell carcinomas on the nasal ala and dorsum: Banner's melolabial transposition flap. (a) Surgical plan, (b) primary defect, (c) immediate post-operative, (d) result after healing (7 months after surgery)
Facial symmetry was well preserved by the spiral and jigsaw puzzle flaps [Figures 2 and 3]. The nasal sulcus was left intact by the spiral flap as well as the tunnelled melolabial island flap [Figures 1 and 3]. The melolabial flaps and the dog-ear island flap allowed for the correction of larger defects on the nasal ala [Figures 1, 4 and 5]. The dog-ear island flap [Figure 4] obtained a good result despite the large size of the primary defect. Banner's melolabial transposition flap [Figure 5] was used to correct a complex defect involving not only the nasal ala but also the nasal dorsum and resulted in facial asymmetry due to trapdooring.
The small size of the defects that can be addressed by the spiral and puzzle flaps may explain their superior cosmetic results.[1,2] The tunnelled melolabial island flap, although technically demanding, may produce excellent results; compared to the cheek-to-nose interpolation flap, the tunnelling technique offers the advantage of being one-stage procedure. The dog-ear island flap is an adaptation of the cheek advancement flap; despite its apparent complexity, it offers a viable alternative to the melolabial flaps,[3] with a lower risk of trapdoor effect and with proper preservation of the alar contour. The discussed flaps are useful alternatives to the bilobed transposition flap and the skin graft for the surgical reconstruction of the nasal ala.
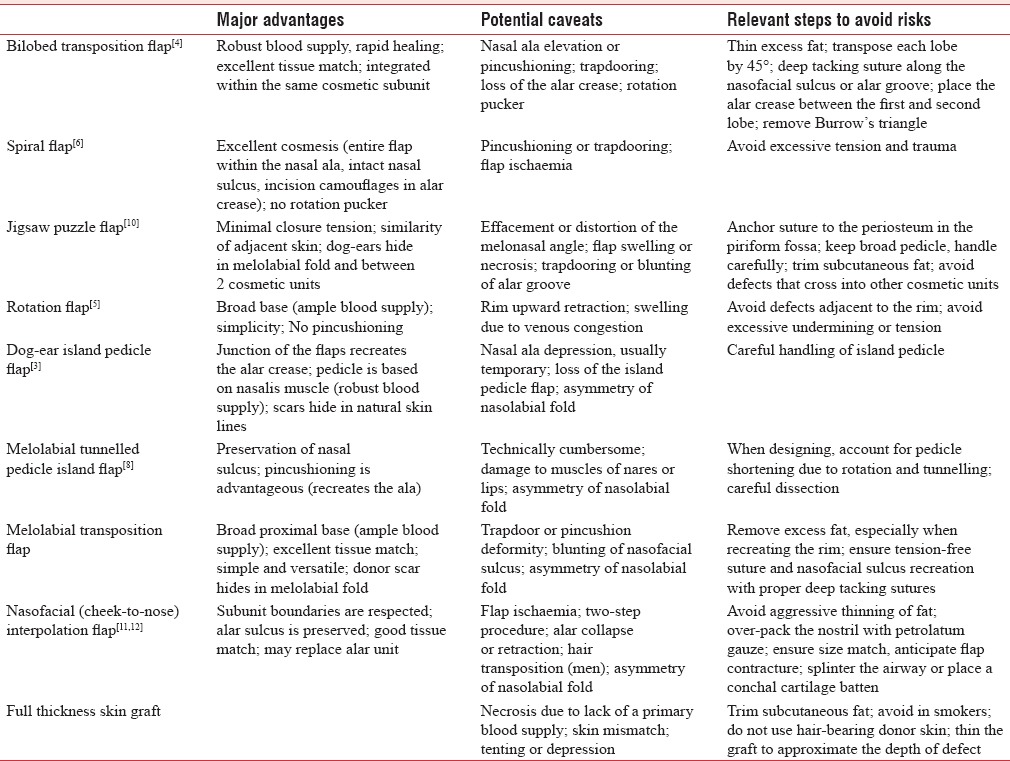
When planning the surgery, it is important to assess the primary defect on the nasal ala: size and location (medial or lateral), depth, involvement of other cosmetic units/subunits and extension to the alar rim, nasal tip or adjacent cheek. Several techniques have been developed that are useful for the reconstruction of defects of the nasal ala. Based on our experience and a review of the literature, we present an algorithm [Table 1] to optimise the choices in the reconstruction of intermediate-thickness defects in nasal ala. In Table 2, we review the main advantages and caveats of some of the most useful surgical techniques for nasal ala reconstruction.[4,5,6,7,8,9,10,11,12,13,14]
Table 1.
Nasal ala reconstruction: What is the optimal approach according to the defects' size and location?
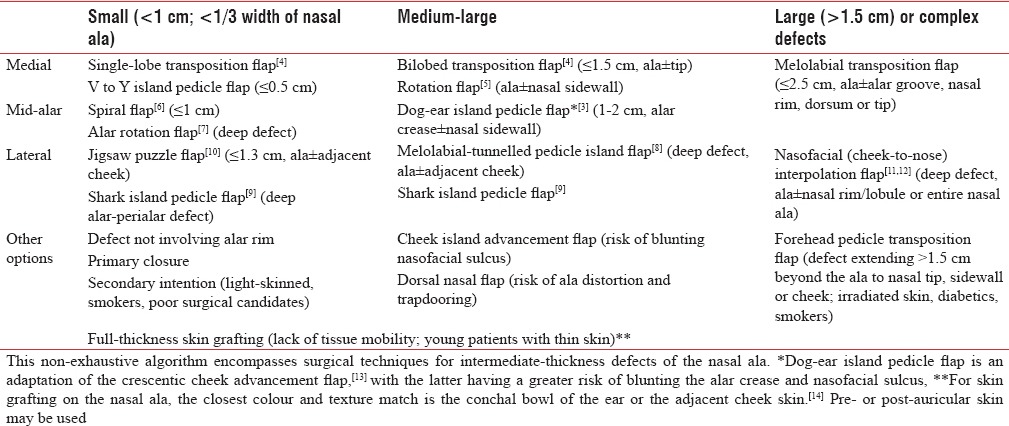
Table 2.
Nasal ala reconstruction: major advantages and potential caveats of different surgical techniques
In the nasal ala, given the paucity of surrounding skin and the importance of minimising nasal ala distortion, flaps that recruit skin from a distant site should be considered. Mastering different techniques is essential for a surgeon to optimise treatment for each patient. At the end of the day, the best choice depends on many factors and should be adapted on a case-by-case basis and to the surgeon's expertise.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgements
We thank the keen devoted nursing team who makes all the work possible.
REFERENCES
- 1.Goldberg LH, Kimyai-Asadi A, Silapunt S. In: “Jigsaw Puzzle” Advancement Flap for Repair of a Surgical Defect Involving the Lateral Nasal Ala, in Reconstructive Conundrums in Dermatologic Surgery: The Nose. Ratner D, Cohen JL, Brodland DG, editors. Chichester, UK: John Wiley & Sons, Ltd; 2014. pp. 93–5. [DOI] [PubMed] [Google Scholar]
- 2.Ascari-Raccagni A, Dondas A, Righini MG, Trevisan G. A “skin helix” flap to correct circular skin loss on the nasal ala. Acta Dermatovenerol Alp Pannonica Adriat. 2010;19:11–4. [PubMed] [Google Scholar]
- 3.Zeikus P, MacCormack M, Olbricht S. Dog ear island pedicle flap for repair of alar and nasal wall defects. Dermatol Surg. 2008;34:1697–700. doi: 10.1111/j.1524-4725.2008.34349.x. [DOI] [PubMed] [Google Scholar]
- 4.Bloom JD, Ransom ER, Miller CJ. Reconstruction of alar defects. Facial Plast Surg Clin North Am. 2011;19:63–83. doi: 10.1016/j.fsc.2010.10.009. [DOI] [PubMed] [Google Scholar]
- 5.Humphreys TR, Goldberg LH, Wiemer DR. Repair of defects of the nasal ala. Dermatol Surg. 1997;23:335–49. doi: 10.1111/j.1524-4725.1997.tb00059.x. [DOI] [PubMed] [Google Scholar]
- 6.Humphreys TR. Use of the “spiral” flap for closure of small defects of the nasal ala. Dermatol Surg. 2001;27:409–10. doi: 10.1046/j.1524-4725.2001.00197.x. [DOI] [PubMed] [Google Scholar]
- 7.Neltner SA, Papa CA, Ramsey ML, Marks VJ. Alar rotation flap for small defects of the ala. Dermatol Surg. 2000;26:543–6. doi: 10.1046/j.1524-4725.2000.00012.x. [DOI] [PubMed] [Google Scholar]
- 8.Mahlberg MJ. Tunneled melolabial pedicle flap for small but deep lateral alar rim defect. Dermatol Surg. 2013;39:1527–9. doi: 10.1111/dsu.12202. [DOI] [PubMed] [Google Scholar]
- 9.Cvancara JL, Michael Wentzell J. In: Shark Island Pedicle Flap for Repair of Combined Nasal Ala-Perialar Defects, in Reconstructive Conundrums in Dermatologic Surgery: The Nose. Ratner D, Cohen JL, Brodland DG, editors. Chichester, UK: John Wiley & Sons, Ltd; 2014. pp. 85–90. [DOI] [PubMed] [Google Scholar]
- 10.Goldberg LH, Kimyai-Asadi A, Silapunt S. “Jigsaw puzzle” advancement flap for repair of a surgical defect involving the lateral nasal ala. Dermatol Surg. 2005;31:569–71. doi: 10.1111/j.1524-4725.2005.31165. [DOI] [PubMed] [Google Scholar]
- 11.Fader DJ, Baker SR, Johnson TM. The staged cheek-to-nose interpolation flap for reconstruction of the nasal alar rim/lobule. J Am Acad Dermatol. 1997;37:614–9. doi: 10.1016/s0190-9622(97)70180-4. [DOI] [PubMed] [Google Scholar]
- 12.Barlow RJ, Swanson NA. The nasofacial interpolated flap in reconstruction of the nasal ala. J Am Acad Dermatol. 1997;36(6 Pt 1):965–9. doi: 10.1016/s0190-9622(97)80282-4. [DOI] [PubMed] [Google Scholar]
- 13.Yoo SS, Miller SJ. The crescentic advancement flap revisited. Dermatol Surg. 2003;29:856–8. doi: 10.1046/j.1524-4725.2003.29232.x. [DOI] [PubMed] [Google Scholar]
- 14.Rohrer TE, Dzubow LM. Conchal bowl skin grafting in nasal tip reconstruction: Clinical and histologic evaluation. J Am Acad Dermatol. 1995;33:476–81. doi: 10.1016/0190-9622(95)91394-7. [DOI] [PubMed] [Google Scholar]