

Abstract
Hair is venerated, cherished, and desired in societies throughout the world. Both women and men express their individual identities through their hairstyles. Healthy hair contributes to successful social assimilation, employment, and overall quality of life. Therefore, hair loss can have detrimental effects on almost every aspect of a person’s life. In this review, we discuss the myriad of options that aid in concealing and camouflaging hair loss to facilitate a healthier-appearing scalp. Camouflage options for patients who suffer from hair loss include full or partial wigs, hair extensions, concealing powders and sprays, surgical tattoos, and hair transplants. We describe these modalities in detail and discuss their respective advantages and disadvantages.
Keywords: wigs, hair transplant, hair camouflage, hair loss, alopecia, concealing, tattoo, micropigmentation
Introduction
Hair is often associated with an individual’s identity, and its significance reaches beyond the surface. Hair has psychological, social, and sometimes spiritual meaning. Therefore, hair loss can lead to multidimensional issues that affect a patient’s well-being. Fortunately, individuals who suffer from hair loss have a plethora of options available to improve the appearance of their hair. In this comprehensive review, we explore the cultural and psychosocial impacts of hair, discuss hair complements and products, and review more permanent solutions.
Historical significance of hair
Hair has cultural and historical importance that varies from era to era. For example, European value on hair and hairstyles continually changes throughout time. Wealthy women in Western Europe between 1770 and 1790 wore their hair in elaborate arrangements with decorations that sometimes included birdcages (Weitz 2004). During this time, capitalism became more important; therefore, men gained a higher status with a wife who had the time and funds required to maintain such ornate hairstyles. During the nineteenth century, while women of lesser means had less time and money to spend on their hair and wore simple hairstyles, wealthier white women would braid their hair overnight and use flat irons to straighten uncurled parts the next morning. With the twentieth century came the popularity of the “bob” haircut. Hair dying in the 1900s was risqué and usually done in secret. Until the 1940s, hair salons even had separate entrances and private booths for women who wanted to dye their hair.
Hair and quality of life
People value hair for different reasons, but value it nonetheless. Therefore, loss of hair may have psychological consequences. A recent study evaluated the prevalence of psychological disorders in 40 participants with alopecia areata (Fig. 1, Fig. 2) and 40 random control group participants who were matched in age and sex (Aghaei et al. 2014). Participants were given three psychological tests: Beck Depression Inventory, Beck Anxiety Inventory, and Eysenck Personality Questionnaire. A significant difference between the case and control groups existed in the prevalence of depression (p = .008), anxiety (p = .003), and neuroticism (p = .05). No significant difference was appreciated between the duration of the disease, age at disease onset, number of relapses, and intensity of disease. While the case group had a significantly higher prevalence of certain psychological illnesses, it is unclear whether the psychological disorders caused/contributed to the alopecia or if the dermatologic disease negatively impacted the patients’ psychological wellbeing. Further research to explain this relationship is needed.
Fig. 1.

Example of patient with patchy alopecia areata.
Fig. 2.
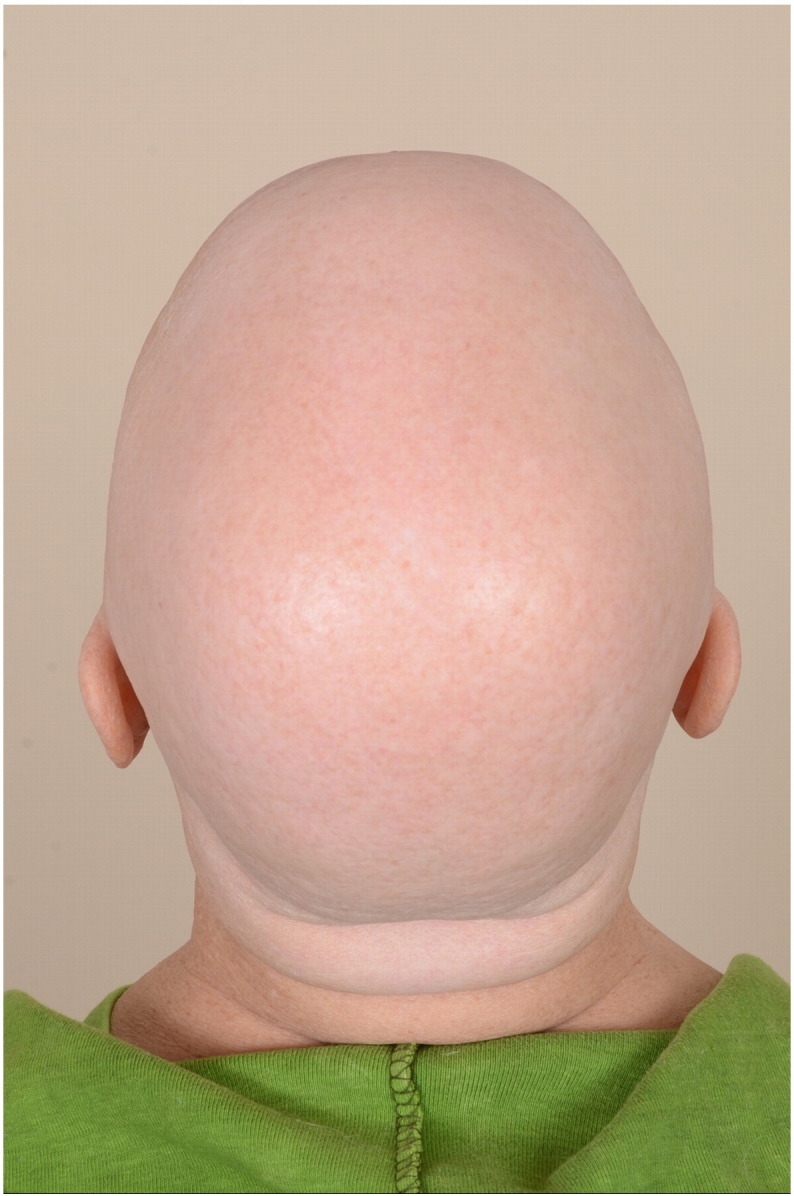
Example of patient with severe alopecia areata, alopecia universalis subtype.
Health-related quality of life in patients with alopecia areata was analyzed from data of 532 patients in the National Alopecia Areata Registry (Shi et al. 2013). The study found that risk factors for poor health-related quality of life included age less than 50 years, female sex, hair loss of 25% to 99%, family stress, and job change. Quality of life is related to emotional wellbeing. In a Canadian study of 35 androgenetic alopecia patients and 42 alopecia areata patients, both groups scored similarly on an emotions assessment, indicating that these patients were less motivated to pursue personal interests and experienced difficulty in coping with stress compared to the controls (Monselise et al. 2013).
In addition to affecting emotions, hair loss may also influence the job market. The Canadian Hair Research Foundation conducted a study among 1,502 men and women to assess the effect of hair loss on employment (Tischer 2000). Of the responders, 1 in 8 believed hair loss to be a barrier to getting hired. Most of those surveyed (81%) believed that physical appearance affects career advancement. Thus, hair loss can shape a person’s wellbeing in deeply meaningful ways.
The psychological effects of hair loss significantly impact patients with cancer who undergo chemotherapy. Among 47% of female cancer patients participating in a study, the most distressingly anticipated aspect of chemotherapy was alopecia (Münstedt et al. 1997). Another study found that the most burdensome part of chemotherapy treatment in women with early stage breast cancer was alopecia (Baxley et al. 1984). An estimated 8% of patients with cancer may be at risk of avoiding treatment due to the consequential hair loss (de Boer-Dennert et al. 1997). A study involving patients with gynecological malignancies reported that 13% of participants anticipated they would be rejected by their significant others as a result of hair loss secondary to treatment (Münstedt et al. 1997). Chemotherapy-induced alopecia can lead to anxiety, depression, reduced quality of life, and decreased self-esteem (Hesketh et al. 2004).
Hair complements
Hair loss can affect a patient’s quality of life. Fortunately, patients have a variety of options available to camouflage, ranging from temporary to nearly permanent. Wigs may be one of the first items that come to mind to conceal hair loss. Patients may be uncomfortable approaching the topic of wigs for alopecia, but the subject deserves discussion, especially with the array of new options available. Wigs are fixed to one of two foundations: wefted, which is the most common and least expensive; or net, the more expensive but more natural-looking option (Donovan et al. 2012).
Wefted foundations have a base of synthetic hair rows that range in price from $60 to $300. Net foundations are a mesh base with synthetic or human hair knotted by hand, which is a more expensive option at $300 to $1,000. For both foundation types, many high-end wigs also have a monofilament cap, which is a fine, transparent nylon lace material (Fig. 3). Hair strands are individually handtied in the lace, allowing for more natural hair movement and styling flexibility. The hairline section of the cap is made in an irregular fashion to resemble the natural pattern of human hairlines (Banka et al. 2012). These wigs generally come with a more expensive price tag of $200 to $2,000. An additional option, lace front wigs place a thin lace material across the frontal hairline (Fig. 4). The lace piece is trimmed and shaped according to the patient’s wishes and can be temporarily glued onto the frontal scalp and/or forehead to achieve a secure hold with every wear.
Fig. 3.

Wig cap with monofilament top, lace front, and handtied back with silicone around the perimeter to allow for better grip of scalp for individuals with total hair loss. Photo courtesy of Hair Enhancements of Pittsburgh (HairEnhancements.net).
Fig. 4.

Lace-front wig cap. Photo courtesy of Hair Enhancements of Pittsburgh (HairEnhancements.net).
The most expensive types of wigs are custom-made wigs with vacuum bases (Donovan et al. 2012). The vacuum base is first made by creating a custom plaster mold of the individual’s scalp. The mold is used to form a silicone or polyurethane vacuum base, a process that can take up to 6 months to do properly.
Wigs can be made either from synthetic or real human hair. Synthetic wig fibers can be machine or hand sewn in the cap, with the latter being more natural-looking but more expensive. Human hair wigs come from China, Thailand, Indonesia, and India. More expensive hair fibers come from Europe. Standard, inexpensive wigs worn daily need to be replaced every 3 to 6 months. High quality human hair wigs can last 3 to 4 years.
Most wigs have Velcro adjustable straps or an adjustable band to help secure them to the scalp. Bonding and taping may be used for attachment but may lead to contact dermatitis, especially from wig adhesives such as acrylates (Torchia et al. 2008). Cases of allergic contact dermatitis to adhesives have been reported, particularly with the widespread use of cyanoacrylate (Sornakumar et al. 2013). Newer hair systems use adhesion on the entire area of attachment to the base, not just the perimeter, making the cap feel more a part of the individual’s scalp (Banka et al. 2012). Other options for wig attachment include taping, which allows for ease of placement and removal; bonds, for longer periods of adhesion; and clips, for temporary attachment that can easily be removed.
An option for patients with hair thinning but not severe hair loss is integration wigs (Donovan et al. 2012). The individual’s hair may be pulled through perforations in the wig to incorporate wig and original hair (Fig. 5). Integration wigs are a widely available option through most companies that sell wigs and hair pieces.
Fig. 5.

Integration wig. Photo courtesy of Hair Enhancements of Pittsburgh (HairEnhancements.net).
Patients with patchy hair loss may prefer the partial coverage of hair pieces or the addition of volume with hair extensions, which are usually made from animal hair such as horse, sheep, or yak hair. Hair extensions are strands of synthetic or human hair that are attached to existing hair fibers by means of glue, braids, sewing, or clips. However, hair extensions may make alopecia worse because of traction. A case study reported on four women who presented with multiple patches of scalp alopecia after use of hair extensions (Yang et al. 2009). A physical examination showed small alopecic erythematous patches at hair extension attachment sites. A dermoscopic evaluation revealed non-scarring alopecia without evidence of alopecia areata. No other areas of alopecia on the scalp or body were noted. The study concluded that traction alopecia can result from constant tension of hair extension on natural hairs and cause the hair shaft to separate from the ostium, resulting in hair loss. Traction alopecia in these cases was initially nonscarring but may lead to scarring or permanent alopecia. Table 1 summarizes and compares the advantages and disadvantages of different types of wigs.
Table 1.
Advantages and disadvantages of natural human hair wigs versus synthetic hair wigs.
| Natural human hair wigs | Synthetic hair wigs |
|---|---|
| Advantages: • Natural appearance because of use of real human hair fibers • May be styled as natural hair • Less susceptible to heat damage • Able to color and perm • Moves like natural hair |
Advantages: • Easy daily maintenance • Less expensive • Less susceptible to fading in sunlight • May be lighter in weight than wigs with human hair • Less odor absorption than wigs with human hair |
| Disadvantages: • More expensive • Needs more maintenance and care • Requires styling • More susceptible to sunlight fading and environmental damage • May be heavier in weight than synthetic wigs, which may lead to itching |
Disadvantages: • Not able to color or perm like human hair • More susceptible to heat damage • May have less natural appearance, movement, and feel • Needs to be replaced more frequently than human hair wigs |
Pigmented concealing powders, lotions, and sprays
Alternative materials can be used to conceal thinning hair. For example, topical hair fibers, which are positively charged particles of wool keratin that adhere to the negatively charged terminal and vellus hair fibers on the scalp, can be used (Donovan et al. 2012). This product requires existing hairs to bind; therefore, this option is ineffective in bald areas. Topical hair fibers are derived from wool or rice keratin, rayon, or human hair and must be applied daily. A popular brand of thinning hair concealer hair fibers is Toppik, which is available online (www.Toppik.com).
Powder cakes, which are circular concealing disks that are applied to the scalp with a sponge, are another option. After application, the hair is brushed to evenly distribute the product. The material is water resistant but can be removed with shampoo. Similar to powder cakes, camouflage lotions and sprays are applied to limit color contrast between existing hair and scalp. Pigmented concealing powders, lotions, and sprays are easy to remove and can apply to various hair colors and styles (Figs. 6A and B; Banka et al. 2012). Also, they may be used alongside medical therapy. Disadvantages of these products include the need for daily application and the fact that water activities may distort the product.
Fig. 6.

(A) Androgenetic alopecia: thinning of the crown and frontal scalp prior to camouflage application. (B) Camouflage powder application resulting in instantly thicker-appearing hair.
Surgical methods
More permanent options for alopecia include surgical hair transplants and micropigmentation. Perhaps the most well-known method to surgically conceal alopecia is hair transplantation, in which hairs are harvested from thicker donor areas on the back of the scalp and implanted in the necessary areas (Fig. 7; Rassman et al. 2015). The two main methods for hair transplantation are follicular unit strip surgery and follicular unit extraction. Follicular unit strip surgery involves the separation of individual follicular units from a linear strip of the donor scalp, leaving behind a linear scar at the donor site (Bernstein and Rassman 1997). In follicular unit extraction, multiple, small (1 mm) punches are used to isolate follicular units (Shin et al. 2015). While the latter has many advantages including the absence of a wide, linear scar, it is far more time consuming than follicular unit strip surgery. Subsequently, a robotic method of follicular unit extraction was developed and approved by the U.S. Food and Drug Administration in 2011 (Shin et al. 2015). The robot is computer-assisted and physician-controlled, allowing for a safe and effective extraction of distinct follicular units from the donor site.
Fig. 7.

Before and 1 year after surgical hair transplantation. Photo courtesy of Dr. Brett Bolton (GreatHairTransplants.com).
Micropigmentation is another more permanent option for hair loss concealment. Van der Velden et al. (1998) describe the medical use of tattooing, specifically in alopecia areata of the eyebrows. Traquina (2001) first reported the use of micropigmentation of the scalp specifically for scalp scars (Figs. 8A and B). Scalp pigmentation is a form of cosmetic tattooing (Rassman et al. 2015). Standard cosmetic tattoo instruments are used along with a specialized technique in order to create the image of pores on a balding scalp (Figs. 9A and B). The process involves the insertion of a pigment through the skin in the upper dermis, using conventional tattoo instruments and artistic and objective judgement on dot placement. The patient will need approximately two to four sessions for completion, with each session lasting up to 8 hours. Risks include infection and allergies to pigment. Needle use carries a risk of infectious disease transmission, such as HIV, hepatitis, and skin infections.
Fig 8.

Linear scar secondary to hair transplantation surgery (A) is concealed with micropigmentation (B). Photos courtesy of Tino Barbone of The Scalp Micropigmentation Center (ScalpMicropigmentationCenter.com).
Fig. 9.

Balding scalp (A) concealed with micropigmentation to mimic pores in scalp (B). Photos courtesy of Tino Barbone of The Scalp Micropigmentation Center (ScalpMicropigmentationCenter.com).
A recent study evaluated the effectiveness of micropigmentation as a scalp camouflage option in 43 Korean patients with alopecia or scalp scars (Park et al. 2014). For the study, the procedure of micropigmentation included the use of a tattoo machine with ink cartridges, insertion of the needle at 90° to the skin, and an appropriate dot-to-dot distance. All patients in the study had black hair so only black pigment was used. Of the 43 patients, only one patient was not satisfied with the results. No complications were reported. In addition to the risk of infection, disadvantages to micropigmentation include the fact that natural hair may grey over time and hair may need to be dyed to match the changing pigment. Also, the final product may need touch-ups over time due to fading and progression of hair loss. Table 2 synthesizes and compares the surgical options for hair loss.
Table 2.
Advantages and disadvantages of surgical treatments for hair loss
| Micropigmentation | Hair Transplantation |
|---|---|
| Advantages: • Relatively permanent results • Visually resembles pores on a balding scalp • Can be used to disguise scalp scars after transplantation surgery |
Advantages: • Effective and permanent solution • Local anesthesia used for transplant • Hair used in transplant belongs to the same individual, resulting in more natural results |
| Disadvantages: • Risk of infection from procedure • Risk of allergy to pigment • Natural hair must be dyed to match pigment • May need touch-ups over time |
Disadvantages: • Risk of scalp swelling, bleeding, and minor infections • Risk of unnatural looking hair • Creation of donor scar • Expensive |
Conclusion
Hair is significant on multiple levels, including psychological, physical, social, and spiritual. Therefore, hair loss can have a substantial negative impact on an individual. Fortunately, a wide variety of hair loss concealment options exist for this common issue. Hair complements such as wigs, hair pieces, and extensions can be used to create the appearance of thicker, healthier hair. Pigmented concealing powders, lotions, and sprays can be used to affordably camouflage thinning hair. Surgical options such as micropigmentation and hair transplantation can be successful in individuals who are willing to commit to more permanent results. Each option carries its own advantages and disadvantages. The patient and treating physician must make an informed and intelligent decision together regarding which option(s) may be best for the patient.
Footnotes
This article is a reprint of a previously published article. For citation purposes, please use the original publication details; International Journal of Women's Dermatology 2 (2016) 122-127. DOI of original item: 10.1016/j.ijwd.2016.09.002.
References
- Aghaei S., Saki N., Daneshmand E., Kardeh B. Prevalence of psychological disorders in patients with alopecia areata in comparison with normal subjects. ISRN Dermatol. 2014;304370 doi: 10.1155/2014/304370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Banka N., Bunagan M.J., Dubrule Y., Shapiro J. Wigs and hairpieces: Evaluating dermatologic issues. Dermatol Ther. 2012;25(3):260–266. doi: 10.1111/j.1529-8019.2012.01506.x. [DOI] [PubMed] [Google Scholar]
- Baxley K.O., Erdman L.K., Henry E.B., Roof B.J. Alopecia: Effect on cancer patients’ body image. Cancer Nurs. 1984;7(6):499–503. [PubMed] [Google Scholar]
- Bernstein R.M., Rassman W.R. Follicular transplantation. Patient evaluation and surgical planning. Dermatol Surg. 1997;23(9):771–784. [PubMed] [Google Scholar]
- de Boer-Dennert M., de Wit R., Schmitz P.I., Djontono J., Beurden V., Stoter G. Patient perceptions of the side-effects of chemotherapy: the influence of 5HT3 antagonists. Br J Cancer. 1997;76(8):1055–1061. doi: 10.1038/bjc.1997.507. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Donovan J.C., Shapiro R.L., Shapiro P., Zupan M., Pierre-Louis M., Hordinsky M. A review of scalp camouflaging agents and prostheses for individuals with hair loss. Dermatol Online J. 2012;18(8):1. [PubMed] [Google Scholar]
- Hesketh P.J., Batchelor D., Golant M., Lyman G.H., Rhodes N., Yardley D. Chemotherapy-induced alopecia: Psychosocial impact and therapeutic approaches. Support Care Cancer. 2004;12(8):543–549. doi: 10.1007/s00520-003-0562-5. [DOI] [PubMed] [Google Scholar]
- Monselise A., Bar-On R., Chan L., Leibushor N., McElwee K., Shapiro J. Examining the relationship between alopecia areata, androgenetic alopecia, and emotional intelligence. J Cutan Med Surg. 2013;17(1):46–51. doi: 10.2310/7750.2012.12003. [DOI] [PubMed] [Google Scholar]
- Münstedt K., Manthey N., Sachsse S., Vahrson H. Changes in self-concept and body image during alopecia induced cancer chemotherapy. Support Care Cancer. 1997;5(2):139–143. doi: 10.1007/BF01262572. [DOI] [PubMed] [Google Scholar]
- Park J.H., Moh J.S., Lee S.Y., You S.H. Micropigmentation: Camouflaging scalp alopecia and scars in Korean patients. Aesthetic Plast Surg. 2014;38(1):199–204. doi: 10.1007/s00266-013-0259-1. [DOI] [PubMed] [Google Scholar]
- Rassman W.R., Pak J.P., Kim J., Estrin N.F. Scalp micropigmentation: A concealer for hair and scalp deformities. J Clin Aesthet Dermatol. 2015;8(3):35–42. [PMC free article] [PubMed] [Google Scholar]
- Shi Q., Duvic M., Osei J.S., Hordinsky M.K., Norris D.A., Price V.H. Health-related quality of life (HRQoL) in alopecia areata patients—A secondary analysis of the National Alopecia Areata Registry Data. J Investig Dermatol Symp Proc. 2013;16(1):S49–S50. doi: 10.1038/jidsymp.2013.18. [DOI] [PubMed] [Google Scholar]
- Shin J.W., Kwon S.H., Kim S.A., Kim J.Y., Na J.I., Park K.C. Characteristics of robotically harvested hair follicles in Koreans. J Am Acad Dermatol. 2015;72(1):146–150. doi: 10.1016/j.jaad.2014.07.058. [DOI] [PubMed] [Google Scholar]
- Sornakumar L., Shanmugasekar C., Rai R., Priya S. Allergic contact dermatitis to superglue. Int J Trichology. 2013;5(1):43–44. doi: 10.4103/0974-7753.114712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tischer B. Abstract presented at: American Academy of Dermatology Meeting. March 2000; San Francisco, CA. 2000. Influence of hair loss on employment decisions. [Google Scholar]
- Torchia D., Giogini S., Gola M., Francalanci S. Allergic contact dermatitis from 2ethylhexyl acrylate contained in a wigfixing adhesive tape and its 'incidental' therapeutic effect on alopecia areata. Contact Dermatitis. 2008;58(3):170–171. doi: 10.1111/j.1600-0536.2007.01212.x. [DOI] [PubMed] [Google Scholar]
- Traquina A.C. Micropigmentation as an adjuvant in cosmetic surgery of the scalp. Dermatol Surg. 2001;27(2):123–128. [PubMed] [Google Scholar]
- van der Velden E.M., Drost B.H., Ijsselmuiden O.E., Baruchin A.M., Hulsebosch H.J. Dermatography as a new treatment for alopecia areata of the eyebrows. Int J Dermatol. 1998;37(8):617–621. doi: 10.1046/j.1365-4362.1998.00540.x. [DOI] [PubMed] [Google Scholar]
- Weitz R. Farrar, Straus and Giroux; New York: 2004. Rapunzel’s daughters: What women’s hair tells us about women’s lives. [Google Scholar]
- Yang A., Iorizzo M., Vincenzi C., Tosti A. Hair extensions: A concerning cause of hair disorders. Br J Dermatol. 2009;160(1):207–209. doi: 10.1111/j.1365-2133.2008.08924.x. [DOI] [PubMed] [Google Scholar]