

Abstract
An audit of thrombolytic therapy for acute myocardial infarction (AMI) in 1992–93 showed that door to needle time had a median delay of 100 min. After discussion, we devised a new 'fast track' procedure. General practitioners (GPs) were given minimum criteria for diagnosing probable AMI and advised how to admit patients directly to the coronary care unit (CCU) after discussion with a senior CCU nurse.
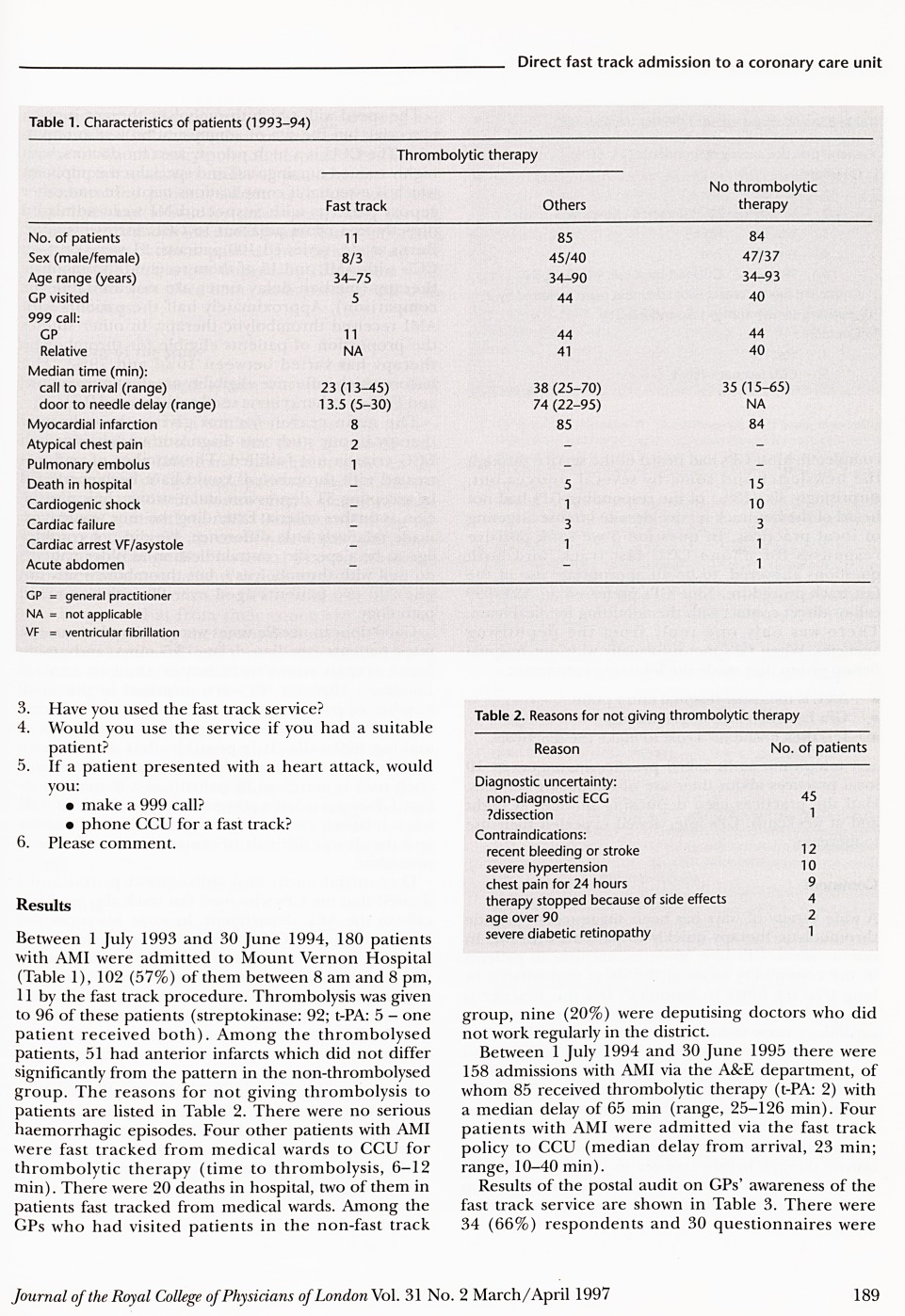
The hospital admitted 180 patients with MI between 1 July 1993 and 30 June 1994, 96 of whom received thrombolysis. Of the 11 admitted by the fast track procedure, eight received thrombolysis (median delay, 13.5 min; range, 5–30 min; p <0.05 when compared with non-fast track patients). Four other patients were fast tracked to the CCU from other medical wards (time to thrombolysis, 6–12 min). In the following year to 30 June 1995 there were 158 admissions with MI, of whom 85 (54%) received thrombolysis. Four patients were admitted by the fast track procedure.
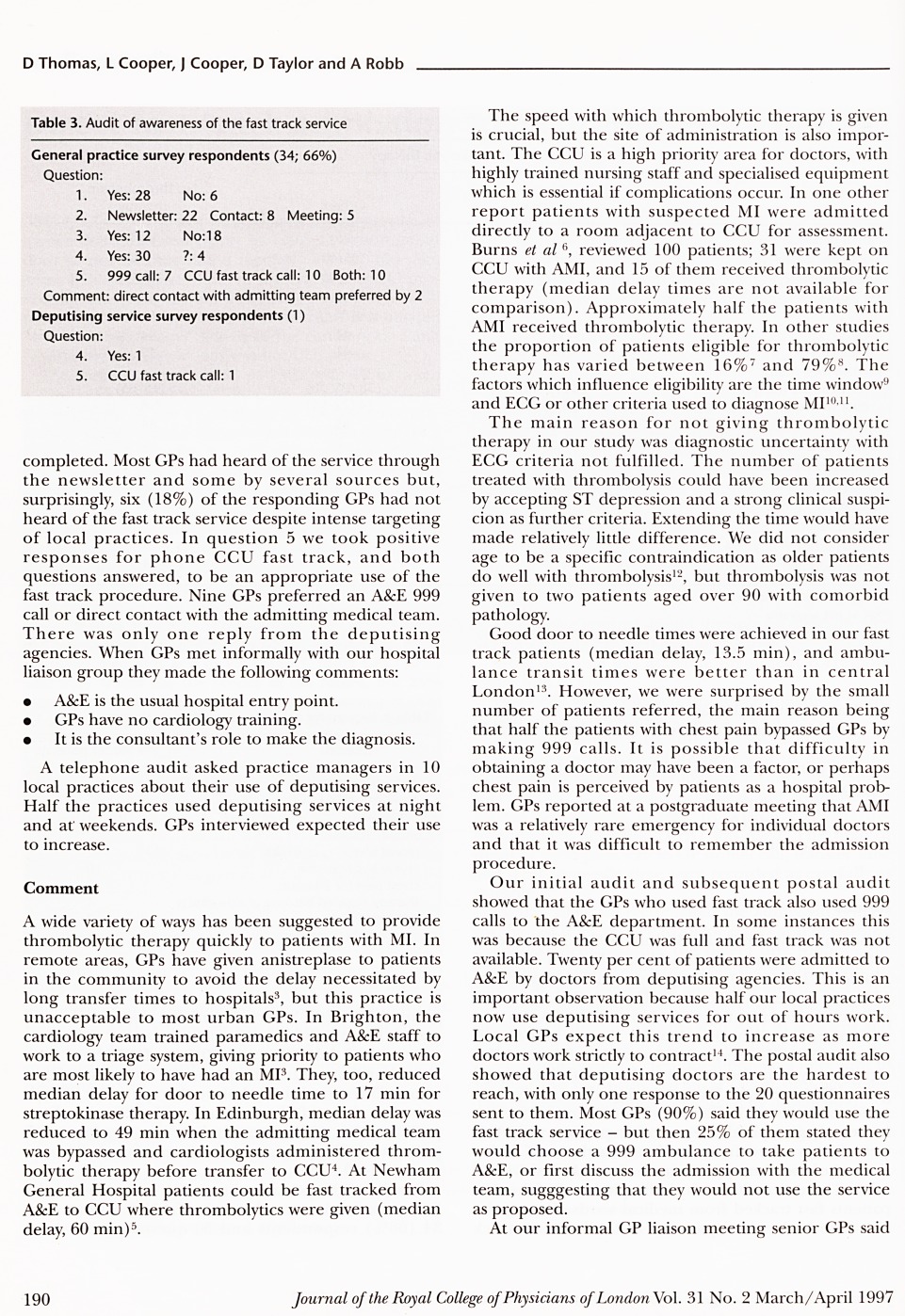
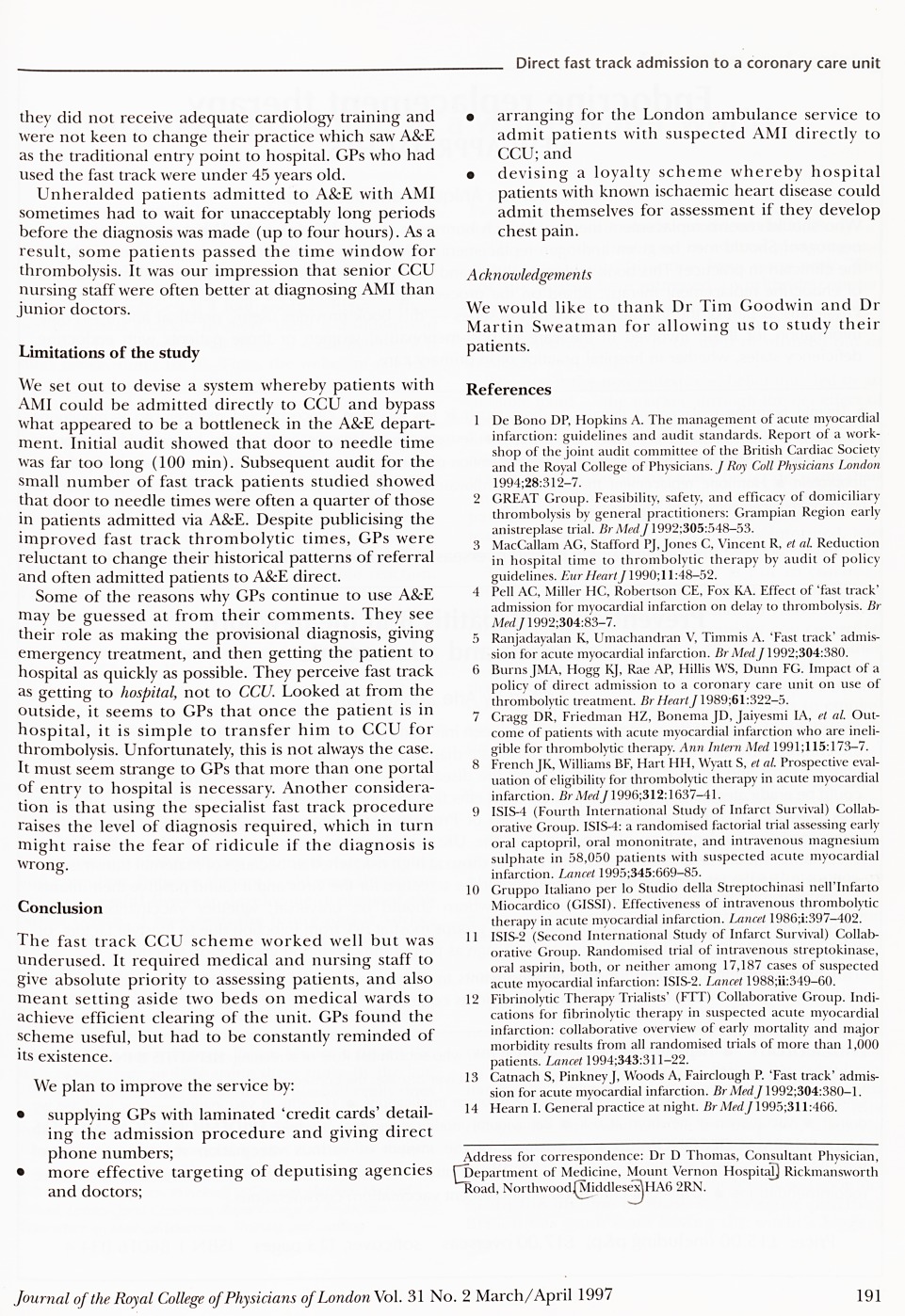
Although the fast track procedure shortened the time to thrombolysis, the service was underused. A postal audit of local practices showed that 18% of GPs were still unaware of the service, in spite of newsletters, post-graduate meetings and direct contact. Most GPs (90%) said they would use the service in the future, but 25% stated later that they would not use it. Twenty per cent of non-fast track AMI patients were admitted by deputising doctors.
Full text
PDF
Contributor Information
David Thomas, Consultant Physician, Mount Vernon Hospital, Northwood, Middlesex.
Leanne Cooper, Coronary Care Sister, Mount Vernon Hospital, Northwood, Middlesex.
Julie Cooper, Coronary Care Sister, Mount Vernon Hospital, Northwood, Middlesex.
Deborah Taylor, Coronary Care Sister, Mount Vernon Hospital, Northwood, Middlesex.
Alex Robb, Audit Facilitator, Mount Vernon Hospital, Northwood, Middlesex.