

Abstract
OBJECTIVE:
To assess the perspective of Saudi women in the Makkah region on breast cancer awareness and early detection.
MATERIALS AND METHODS:
A mixed method study was conducted among 25-65 years old healthy Saudi females from Makkah region during the awareness campaign in October 2014. The participants were recruited by personal invitations at the women's places of work and social gatherings. The initial invitations were issued by either the research coordinator or the investigator. All women were asked to complete a short questionnaire on basic knowledge on breast cancer. This was followed by focus group discussions. All interviews were carried out by female breast cancer consultant oncologists. All discussion transcripts were summarized and categorized into main themes; data presented as frequencies and percentages.
RESULTS:
Forty Saudi females, aged 25-65 years, were included in the study. Nearly 38% of them had never attended any awareness campaign on breast cancer. Only 10% of the participants correctly answered all five basic questions on the risk and early detection of breast cancer; 63% of the women had never been taught breast self-examination. Participants' perception was discussed in five focus groups. Four themes were identified during the discussions: knowledge about breast cancer and screening; resources of breast cancer awareness; social support for access to awareness program; and beliefs on breast cancer and early detection.
CONCLUSION:
We recommend that strategies on breast cancer awareness in our population should focus on early detection by improving the knowledge and skills of women. These strategies should include programs widely accessible through primary health-care centers and other health-care institutions. In addition, we recommend that physicians and family members should be involved in these programs.
Key words: Awareness, breast cancer, women's perspective
Introduction
Breast cancer is the most common cancer in females throughout the world.[1] In 2012, 1.7 million new cases of breast cancer were diagnosed. This represents 12% of all new cancers diagnosed and 25% of all cancer diagnoses in females.[2] In Saudi Arabia, breast cancer is the most common cancer in females. The last report on the incidence of cancer by the Saudi Health Council in 2013 showed that breast cancer accounted for 29% of all cancers in females and 16% of all cancers in Saudi adults of both genders. Only 33% of cases presented with localized disease of early stage compared to 42% that presented with regional disease, 13% of which were metastatic disease at presentation and 12% of unknown stage.[3] In the United States of America, the Surveillance Epidemiology and End Results database reported only 6% incidence of metastatic disease at presentation.[4]
Although the incidence of cancer is much less in developing countries than in advanced countries, mortality from cancer is higher, and patients continue to present with more advanced disease.[1] The stage of breast cancer at presentation is considered the most important prognostic factor. Early detection and management of localized disease that is limited only to breast influences the disease outcome and minimizes treatment morbidities. Data shows that cure rate in patients with localized breast cancer can reach up to 98%, and 84.4% in regional disease. This drops to 24.3% in cases of distant metastatic disease.[4] Despite the knowledge of the value of early detection in reducing breast cancer morbidity and mortality, we still come across in our clinics a large number of patients who present with more advanced stages of the disease.
Several factors might contribute to the late presentation of breast cancer in our population. Some of these factors are the women's lack of knowledge and awareness of breast cancer and early detection methods and the lack of population-based breast cancer screening programs. A study on breast cancer awareness and early detection in the Eastern Province of Saudi Arabia demonstrated that more than 80% of women were not aware of breast cancer screening modalities.[5]
Several reports have addressed the issues that militated against accessing, screening, and early detection. It was found that cultural beliefs, health practices, fear, lack of knowledge, social barriers, the stigma of the diagnosis of breast cancer, and the level of education were all contributory factors that hindered screening and early detection of breast cancer.[6,7,8,9,10]
Despite the availability of screening and diagnostic facilities for all Saudis, the majority of breast cancer cases are detected at advanced stages. Some studies suggest that increasing the knowledge and awareness of breast cancer would positively affect breast cancer screening practices. A cross-sectional study on the knowledge of women attending a primary health-care center in the western region of Saudi Arabia showed that 48% had poor knowledge of breast cancer and they found that age, the level of education, and being employed were significant positive predictors of the level of knowledge.[11] A study of Egyptian women in urban and rural areas recommended that culture-specific awareness programs in developing countries are essential for achieving the downstaging of breast cancer.[12]
We hypothesized that late presentation of breast cancer in our community might be related to the lack of knowledge, cultural beliefs, and social barriers, which interfere with awareness and early detection. We desired to address these in a qualitative study to get a better understanding of the issue from the women's standpoint. In addition, we wanted to be able to make recommendations for the national planning of breast cancer and health promotion programs on what the priorities should be from the women's perspective to improve results of the programs.
We conducted this study on Saudi women in the Makkah region to assess their knowledge and perceptions of breast cancer and early detection.
Materials and Methods
Women were eligible if they were healthy Saudis aged 25–65 years from the Makkah region. Females with a previous history of breast cancer were excluded from the study. The participants were recruited either from their places of work or from the hospital's family medicine clinic waiting area. All eligible participants were invited initially either by a phone call or direct communication to participate in the study. Formal invitations were given by either the research coordinator or investigator to individuals or groups by handing out the questionnaire or an interview during prearranged visits to the workplaces of the women or participants' gatherings. To ensure a diverse study population, it was necessary to select women of different ages. All participants were introduced to the survey by the study coordinator or investigator. The focus group interview was conducted by one of the main investigators, a female breast cancer consultant oncologist. The interviewer started with a discussion of the study and asked all who agreed to participate to sign the approved Institutional Review Board consent form to participate in the study and for the discussion to be audio recorded. At the beginning of each interview, the investigator asked each participant to complete a short questionnaire on demographic data and basic knowledge about the risk of and screening for breast cancer.
A mixed study design of quantitative and qualitative approaches was used. A focus group discussion was selected as the primary methodology to collect in-depth information from groups of eligible women to achieve the study objective. All interviews were preceded by the completion of a questionnaire on the participant's demographic data and basic knowledge on breast cancer risk and screening. All the five focus group discussions were conducted at the same setting. Each group comprised 6–10 female participants of the same predefined age group to minimize shyness. There were three groups aged 25–49 and two groups aged 50–65 years.
The focus groups each had a facilitator, a female breast cancer consultant oncologist experienced in conducting breast cancer awareness. All interviews were conducted in Arabic. A semi-structured questionnaire consisting of 19 questions was used to facilitate and guide the discussion to ensure consistency of all interviews. The group discussions included breast cancer risk, diagnosis, treatment, screening, early detection, and breast cancer awareness resources. Two interviewers were in charge of the discussions. One investigator conducted the interview while the other recorded and took notes of the discussion. Each interview took 60–90 min. All interviews and discussions were audio recorded and transcribed and coded in Arabic. All codes were translated into English by a single research coordinator who had a good command of English. The two investigators independently reviewed the translated codes and categorized them into main themes.
This study was approved by the Institutional Review Board of King Abdullah Medical City. All participants were informed of the purpose of the study and the fact that participation was voluntary. Informed consent was obtained from each participant to audio record the interview. Confidentiality was observed throughout the study process.
Results
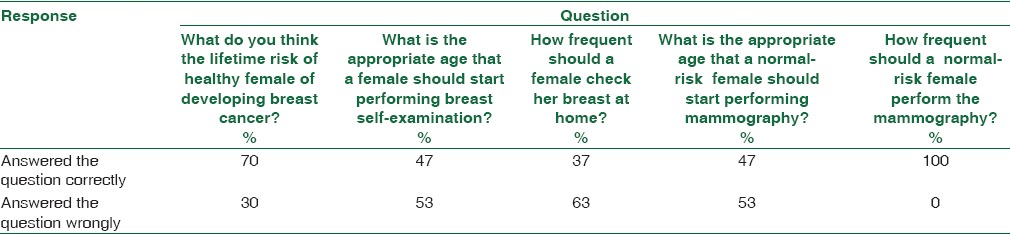
Forty Saudi women from the Makkah region aged 25–65 years participated in five focus groups. More than 70% of the women included in the study were college or university educated and employed; 73% had no family history of breast cancer. Social and demographic characteristics of the participants are shown in Table 1. Thirty-eight percent of the participants had never attended any awareness campaign or lecture on breast cancer. Sixty-three percent never had any formal instruction on breast self-examination. Forty-five percent of the participants never had any practice of breast self-examination [Table 2]. When the women were asked the five questions on the basic knowledge of breast cancer risk and schedule of methods of early detection, only 10% of the participants knew enough to answer all the basic knowledge questions correctly [Table 3].
Table 1.
Socio-demographic characteristics of study participants
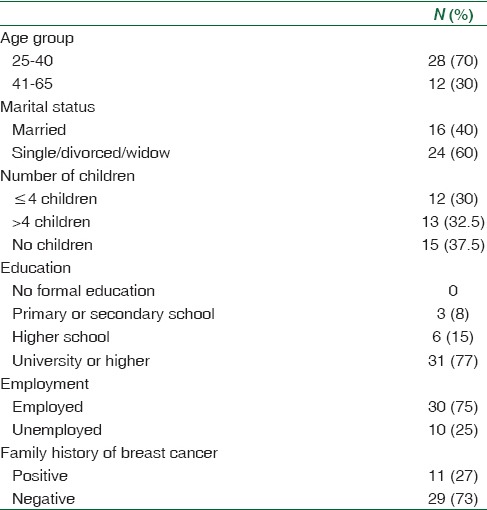
Table 2.
Participants' responses to basic skills questions about early detection of breast cancer
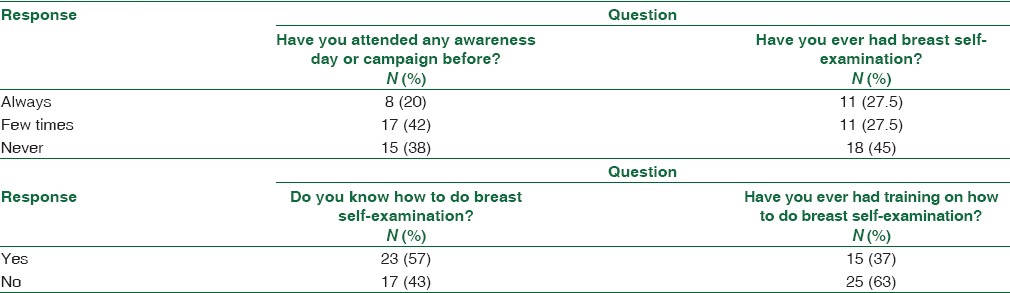
Table 3.
Participants' responses to basic knowledge questions about breast cancer risk and early detection
Participants' perceptions about breast cancer awareness and early detection were discussed in all the focus groups. Four main themes were identified during the discussion: knowledge about breast cancer and screening program; resources for breast cancer awareness and health promotion; social and family support to access for breast cancer awareness; and women's beliefs and attitudes toward breast cancer and early detection.
The first theme was about knowledge of breast cancer and screening program. The majority of women in the focus groups realized the impact of early detection of breast cancer in reducing disease mortality. In addition, they had a clear understanding of the importance of early detection and screening for breast cancer to reduce the complications of treatment for the disease. Some had the misperception that early diagnoses would completely eliminate breast surgery. A review of the basic knowledge of breast cancer risk and screening program showed that the majority of participants had overestimated their knowledge. Most did not have enough knowledge of lifetime risk and the scheduling of different methods for the early detection program.
The second theme was about resources for breast cancer awareness and health promotion. The majority of the women were not satisfied with the sources of information and awareness programs. They pointed out that “these awareness programs are seasonal and not done throughout the year to accommodate our social commitments.” The majority of women never had any awareness campaign at work or school; the majority also thought that shopping malls were not the best venues for programs on the awareness of breast cancer. Most of the women commented that “shopping malls are for shopping.”
The majority of women in the groups had never watched videos or TV programs on breast cancer or breast cancer examination or early detection methods. The majority of women did not have any formal instruction on breast self-examination and they were not certain of what and when they should use the screening methods. The minority who had some form of training said: “This was carried out by a family member who is a physician.” The majority of women expressed their preference for their breasts to be checked by a doctor rather than themselves even if they knew how to do the breast examination. Some said, “This makes me more comfortable because I do not want to discover anything myself.” Participants advocated the use of a combination of different approaches to communicating the knowledge on breast cancer and early detection methods. Women aged below forty said they preferred awareness campaigns and interactive sessions in health-care facilities. They opined that “I trust the information given by doctors at the hospital or the primary health-care center.” While older women in the groups aged fifty and above preferred a variety of methods to acquire knowledge and awareness such as programs disseminated by the media and TV shows.
The third theme was about social and family support for access to breast cancer awareness. The majority of the women indicated that their families did not provide enough support to attend awareness campaigns, mainly because of transportation difficulties and time constraints. The majority of the married women did not think that they had enough time to discuss health matters with their husbands. The majority did not feel comfortable discussing breast cancer risks with family members, but felt more comfortable in open discussions with friends.
The fourth theme was about women's beliefs and attitudes toward breast cancer and early detection. The majority of the women were afraid of the disease because of consequences of treatments such as loss of the breast, chemotherapy, and hair loss. Despite these fears, most of the women believed and valued their own health as a priority, especially because they had families to take care of. The majority believed that they were responsible for their own health and said, “I will seek immediate attention from a doctor if I find a lump in my breast.” When asked which physician they will see if they felt a lump in their breast, some said, “I will go to my gynecologist,” but the majority had no particular doctor or specialty or hospital in mind they would go to for advice. The majority believed that the diagnosis of breast cancer was a test from the God, but it bore no relation to any kind of punishment from the God. Some of the women believed that it could be a result of envy. The majority of women did not think that breast cancer would stigmatize the family and they would not feel the need to withhold information of the diagnosis of this disease from others.
Discussion
Although many women in our study had very little knowledge of breast cancer risk and had limited family and social support for acquiring awareness of breast cancer, they had positive perceptions of early detection of the disease and the value of prioritizing their own health. The majority accepted the diagnosis of breast cancer as a test from the God and did not have inordinate fear or anxieties that would make them unwilling to disclose the diagnosis. None of the participating females thought that they would not divulge the diagnosis because of the dread of family stigma or feelings of diminished femininity. Despite the fact that some women would rather not do breast self-examination and preferred clinical examination, the majority of women were comfortable with the idea of acquiring knowledge about breast cancer and skills of breast self-examination to help reduce their anxiety and encourage them to seek early detection.
In contrast to our population, Taha et al. in a similar study of Jordanian females found that fear could be a potential barrier to screening, as women feared that if they went for screening they might discover that they had breast cancer and felt they would rather not know.
From the information gathered from our focus groups of Saudi women in the Makkah region on their perceptions of breast cancer and early detection, we recommend that health promotion programs must be tailored to the beliefs and attitudes of our population. The design of the program should make use of the positive attitudes of women and their willingness to accept the diagnosis, their recognition of the value of early detection, and acceptance of responsibility for their own health. In addition, it should note the legitimate fear of breast cancer to promote the awareness of breast cancer and early detection of the disease.
From the women's perspective, we suggest that health promotion programs and initiatives should be well structured, community sensitive, and cognizant of all social and family commitment and concerns of Saudi women. These programs should be provided on a wider scale at accessible health promotion centers or at primary health-care centers since these are widely distributed in the country. These centers should have frequent regular sessions on breast cancer awareness and early detection. They should acknowledge the preference of females to have their examination done by physicians and the trust they have in the physicians and use them as promoters of the programs. Furthermore, they should engage family members in breast cancer awareness and health promotion programs. This will boost family and social support for the women and promote breast cancer awareness and early detection. The media should be engaged as a major partner in breast health promotion.
The main limitation of the current study was the small number of the study population. Primarily because of the qualitative nature of the study, it was hard to recruit a large number of participants. Second, the majority of our participants were highly educated which makes the findings of this study inapplicable to Saudi women in general, though it could represent a good percentage of Saudi females in our region.
Conclusion
We recommend that national strategies for breast cancer awareness and early detection should be driven by the perspectives and attitudes of Saudi women. These strategies and programs should stress on improving knowledge and developing the skills of women to facilitate the early detection of breast cancer. The programs should be accessible and widely available at primary health-care centers. These strategies should engage other family members and use physicians as promoters.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 2.Stewart BW, Wild CP. World Cancer Report 2014 [Google Scholar]
- 3.Kingdom of Saudi Arabia Saudi Health Council Saudi Cancer Registry. Cancer Incidence Report Saudi Arabia 2013 [Google Scholar]
- 4.Howlader N, Noone A, Krapcho M, Neyman N, Aminou R, Altekruse S, et al. SEER cancer statistics review, 1975-2009 (vintage 2009 populations) Bethesda, MD: National Cancer Institute; 2012. [Google Scholar]
- 5.Abdelhadi MS. Breast cancer awareness campaign: Will it make a difference? J Family Community Med. 2006;13:115–8. [PMC free article] [PubMed] [Google Scholar]
- 6.Taha H, Al-Qutob R, Nyström L, Wahlström R, Berggren V. “Voices of fear and safety” women's ambivalence towards breast cancer and breast health: A qualitative study from Jordan. BMC Womens Health. 2012;12:21. doi: 10.1186/1472-6874-12-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Lee-Lin F, Menon U, Nail L, Lutz KF. Findings from focus groups indicating what Chinese American immigrant women think about breast cancer and breast cancer screening. J Obstet Gynecol Neonatal Nurs. 2012;41:627–37. doi: 10.1111/j.1552-6909.2012.01348.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Bener A, Honein G, Carter AO, Da'ar Z, Miller C, Dunn EV. The determinants of breast cancer screening behavior: A focus group study of women in the United Arab Emirates. Oncol Nurs Forum. 2002;29:E91–8. doi: 10.1188/02.ONF.E91-E98. [DOI] [PubMed] [Google Scholar]
- 9.Vithana PV, Hemachandra NN, Ariyaratne Y, Jayawardana PL. Qualitative assessment of breast cancer early detection services provided through well woman clinics in the district of Gampaha in Sri Lanka. Asian Pac J Cancer Prev. 2013;14:7639–44. doi: 10.7314/apjcp.2013.14.12.7639. [DOI] [PubMed] [Google Scholar]
- 10.Ibrahim EM, al-Idrissi HY, al-Khadra AH, Kurashi NY, al-Jishi FM, Saied I, et al. Women's knowledge of and attitude toward breast cancer in a developing country: Implications for program interventions – Results based on interviewing 500 women in Saudi Arabia. J Cancer Educ. 1991;6:73–81. doi: 10.1080/08858199109528095. [DOI] [PubMed] [Google Scholar]
- 11.Rasheed P, Soweilum LS. Knowledge and perception of breast cancer and practice of breast self-examination among female patients attending primary health care centers in Al Khobar City, Saudi Arabia. J Kuwait Med Assoc. 2013;45:123–9. [Google Scholar]
- 12.Uddin N, Fateem E, Hablas A, Seifeldin IA, Brown E, Merajver SD, et al. Public and professional educational needs for downstaging breast cancer in Egypt. J Cancer Educ. 2012;27:149–55. doi: 10.1007/s13187-011-0282-3. [DOI] [PMC free article] [PubMed] [Google Scholar]