

Abstract
Isolated posterior cruciate ligament (PCL) tears are much less frequent than anterior cruciate ligament (ACL) tears.
Abrupt posterior tibial translation (such as dashboard impact), falls in hyperflexion and direct hyperextension trauma are the most frequent mechanisms of production.
The anterolateral bundle represents two-thirds of PCL mass and is reconstructed in single-bundle techniques.
The PCL has an intrinsic capability for healing. This is the reason why, nowadays, the majority of isolated PCL tears are managed non-operatively, with rehabilitation and bracing.
Recent studies have focused on double-bundle reconstruction techniques, as they seem to restore knee kinematics.
No significant clinical differences have been established between single versus double-bundle techniques, autograft versus allograft, transtibial tunnel versus tibial inlay techniques or remnant-preserving versus remnant-release techniques.
Cite this article: EFORT Open Rev 2017;2:89-96. DOI: 10.1302/2058-5241.2.160009
Keywords: PCL, ligament reconstruction, current management, posterior cruciate ligament
Introduction
Posterior cruciate ligament (PCL) tears are not as frequent as anterior cruciate ligament (ACL) tears. They are rare as an isolated injury and more commonly occur in a multi-ligament-injured knee.1
Although it is well-known that many patients may tolerate a PCL-deficient knee, it is also well-known that this situation can lead to altered loads and kinematics during activities of daily life.
Many conservative and surgical options have been proposed, but no consensus has been established, as the optimal PCL reconstruction has not been developed yet. The knowledge about PCL anatomy, epidemiology, biomechanics, clinical diagnosis and treatment management has evolved dramatically in recent years.2 These advances have achieved excellent clinical and functional outcomes after PCL reconstruction and could lead to better decision-making in future PCL tear management.
Epidemiology
There are about 200 000 ACL injuries per year in the United States, whereas only 3% of the injured knees have a PCL disruption.3 PCL injuries rarely occur in isolation, being typically associated with other ligament injuries such as ACL, medial collateral ligament (MCL) or posterolateral corner (PLC) injury.4,5 Specifically, most grade III PCL injuries present concurrently with other ligament injuries (79% of cases).5 These associated injuries are of the ACL in 46%, the MCL in 31% and the PLC in 62%.6
PCL injuries are commonly produced as a result of high-energy trauma, such as sport and motor vehicle accidents (57% of cases). The dashboard impact with abrupt posterior relative upper tibial translation is the most common mechanism in vehicle accidents. A fall in hyperflexion is a common cause of injury in athletes, especially affecting the anterolateral bundle. Another common mechanism is an abrupt impact with hyperextension of the knee.6 Other mechanisms of production include knee dislocation or rotation combined with varus/valgus forces.7 These injuries are more common in males, isolated or combined with other injuries, with significantly higher incidences (97%) compared with females (73%).6
Relevant anatomy and biomechanics
The PCL complex is composed of the anterolateral (ALB) and posteromedial (PMB) bundles and the meniscofemoral ligaments (Fig. 1).8 They can be well-differentiated at their femoral insertion, but they are very compact and difficult to separate at their tibial origin (Fig. 2).9
Fig. 1.
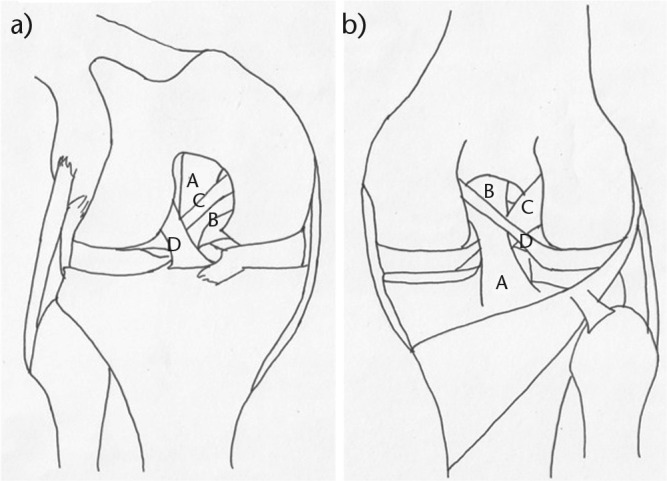
General ligament anatomy of a right knee. a) Anterior view. A, Anterolateral bundle of posterior cruciate ligament (PCL); B, posteromedial bundle (PMB) of PCL; C, anterior meniscofemoral ligament; D, anterior cruciate ligament. b) Posterior view. A, PMB; B, ALB; C, ACL; D, posterior meniscofemoral ligament.
Fig. 2.
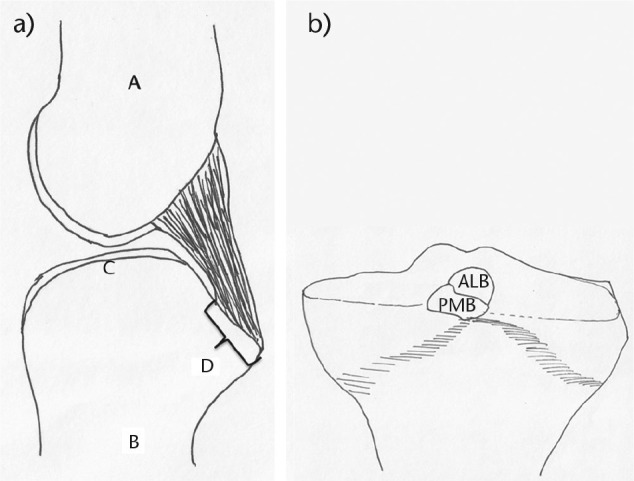
The two bundles of the posterior cruciate ligament (PCL) are very compact and difficult to separate at their tibial origin. a) Sagittal view of the tibial origin of the PCL. A, femur; B, tibia; C, tibial articular surface; D, origin of PCL. b) Coronal view of the posterior aspect of the proximal tibia showing the origin of the anterolateral bundle (ALB) and posteromedial bundle (PMB).
The PCL is an intra-articular extrasynovial ligament. The synovial membrane covers the entire ligament except the posterior part. The blood supply comes from the middle geniculate artery. Branches of the tibial nerve innervate the complex.
Classically, it was thought that each bundle dominated over the other one at different points in the range of movement (ROM). Recent studies have demonstrated that a co-dominant relationship exists between bundles in all ROMs.10 It has been noted that the PCL is the main restrictor of posterior tibial translation in all ROMs providing a significant restraint of internal rotation with a knee flexion of 90° or more.
The anterolateral bundle (ALB)
The femoral attachment of the ALB is nearly twice as big as the tibial insertion. The distance between the two attachments is 12.1 mm.9 The femoral attachment is 7.4 mm from the trochlear point, 11.0 mm from the medial arch point and 7.9 mm from the distal articular cartilage.9 The centre of the ALB tibial attachment site is 6.1 mm from posteromedial meniscus root.9 The ALB is more lax in full extension and tight in full flexion. As this bundle comprises about 65% of the total mass of the PCL, the classical techniques of single-bundle reconstruction try to substitute for it.
The posteromedial bundle (PMB)
The femoral attachment of the PMB is 11.1 mm from the medial arch point and 10.8 mm from the posterior point of the articular cartilage margin.9 The PMB is taught in extension and lax in flexion. Double-bundle techniques attempt to restore this bundle’s function.
The menisco-femoral ligaments
The PCL is surrounded by the anterior meniscofemoral ligament (Humphrey ligament) and the posterior meniscofemoral ligament (Wrisberg ligament), which emerge from the lateral aspect of the medial femoral condyle and insert distally close to the posterior horn of the lateral meniscus. Both ligaments are only present in 49% of the knees, providing up to 71% of the posterior stability in a PCL-deficient knee, particularly between 60° and 90° of flexion.11
Bony anatomy
Several bone references related to the tibial insertion and the intercondylar notch have been highlighted recently.9 The intercondylar notch apex is used for the point at the top of the notch. The ALB femoral insertion extends from the trochlear point to the medial arch point. The cartilage between these points is the so-called ‘arch of the cartilage’. The so-called ‘straight cartilage’ extends distally to the medial arch point on the lateral aspect of the medial femoral condyle.
Diagnosis of PCL injuries
It is paramount to elucidate whether the PCL tear is isolated or combined with other injuries because it determines long-term results of the treatment. Patient history, physical examination and correct imaging techniques are useful to achieve a correct diagnosis.
Patient history
The patient with a PCL tear frequently complains of symptoms such as instability or discomfort. Mild to moderate effusion and pain in the posterior aspect of the knee or with kneeling are also frequent in the acute stage. Symptoms from chronic injuries are usually related to deceleration movements, such as descending inclines or stairs.12
Physical examination
The majority of physical examination manoeuvres attempt to demonstrate a posterior instability and subluxation of the knee. The most frequently used are the posterior sag sign, the Godfrey’s test, the quadriceps active test and posterior drawer test (Fig. 3a).13 No complete evidence for diagnosis of a PCL tear has been demonstrated with any of these tests.14
Fig. 3.
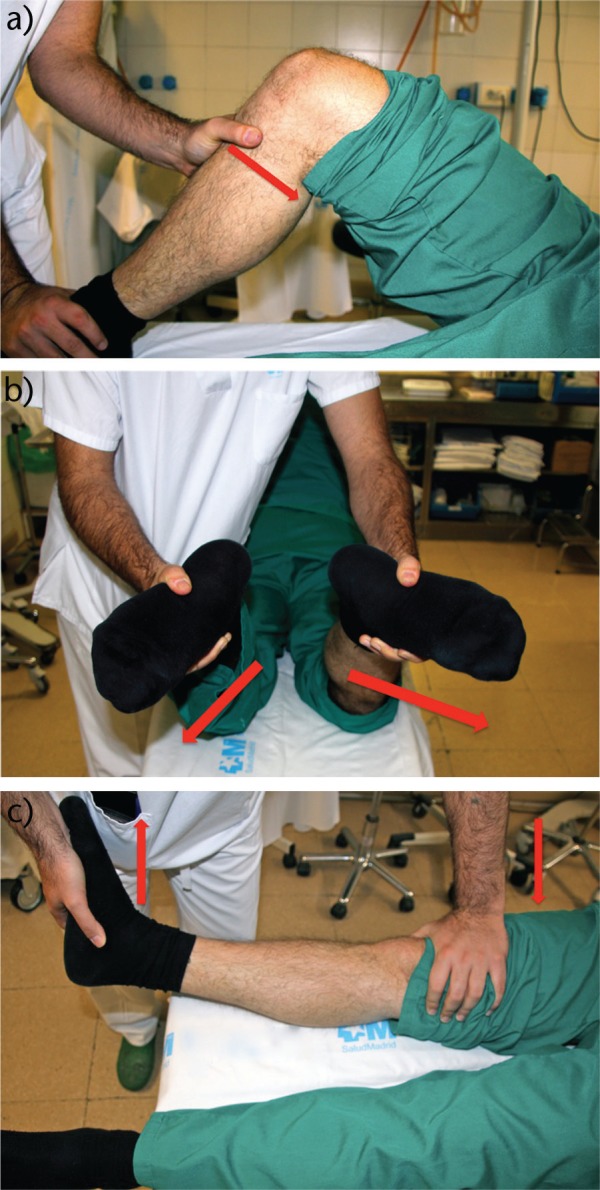
Most frequently used tests to demonstrate a posterior cruciate ligament (PCL) injury. a) Posterior ‘drawer’ test. The knee is flexed at 90°, the hip is flexed at 45°, the foot is stabilised and the tibia is in neutral position. A posterior direction force is applied to the proximal tibia. Posterior subluxation of the tibia is assessed by measuring of the displacement of the medial tibial plateau related to the medial femoral condyle. b) ‘Dial’ test. An increase of external rotation (> 10°) with the knee at 90° and 30° of flexion is suggestive of a PCL and posterolateral corner (PLC) injury. If the increase is only at 30° but not at 90°, the PCL is intact but a PLC injury exists. c) External rotation-recurvatum test. This test is positive if the knee acquires hyperextension, varus angulation and external rotation of the tibia compared with the contralateral side.
As PCL tears are usually present with other concomitant injuries, mainly affecting MCL and PLC, varus and valgus stress tests, in full extension and 30° of flexion, are useful for examining the integrity of MCL and LCL. Posterolateral and anteromedial ‘drawer’ test and ‘dial’ tests (Fig. 3b) are especially useful in the diagnosis of a concomitant posterolateral or posteromedial corner injury. The external rotation-recurvatum test (Fig. 3c) and reverse pivot-shift test may indicate an associated PLC tear.7 Walking with a varus deviation of the knee has to make us consider a concomitant PLC injury.
Imaging studies
Multiple imaging studies can be used as adjuvant to physical examination for PCL diagnosis: plain radiographs, examination under fluoroscopy, MRI, etc.
Plain radiographs and fluoroscopy
Standard radiographic studies should include anteroposterior, lateral, ‘sunrise’ and tunnel views.15 We should address any sign of bone fracture or avulsion (PCL tibial insertion, Segond fracture, widening of the lateral joint space, avulsion of the fibula head, etc.) and any degree of posterior tibial sag or knee subluxation must be checked.13 Intra-operative fluoroscopy examination is crucial, because the tibial attachment of the PCL is not easy to visualise with arthroscopy. A recent study has accurately defined the tibial attachment of the PCL.16
Stress radiographs are objective tests to demonstrate posterior tibial subluxation. Many devices (i.e. Telos)17 and manoeuvres (i.e. hamstring contraction with the knee flexed 90°) have been proposed,12,18 with no significant differences in usefulness. However, the single-leg kneeling technique is a cheap, reliable, fast and useful technique to address a posterior tibial instability.
Posterior translation of the tibia has been measured, which identifies isolated PCL partial tears where there is < 8 mm of translation, complete PCL tears, where there is between 8 mm and 12 mm, and associated PLC injury when the posterior tibial translation is > 12 mm.19
MRI
The use of MRI techniques has been demonstrated to be highly accurate for diagnosing acute PCL tears. High sensitivity (near 100%) and specificity (near 97%) have been reported.20 The normal PCL has a curved appearance, with uniform low signal intensity on all pulse sequences.3 The PCL can be torn at its tibial or femoral attachments or more commonly through its substance. There are some characteristics of a PCL tear on MRI, such as: increased signal intensity with disruption of the ligament; abnormal thickening of PCL with anteroposterior diameter greater than 7 mm; and intra-substance fluid signal on T2 or a striated appearance in the case of a partial tear. The ‘double PCL’ sign usually correlates with a bucket handle tear of the medial meniscus with an intact PCL.7
As the PCL trends to healing without repair or reconstruction, it is a vital point to distinguish a chronic injury, particularly when MRI is done after six months from the injury. It has been shown that 28% of chronic PCL injuries show a near-normal MRI appearance.21 Residual morphological deformity, but with continuous ligament was seen in 44%. In these cases, stress radiographs may provide accurate information for diagnosis of instability.
Lateral bone bruising on radiographs is common when concomitant PCL-MCL occurs. Medial bone bruising makes us consider a combined PCL-PLC injury.22 Meniscal and concomitant ACL injuries can also be addressed with MRI.
Treatment
Indications for operative management
The main questions in PCL tear treatment are to elucidate whether it is an acute or chronic lesion and an isolated or combined injury. An isolated PCL injury is usually managed non-operatively.
Acute PCL tears, with posterior tibial translation between 8 mm and 12 mm, are usually due to an isolated ligament injury. These injuries are usually managed non-operatively. A concomitant repairable meniscal injury could therefore be an indication for surgical treatment of both lesions.
Acute PCL tears, with knee dislocation or posterior tibial translation ⩾ 12 mm, have to make us consider a combined injury, which is managed surgically.
Chronic PCL tears are treated only in cases of the presence of PCL-related symptoms (problems with deceleration, incline descending, etc.) and posterior tibial translation > 8 mm,23,24 or if a combined injury exists.
Non-operative treatment
It is well known that the PCL has an intrinsic ability to heal. However, it has been noted that this healing usually occurs in a lax position.25,26 On the other hand, isolated injuries have been well managed with bracing as a non-operative treatment.27-29 The majority of athletes suffering an isolated PCL tear return to activity with rehabilitation, achieving knee stability by enhancing muscles to compensate posterior tibial translation.15 PCL bracing aims to compensate the tibial sag, applying an anterior counterforce, in an effort to achieve PCL healing in better position.24
The knee is usually immobilised between two and four weeks in full extension. After that, a programme encouraging strengthening of quadriceps muscle is performed. Hamstrings use is prohibited to avoid posterior tibial translation. The athletes are normally allowed to return to sport when the knee is completely stabilised and the quadriceps force is 90% of the contralateral knee, which is often not before three months from the injury, depending on the sport.7
Conflicting objective and subjective results have been reported in the literature.29,30 Although most case series show good subjective outcomes, a significant percentage of moderate to severe cases of osteoarthritis have been noted, directly related to the length of time of follow-up.27 Dynamic braces have been shown to achieve good healing rates and compensate tibial sag in the short to medium term.25
Operative treatment
Most of the techniques developed for PCL tear treatment are arthroscopically performed. Single- or double-bundle reconstruction using autograft or allograft and different methods of fixation have been proposed.
Single-bundle reconstruction
Single-bundle reconstruction techniques have been performed classically for PCL reconstruction. Some clinical differences have been seen between ‘isometric point’ techniques and ‘anatomical’ techniques.30,31 As the first option has been related to over-constraint of the joint in the post-operative period and a trend to laxity with time, the anatomical techniques, using radiographic and arthroscopic references, are most favoured.
Moreover, many studies have been focused on tibial graft fixation. Two main types of fixation have been investigated: the transtibial tunnel and the tibial-inlay techniques.27
The transtibial tunnel technique (Fig. 4a) aims to simulate the tibial and femoral ALB origins. The main concern in this technique is the so-called ‘killer turn’, the sharp angle on the tibial tunnel exit that may produce abrasion, attenuation and subsequent graft failure.32,33 The tibial-inlay techniques (Fig. 4b) try to avoid this situation with a bone plug in the extremity of the graft, securing bone-to-bone tibial attachment with an anchor or screw. Classically, these techniques were performed by a posteromedial approach between semi-tendinosus and medial gastrocnemius for securing the tibial attachment, but several all-arthroscopic options have been proposed recently.34 Bone-patellar tendon-bone (BTB) autograft or Achilles tendon allograft are usually used for this reconstruction. Even if some studies reported better results with tibial-inlay techniques,34 this topic remains controversial and no sufficient evidence exists supporting this affirmation13 as there is no in vivo evidence of increased graft failure rate for trans-tibial tunnel techniques.35 Knee stability is improved with both techniques either in isolated or combined PCL tears, but it is not completely restored to normality independently of the single-bundle technique used.
Fig. 4.
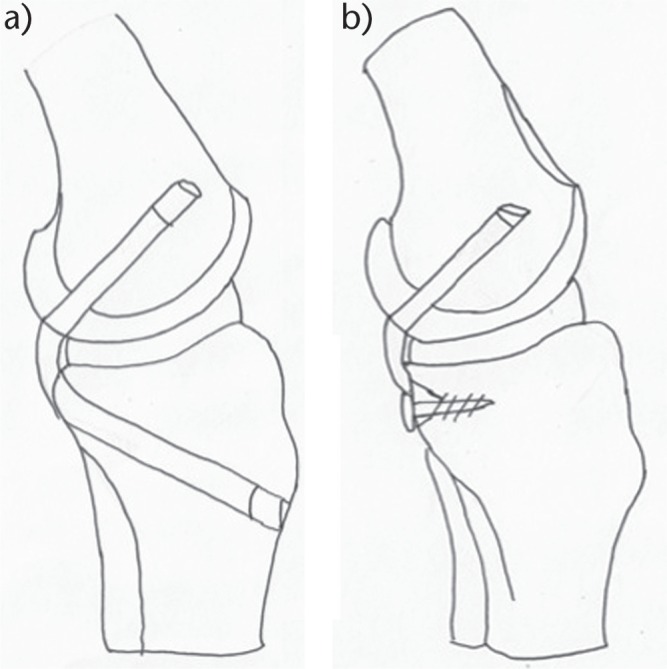
The two main surgical techniques for reconstruction of the posterior cruciate ligament (PCL). a) Trans-tibial tunnel technique. b) Tibial inlay technique.
Regarding the graft type, most reconstructions are performed with autograft, usually BTB or hamstrings, especially in isolated PCL reconstructions.1 Achilles tendon is the most-used option for the allograft group.1 In biomechanical studies, quadruple-strand hamstrings have demonstrated more resistance to loading failure, as the BTB is more resistant to elongation.36 No differences in clinical results regarding failure rate have been demonstrated between allografts and autografts, but surgical time, donor site complications and infections are more frequent with autograft.37
Remnant-preserving of femoral and tibial attachments of the native ligament has been advocated as a way to improve healing and function of the reconstruction. Theoretical benefit of improved blood supply and innervation is claimed by those surgeons who do not make a full release of the PCL attachments. However, no differences have been demonstrated between remnant-preserving and conventional techniques.38
Double-bundle reconstruction
Double-bundle reconstruction techniques have been developed as an alternative to single-bundle techniques. The theoretical benefit is to restore the normal kinematics of the knee, as both ALB and PMB work in a combined relationship not emulated by a single-bundle reconstruction (which could only restore normal kinematics between the first 0° to 60° of flexion).10
This technique requires two femoral tunnels (one bigger for the ALB and one smaller for the PMB) but just one tibial tunnel is usually needed.39 Tibial inlay techniques have also been developed for double-bundle reconstruction.34 Among these techniques, an allograft (i.e. Achilles tendon, quadriceps tendon or BTB allograft) is usually attached to the tibial origin with a bone plug and the tendon is split in two, simulating the two PCL bundles. Autografts (BTB for ALB reconstruction and hamstrings for PMB reconstruction) have also been used for double-bundle reconstruction.40
No differences between tibial inlay and trans-tibial double-bundle techniques have been reported in the literature.13 Both techniques have good clinical outcomes, especially in posterior tibial translation and subjective function, either with isolated or combined injuries as well as in primary or revision surgery.13 Tibial inlay techniques have been proposed as a good alternative for revision surgeries.41
Comparison between single-bundle and double-bundle reconstructions
There are no level I studies in the literature comparing single-bundle and double-bundle reconstructions. Nevertheless, a recent well-designed study42 has demonstrated slight differences in objectives outcomes (posterior tibial translation, Lysholm score), with double-bundle reconstructions being more accurate than single-bundle reconstructions in restoring the knee to native stability levels.
Rehabilitation
It is well-known that PCL graft healing usually takes about double the time of an ACL healing. This is why PCL rehabilitation is the keystone of a successful recovery. Several principles have been established: progressive weight-bearing; avoiding posterior tibial subluxation; avoiding hamstring action; and improving quadriceps force.43
The knee is immobilised for three to six weeks in full extension, and after that progressive passive flexion range is allowed. The brace should be worn all the time for at least two to four months. Dynamic braces, applying an anterior drawer force depending on flexion degree, can be useful during the rehabilitation programme.25,44 Return to sport is not usually allowed before six to nine months after reconstruction.
Complications
The most frequent complications in PCL injuries are related to ROM.45 Residual laxity (posterior tibial translation > 4 mm) can be a manifestation of undiagnosed concomitant soft-tissue injury (i.e. PLC). Flexion loss is more frequent after prolonged immobilisation in extension after the surgery and can be managed with mobilisation under anaesthesia. Excessively tensioned or malpositioned graft can also lead to limited movement.7 Meniscal roots or popliteal artery injuries have been described in transtibial tunnel techniques.45 In tibial inlay techniques, saphenous nerve and popliteal artery injuries are related to the approach used and a risk of bone plug nonunion exists.45
Conclusions
Table 1 summarises current recommended treatment (conservative versus reconstruction) for isolated PCL injuries depending on the grade of injury (I to III) and the time of injury (acute versus chronic). Table 2 shows current recommended reconstruction techniques and types of graft for isolated PCL injuries.
Table 1.
Recommended treatment for isolated posterior cruciate ligament (PCL) injuries
| Grade of injury | Recommended treatment |
|---|---|
| Acute injury | |
| Grade I and II injuries (< 10 mm posterior laxity) | Conservative treatment |
| Grade III injuries (> 10 mm posterior laxity) | PCL injury may be treated conservatively but if instability persists, reconstruction should be performed |
| Chronic injury | |
| Grade I and II injuries | Conservative treatment |
| Grade III injuries | PCL injury should be reconstructed if pain and instability persists after conservative treatment |
Table 2.
Recommended reconstruction techniques and type of graft for isolated posterior cruciate ligament (PCL) injuries
| Optimal reconstruction technique |
|---|
| Reconstruction must be performed arthroscopically using single- or double-bundle techniques with inlay or inlay/transtibial technique Reported fixation methods are numerous and none has shown superiority |
| Type of graft |
| Reliable results have been found with a variety of auto- and allograft choices including: bone-patellar tendon-bone autograft; hamstring tendons; quadriceps tendon; and Achilles tendon. None has shown superiority Allografts: shorter duration of surgery, no donor site morbidity. Tissue quality can be a problem |
Acknowledgments
We thank Dr. Joaquín Núñez-De Armas and Dr Rafael Carbonell Escobar for their collaboration with the figures.
Footnotes
ICMJE Conflict of interest statement: None.
Funding statement
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
References
- 1. Kim YM, Lee CA, Matava MJ. Clinical results of arthroscopic single-bundle transtibial posterior cruciate ligament reconstruction: a systematic review. Am J Sports Med 2011;39:425-434. [DOI] [PubMed] [Google Scholar]
- 2. Levy BA, Fanelli GC, Miller MD, Stuart MJ. Advances in posterior cruciate ligament reconstruction. Instr Course Lect 2015;64:543-554. [PubMed] [Google Scholar]
- 3. Naraghi A, White LM. MR imaging of cruciate ligaments. Magn Reson Imaging Clin N Am 2014;22:557-580. [DOI] [PubMed] [Google Scholar]
- 4. Morelli V, Bright C, Fields A. Ligamentous injuries of the knee: anterior cruciate, medial collateral, posterior cruciate, and posterolateral corner injuries. Prim Care 2013;40:335-356. [DOI] [PubMed] [Google Scholar]
- 5. Becker EH, Watson JD, Dreese JC. Investigation of multiligamentous knee injury patterns with associated injuries presenting at a level I trauma center. J Orthop Trauma 2013;27:226-231. [DOI] [PubMed] [Google Scholar]
- 6. Fanelli GC, Edson CJ. Posterior cruciate ligament injuries in trauma patients: part II. Arthroscopy 1995;11:526-529. [DOI] [PubMed] [Google Scholar]
- 7. Rosenthal MD, Rainey CE, Tognoni A, Worms R. Evaluation and management of posterior cruciate ligament injuries. Phys Ther Sport 2012;13:196-208. [DOI] [PubMed] [Google Scholar]
- 8. Narvy SJ, Pearl M, Vrla M, Yi A, Hatch GFR., III Anatomy of the femoral footprint of the posterior cruciate ligament: a systematic review. Arthroscopy 2015;31:345-354. [DOI] [PubMed] [Google Scholar]
- 9. Anderson CJ, Ziegler CG, Wijdicks CA, Engebretsen L, LaPrade RF. Arthroscopically pertinent anatomy of the anterolateral and posteromedial bundles of the posterior cruciate ligament. J Bone Joint Surg [Am] 2012;94-A:1936-1945. [DOI] [PubMed] [Google Scholar]
- 10. Kennedy NI, Wijdicks CA, Goldsmith MT, et al. Kinematic analysis of the posterior cruciate ligament, part 1: the individual and collective function of the anterolateral and posteromedial bundles. Am J Sports Med 2013;41:2828-2838. [DOI] [PubMed] [Google Scholar]
- 11. Gupte CM, Bull AMJ, Thomas RD, Amis AA. The meniscofemoral ligaments: secondary restraints to the posterior drawer. Analysis of anteroposterior and rotary laxity in the intact and posterior-cruciate-deficient knee. J Bone Joint Surg [Br] 2003;85-B:765-773. [PubMed] [Google Scholar]
- 12. Margheritini F, Mariani PP. Diagnostic evaluation of posterior cruciate ligament injuries. Knee Surg Sports Traumatol Arthrosc 2003;11:282-288. [DOI] [PubMed] [Google Scholar]
- 13. LaPrade CM, Civitarese DM, Rasmussen MT, LaPrade RF. Emerging updates on the posterior cruciate ligament: A review of the current literature. Am J Sports Med 2015;43:3077-3092. [DOI] [PubMed] [Google Scholar]
- 14. Kopkow C, Freiberg A, Kirschner S, Seidler A, Schmitt J. Physical examination tests for the diagnosis of posterior cruciate ligament rupture: a systematic review. J Orthop Sports Phys Ther 2013;43:804-813. [DOI] [PubMed] [Google Scholar]
- 15. Colvin AC, Meislin RJ. Posterior cruciate ligament injuries in the athlete: diagnosis and treatment. Bull NYU Hosp Jt Dis 2009;67:45-51. [PubMed] [Google Scholar]
- 16. Johannsen AM, Anderson CJ, Wijdicks CA, Engebretsen L, LaPrade RF. Radiographic landmarks for tunnel positioning in posterior cruciate ligament reconstructions. Am J Sports Med 2013;41:35-42. [DOI] [PubMed] [Google Scholar]
- 17. Jackman T, LaPrade RF, Pontinen T, Lender PA. Intraobserver and interobserver reliability of the kneeling technique of stress radiography for the evaluation of posterior knee laxity. Am J Sports Med 2008;36:1571-1576. [DOI] [PubMed] [Google Scholar]
- 18. Jung TM, Reinhardt C, Scheffler SU, Weiler A. Stress radiography to measure posterior cruciate ligament insufficiency: a comparison of five different techniques. Knee Surg Sports Traumatol Arthrosc 2006;14:1116-1121. [DOI] [PubMed] [Google Scholar]
- 19. Sekiya JK, Whiddon DR, Zehms CT, Miller MD. A clinically relevant assessment of posterior cruciate ligament and posterolateral corner injuries. Evaluation of isolated and combined deficiency. J Bone Joint Surg [Am] 2008;90-A:1621-1627. [DOI] [PubMed] [Google Scholar]
- 20. Laoruengthana A, Jarusriwanna A. Sensitivity and specificity of magnetic resonance imaging for knee injury and clinical application for the Naresuan University Hospital. J Med Assoc Thai 2012;95:S151-S157. [PubMed] [Google Scholar]
- 21. Jung YB, Jung HJ, Yang JJ, et al. Characterization of spontaneous healing of chronic posterior cruciate ligament injury: analysis of instability and magnetic resonance imaging. J Magn Reson Imaging 2008;27:1336-1340. [DOI] [PubMed] [Google Scholar]
- 22. Mair SD, Schlegel TF, Gill TJ, Hawkins RJ, Steadman JR. Incidence and location of bone bruises after acute posterior cruciate ligament injury. Am J Sports Med 2004;32:1681-1687. [DOI] [PubMed] [Google Scholar]
- 23. Montgomery SR, Johnson JS, McAllister DR, Petrigliano FA. Surgical management of PCL injuries: indications, techniques, and outcomes. Curr Rev Musculoskelet Med 2013;6:115-123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Jansson KS, Costello KE, O’Brien L, Wijdicks CA, Laprade RF. A historical perspective of PCL bracing. Knee Surg Sports Traumatol Arthrosc 2013;21:1064-1070. [DOI] [PubMed] [Google Scholar]
- 25. Jacobi M, Reischl N, Wahl P, Gautier E, Jakob RP. Acute isolated injury of the posterior cruciate ligament treated by a dynamic anterior drawer brace: a preliminary report. J Bone Joint Surg [Br] 2010;92-B:1381-1384. [DOI] [PubMed] [Google Scholar]
- 26. Chandrasekaran S, Ma D, Scarvell JM, Woods KR, Smith PN. A review of the anatomical, biomechanical and kinematic findings of posterior cruciate ligament injury with respect to non-operative management. Knee 2012;19:738-745. [DOI] [PubMed] [Google Scholar]
- 27. Shelbourne KD, Clark M, Gray T. Minimum 10-year follow-up of patients after an acute, isolated posterior cruciate ligament injury treated nonoperatively. Am J Sports Med 2013;41:1526-1533. [DOI] [PubMed] [Google Scholar]
- 28. Shelbourne KD, Davis TJ, Patel DV. The natural history of acute, isolated, nonoperatively treated posterior cruciate ligament injuries. A prospective study. Am J Sports Med 1999;27:276-283. [DOI] [PubMed] [Google Scholar]
- 29. Shelbourne KD, Muthukaruppan Y. Subjective results of nonoperatively treated, acute, isolated posterior cruciate ligament injuries. Arthroscopy 2005;21:457-461. [DOI] [PubMed] [Google Scholar]
- 30. Race A, Amis AA. PCL reconstruction. In vitro biomechanical comparison of ‘isometric’ versus single and double-bundled ‘anatomic’ grafts. J Bone Joint Surg [Br] 1998;80-B:173-179. [DOI] [PubMed] [Google Scholar]
- 31. Wijdicks CA, Kennedy NI, Goldsmith MT, et al. Kinematic analysis of the posterior cruciate ligament, part 2: a comparison of anatomic single- versus double-bundle reconstruction. Am J Sports Med 2013;41:2839-2848. [DOI] [PubMed] [Google Scholar]
- 32. Panchal HB, Sekiya JK. Open tibial inlay versus arthroscopic transtibial posterior cruciate ligament reconstructions. Arthroscopy 2011;27:1289-1295. [DOI] [PubMed] [Google Scholar]
- 33. Markolf KL, Zemanovic JR, McAllister DR. Cyclic loading of posterior cruciate ligament replacements fixed with tibial tunnel and tibial inlay methods. J Bone Joint Surg [Am] 2002;84-A:518-524. [DOI] [PubMed] [Google Scholar]
- 34. Kim SJ, Kim TE, Jo SB, Kung YP. Comparison of the clinical results of three posterior cruciate ligament reconstruction techniques. J Bone Joint Surg [Am] 2009;91-A:2543-2549. [DOI] [PubMed] [Google Scholar]
- 35. Hermans S, Corten K, Bellemans J. Long-term results of isolated anterolateral bundle reconstructions of the posterior cruciate ligament: a 6- to 12-year follow-up study. Am J Sports Med 2009;37:1499-1507. [DOI] [PubMed] [Google Scholar]
- 36. Chen CH, Chou SW, Chen WJ, Shih CH. Fixation strength of three different graft types used in posterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 2004;12:371-375. [DOI] [PubMed] [Google Scholar]
- 37. Wang CJ, Chan YS, Weng LH, Yuan LJ, Chen HS. Comparison of autogenous and allogenous posterior cruciate ligament reconstructions of the knee. Injury 2004;35:1279-1285. [DOI] [PubMed] [Google Scholar]
- 38. Del Buono A, Radmilovic J, Gargano G, Gatto S, Maffulli N. Augmentation or reconstruction of PCL? A quantitative review. Knee Surg Sports Traumatol Arthrosc 2013;21:1050-1063. [DOI] [PubMed] [Google Scholar]
- 39. Spiridonov SI, Slinkard NJ, LaPrade RF. Isolated and combined grade-III posterior cruciate ligament tears treated with double-bundle reconstruction with use of endoscopically placed femoral tunnels and grafts: operative technique and clinical outcomes. J Bone Joint Surg [Am] 2011;93-A:1773-1780. [DOI] [PubMed] [Google Scholar]
- 40. Garofalo R, Jolles BM, Moretti B, Siegrist O. Double-bundle transtibial posterior cruciate ligament reconstruction with a tendon-patellar bone-semitendinosus tendon autograft: clinical results with a minimum of 2 years’ follow-up. Arthroscopy 2006;22:1331-1338.e1. [DOI] [PubMed] [Google Scholar]
- 41. Lee SH, Jung YB, Lee HJ, Jung HJ, Kim SH. Revision posterior cruciate ligament reconstruction using a modified tibial-inlay double-bundle technique. J Bone Joint Surg [Am] 2012;94-A:516-522. [DOI] [PubMed] [Google Scholar]
- 42. Yoon KH, Bae DK, Song SJ, Cho HJ, Lee JH. A prospective randomized study comparing arthroscopic single-bundle and double-bundle posterior cruciate ligament reconstructions preserving remnant fibers. Am J Sports Med 2011;39:474-480. [DOI] [PubMed] [Google Scholar]
- 43. Pierce CM, O’Brien L, Griffin LW, Laprade RF. Posterior cruciate ligament tears: functional and postoperative rehabilitation. Knee Surg Sports Traumatol Arthrosc 2013;21:1071-1084. [DOI] [PubMed] [Google Scholar]
- 44. LaPrade RF, Smith SD, Wilson KJ, Wijdicks CA. Quantification of functional brace forces for posterior cruciate ligament injuries on the knee joint: an in vivo investigation. Knee Surg Sports Traumatol Arthrosc 2015;23:3070-3076. [DOI] [PubMed] [Google Scholar]
- 45. Zawodny SR, Miller MD. Complications of posterior cruciate ligament surgery. Sports Med Arthrosc 2010;18:269-274. [DOI] [PubMed] [Google Scholar]