

Abstract
We sought to organize a functional system of recognition and advanced treatment of hypothermic patients with extracorporeal rewarming as a treatment option. All patients with suspected hypothermia are consulted with the hypothermia coordinator (HC), whose role is to provide expertise on hypothermia recognition and treatment to all rescue and medical services. Patients with Swiss staging system of hypothermia class III and IV are subjected to extracorporeal rewarming. Patients with class I and II are managed in local hospitals, after the HC provides instructions. From program initiation (July 29, 2013) to November 1, 2015, HC consulted 104 hypothermic patients; 21 in hypothermia class III and IV were subjected to extracorporeal rewarming in the John Paul II Hospital in Cracow, Poland. The remaining people were rewarmed in the referring hospitals. Cardiac arrest upon referral was present in 10 cases (resuscitation times from arrest to extracorporeal membrane oxygenation implantation ranged 107–345 minutes). Seven patients died, and the remaining 14 have been rewarmed with the restoration of hemodynamic stability. Systematic approach to active recognition and treatment of profound accidental hypothermia patients, on the basis of HC cooperation with emergency medical services, enables advanced management with good outcomes, especially in patients with cardiac arrest.
Keywords: hypothermia, extracorporeal membrane oxygenation, cardiopulmonary resuscitation, rewarming
Profound accidental hypothermia is one of the causes of refractory cardiogenic shock or cardiac arrest and, unless treated aggressively, may be fatal. The incidence of accidental hypothermia of any severity is difficult to assess worldwide, and all data are believed to be highly underestimated. Exposure to excessive natural cold had been recognized as a cause of death in 2,198 patients in Poland in years 2009–2013, out of which 624 (28.3%) died in hospital.1,2 These deaths were classified as deaths to be prevented.
As no special protocol or algorithm for hypothermia recognition and treatment had been implemented in Poland, Severe Hypothermia Treatment Center was established on July 29, 2013 in Cracow. To the best of our knowledge, it is the only such an initiative worldwide.3 What at first meant to be mainly a help in qualification for extracorporeal rewarming became a multidisciplinary project, and the aim is to organize a functional system of early recognition and advanced treatment of hypothermic patients, with extracorporeal rewarming being one of the therapeutic options for unstable or arrested patients. Any cardiac surgery center, having experienced staff and equipment for extracorporeal circulation at disposal, should be dedicated to manage patients with profound accidental hypothermia, who require extracorporeal rewarming.4
The purpose of this study is to present Severe Hypothermia Treatment Center experience in arranging a system of active recognition and treatment of hypothermic patients. Because the literature covering the topic of accidental hypothermia is mainly limited to case studies or case series,5 our approach seems to be novel and in our opinion may attribute to development of national or regional complex protocols of managing hypothermic patients.
Materials and Methods
To consult and manage as many hypothermic patients as possible, and preferably all, some arrangements have been made, which on the one hand are targeted on prehospital and inhospital emergency services, and all civil rescue services, and on the other hand cover all duties of the team of Severe Hypothermia Treatment Center. It should be pointed out that Severe Hypothermia Treatment Center constitutes a part of the Department of Cardiovascular Surgery and Transplantation of the John Paul II Hospital in Cracow, Poland, and uses both equipment and staff of this institution.
An on-call hypothermia coordinator (HC) has been designated, who serves with expert knowledge on hypothermia to all outhospital and inhospital emergency services, coordinates transfers of hypothermic patients, and collaborates with all civil rescue services. Their role is to assess all referred people with suspected or confirmed hypothermia, and depending on its severity, they either instruct referring team how to manage the patient with noninvasive or less-invasive means of rewarming or accept the patient for extracorporeal rewarming to Severe Hypothermia Treatment Center. The role of the coordinator is also to collaborate with local transport emergency service and helicopter emergency service to arrange safe transfer to the Center, also from remote, mountainous regions. Last but not least, the coordinator calls in the onsite team that implements extracorporeal membrane oxygenation (ECMO) and further manages the patient.
To be able to consult all hypothermic patients, a massive campaign has been launched, targeted not only on all prehospital and inhospital medical services, but also on all civil rescue services, namely policemen, firemen, city guards, border guards, and park rangers—everybody, who may come across hypothermic casualty. The center collaborates with all mountain rescue services in the region, and all search and rescue emergencies during the cold months (period from October 1 till April 30) are reported to HC; thus, possible hypothermic casualties are anticipated beforehand.
The National Chief Consultant of Emergency Medicine has sent a recommendation to all emergency departments in Poland that it is mandatory to measure core temperature (Tc) in all patients with confirmed or suspected hypothermia, and should the temperature be below 28°C, it is recommended to consult the patient with nearest ECMO center and consider extracorporeal rewarming. Furthermore, all medical and mountain rescue services are to be equipped with low-range thermometers.
Severe Hypothermia Treatment Center serves all patients of Malopolska Region (population 3.3 million; area 15.1 thousand square kilometers). To improve the quality of transport of arrested or hemodynamically unstable patients,6 the map of all available mechanical chest compression devices was created, which enables the coordinator to ensure that adequate quality of resuscitation is provided, also during long-distance transfers. The coordinator is in touch with both the emergency team and the dispatch center, helping to arrange the onsite team and gather as much information about the patient as possible, all of it being crucial in qualification for extracorporeal rewarming.
Whenever possible, the coordinator contacts a family of hypothermic patient to find any medical conditions that on the one hand may lead to hypothermia and on the other hand could exclude the patient from extracorporeal rewarming. Time for such decision-making is usually very limited with arrested or hemodynamically unstable patients, so all information is sought very carefully.
Modern means of telemetric data transfer enable the HC to see on an electronic tablet computer or mobile phone the print of electrocardiogram strip from defibrillator along with all other vital signs. As monitoring of hypothermic patients might sometimes be troublesome because of low metabolism rate, low heart rate, blood pressure, and respiratory rate with low exhaled CO2, cool extremities, or interference caused by shivering, the coordinator serves with expert knowledge on proper assessment of the vital signs. Furthermore, all medical emergency teams have been equipped with software that automatically suggests contacting HC if the patient is assessed as unconscious and hypotensive (systolic blood pressure below 90 mm Hg) and has a cold trunk or history of exposure to natural cold. Such telemetric monitoring and consultation is helpful during qualification for extracorporeal rewarming.
Another tool, complementing the possibility to consult with the HC, is a specially run website that covers all topics of basic management of hypothermic patients, as well as problems of qualification for extracorporeal rewarming, and links to corresponding articles and websites (www.hipotermia.edu.pl). It is meant to spread the knowledge on hypothermia to all rescue service and medical teams, and substantially improve patient management.
All hypothermic patients are classified depending on temperature and symptoms to one of five classes of hypothermia, according to Swiss hypothermia staging system (SHSS).7 Patients with class III (hemodynamic instability, Tc < 28°C) and class IV (hypothermic cardiac arrest, Tc < 24°C) are subjected to extracorporeal rewarming. Patients with class I (shivering, Tc > 32°C) and class II (hemodynamic stability, Tc < 32°C) require minimally invasive ways of rewarming, and after the HC provides instructions, they are managed in local hospitals. Class V casualties are ones with irreversible death caused by hypothermia. The severity of hypothermia alone does not determine the way of rewarming because there are many contraindications for extracorporeal rewarming, all of these being beyond the scope of this article. The implemented protocol is demonstrated in Figure 1.
Figure 1.
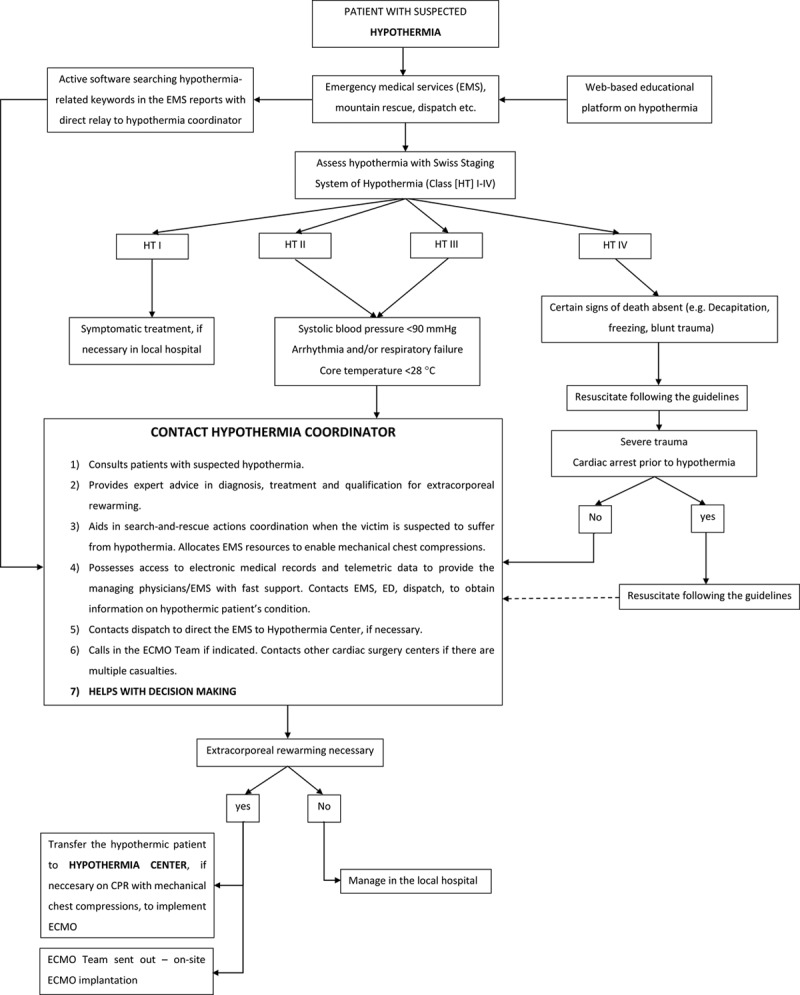
Schematic demonstration of hypothermia treatment in Malopolskie Region and the role of hypothermia coordinator.
Results
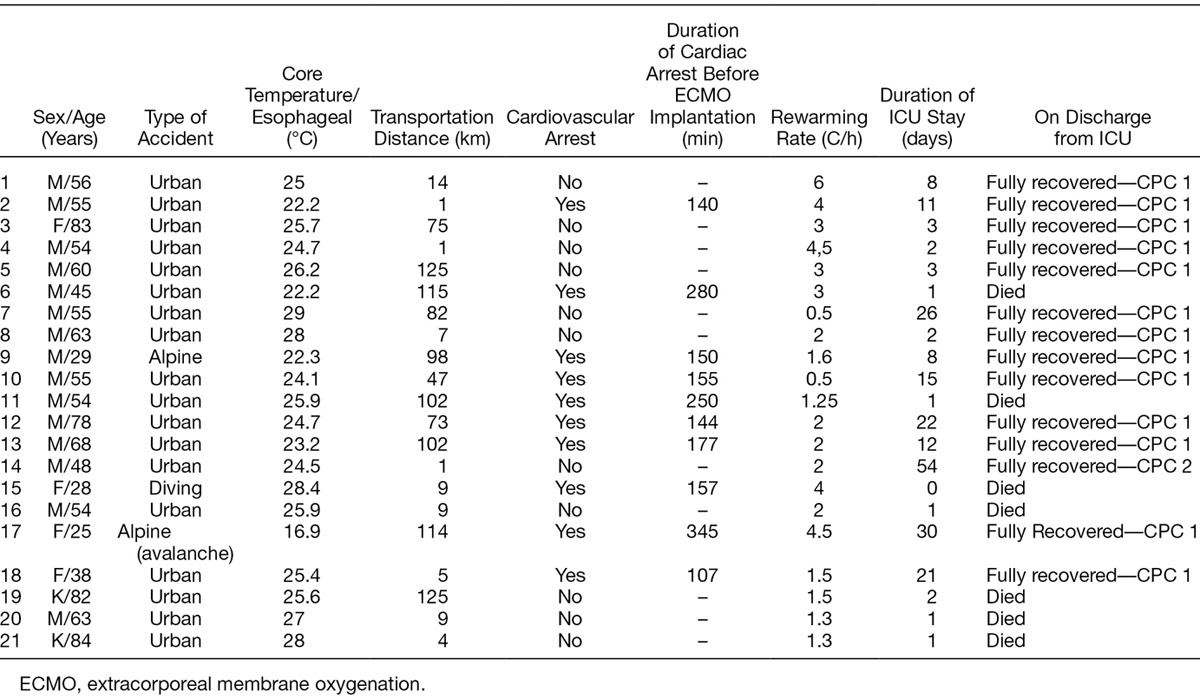
Since July 29, 2013 until November 1, 2015, the HC has consulted 104 hypothermic patients. Twenty-one patients were subjected to extracorporeal rewarming (SHSS class III and IV), and the remaining were rewarmed with less-invasive methods in the referring hospitals. Ten patients were arrested on referral, with cardiopulmonary resuscitation (CPR) times from cardiac arrest to ECMO implantation ranging from 107 to 345 minutes. Despite the treatment, seven patients died (three in hypothermia class IV and four in hypothermia class III) and the remaining 14 being rewarmed successfully with hemodynamic stability restoration and full neurologic recovery (GCS 15, CPC 1). The characteristics of the group are presented in Table 1.
Table 1.
Characteristics of Patients Subjected to Extracorporeal Rewarming in Cracow
Extracorporeal membrane oxygenation implantation in hypothermic patients is no different than in any other indication. As both cardiovascular and respiratory failures are observed along with severe hypothermia, implantation of venous-arterial ECMO is a treatment of choice in extracorporeal rewarming. Standard cannulas are used, and the easiest accessible sites of cannulation are the femoral vessels, unilateral or bilateral. There are, however, some difficulties that one should be well aware of. It is difficult to quickly puncture femoral vessels in an arrested patient or the one with a slow metabolic rate, so in our protocol we tend to implant cannulas surgically. Because restoration of normal temperature usually restores hemodynamic stability, unless there are no respiratory indications (i.e., aspirational pneumonia) we terminate ECMO support early, and hence little is the incidence of typical ECMO complications like bleeding or oozing, thrombosis or acute limb ischemia. None of the above has led to premature extracorporeal rewarming termination; however, we are aware that such complications are likely to occur, so extra caution is exerted to early recognition to any symptoms of ECMO treatment complications.
Neither the duration of resuscitation nor the mechanism of developing hypothermia (urban, wilderness, avalanche) had any impact on survival or neurologic recovery. However, it was the concomitant injuries and conditions (intoxication, submersion, injury to great vessels with occult bleeding) that caused fatalities, stressing the importance of proper qualification to extracorporeal rewarming.8 Full neurologic recovery in all surviving patients confirms the protective role of low temperature on central nervous system and encourages the aggressive treatment of all hypothermic casualties despite long CPR times.
Discussion
As the example of efficacy of Severe Hypothermia Treatment Center shows systematic approach to active recognition and treatment of patients with profound accidental hypothermia, on the basis of cooperation of HC representing cardiac surgery center with emergency, mountain rescue and transport services enable to perform high-quality advanced management, resulting in good outcomes, especially in patients in cardiac arrest. All of the above arrangements are novel, yet with growing number of cases managed, their utility being measured with lives saved has proven right. Therefore, further efforts are made to make this experience a template for national, and possibly European protocols of managing patients with profound accidental hypothermia.
At the same time, some improvements are being implemented or are planned, which are supposed to bring the management of hypothermic patients to even higher standards. The most important concept is the use of mobile ECMO system, which would be inserted onsite in a referring hospital, shortening the time of performed CPR and allowing for avoidance of hazardous transport of patient during cardiac arrest. Obviously, ECMO implementation outside ECMO center brings many challenges; however, it is believed to be a feasible procedure and hypothermic-arrested patients are good candidates for such management.
Along with developing the modalities offered by the center itself, the educational platform for all collaborating parties is updated. Now the online podcasts covering all problems of hypothermia pathophysiology, recognition, and treatment are written, and the project of Academy of Hypothermia is in progress of implementing. The aim is to spread the knowledge of hypothermia to all health care providers, so less patients are being mistreated.
Modern means of telemetric medicine are also in the scope of interest. One of the projects being investigated is a mobile core thermometer, which could be of use by all emergency teams, including mountain rescue services. For obvious reasons, the limitations of such a device are good reliability and small size, but the presented and tested prototype looks promising. The other project that is developed seems very innovative—a software that analyses words used to describe casualties, and if certain vocabulary is used, HC is alarmed. A preliminary study showed that this kind of automatic patient preselection could trigger as many as 1,000 consultations of possibly hypothermic patients a year (T. Darocha, unpublished data). All of the research is carried by the Cracow University of Science and Technology, Cracow, Poland, making the management of hypothermic patients truly multidisciplinary.
It is difficult to determine what are the surviving rates of hypothermic patients not subjected to described protocol. It is impossible to compare groups of patients from times before the onset of the project with more recent ones because previously hypothermic casualties were neither reported nor counted. Also the idea of comparing groups of hypothermic patients from other parts of the country with our results is erroneous because apart from the usual urban hypothermic casualties we are dealing also with far more difficult cases of alpine accidents.
As qualification for extracorporeal rewarming is reserved for patients with the most severe cardiogenic shock or cardiac arrest, in our opinion irreversible with conventional ways of treatment and rewarming, we believe that presented survivals would otherwise be fatalities. All of the described experience of Severe Hypothermia Treatment Center proves how systematic approach to active recognition and treatment of patients with profound accidental hypothermia brings good outcomes in managing these sometimes problematic patients. It is strongly encouraged that cardiac surgery centers having both equipment and experienced staff become natural candidates for leading this kind of activity.
Footnotes
Disclosure: The authors have no conflicts of interest to report.
This publication was supported by the Faculty of Medicine of Jagiellonian University Medical College (Leading National Research Centre 2012-2017).
References
- 1.Central Statistical Office of Poland: Demographic Base. 2015Warsaw, Central Statistical Office of Poland. [Google Scholar]
- 2.Kosiński S, Darocha T, Gałązkowski R, Drwiła R. Accidental hypothermia in Poland—Estimation of prevalence, diagnostic methods and treatment. Scand J Trauma Resusc Emerg Med 201523: 13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Darocha T, Kosiński S, Jarosz A, Gałązkowski R, Sadowski J, Drwiła R. Severe accidental hypothermia center. Eur J Emerg Med 201522: 288–291.. [DOI] [PubMed] [Google Scholar]
- 4.Brown DJ, Brugger H, Boyd J, Paal P. Accidental hypothermia. N Engl J Med 2012367: 1930–1938.. [DOI] [PubMed] [Google Scholar]
- 5.Wanscher M, Agersnap L, Ravn J, et al. Outcome of accidental hypothermia with or without circulatory arrest: Experience from the Danish Præstø Fjord boating accident. Resuscitation 201283: 1078–1084.. [DOI] [PubMed] [Google Scholar]
- 6.Holmström P, Boyd J, Sorsa M, Kuisma M. A case of hypothermic cardiac arrest treated with an external chest compression device (LUCAS) during transport to re-warming. Resuscitation 200567: 139–141.. [DOI] [PubMed] [Google Scholar]
- 7.Gordon L, Ellerton JA, Paal P, Peek GJ, Barker J. Severe accidental hypothermia. BMJ 2014348: g1675. [DOI] [PubMed] [Google Scholar]
- 8.Jarosz A, Kosiński S, Darocha T, et al. Problems and pitfalls of qualification for extracorporeal rewarming in severe accidental hypothermia. J Cardiothorac Vasc Anesth. 2016. In press. [DOI] [PubMed] [Google Scholar]