

Abstract
We report a case of persisting nictitating membrane in a 9-year-old girl presenting to us with the complaints of fleshy mass in the medial part of the left eye since birth, which was nonprogressive. On examination, her left eye was amblyopic with a vision of 20/500. The membrane was continuous with the medial canthus and was spread in a horizontal fashion, covering the underlying bulbar conjunctiva and one-third of the cornea. The globe however moved freely underneath the membrane, indicating no attachment between the globe and overlying membrane. The patient underwent simple excision of the nictitating membrane with good outcome.
Key words: Nictitating membrane, plica semilunaris, vestigial organ
The first anatomical description of nictitating membrane in the eye was made by Owen in 1866. He describes this as a membrane stiffened by cartilage and covered in conjunctiva which moves horizontally across the eye, from the inner to the outer corner, in birds.[1] As the humans and most other primates have evolved over the years, the nictitating membrane in them has dwindled away to a small vestigial structure called as the plica semilunaris, membrana nictitans, or palpebra tertia. After a thorough literature search, this is only the second such case report of a persisting nictitating membrane in a human being.
Case Report
A 9-year-old girl was brought by her mother with the complaints of fleshy growth in her left eye noticed since birth, which was nonprogressive. There was no preceding history suggestive of mechanical/chemical/thermal injury to the eye, no history of ocular surgery, or any history of fever with eruptive skin lesions. Prenatal history in the mother was unremarkable. On examination, her left eye was amblyopic with a best-corrected visual acuity (BCVA) of 20/500, N12. The right eye had a BCVA of 20/20, N6. Her left eye was exotropic with eccentric fixation. On slit-lamp examination, a translucent membrane arising from medial canthus and spreading out in a horizontal fashion over the bulbar conjunctiva and covering one-third of the cornea in the primary gaze, with its superior end attached to the palpebral conjunctiva of upper lid just posterior to the posterior lid margin and its inferior end attached to the palpebral conjunctiva of lower lid just posterior to the posterior lid margin was noted. Lateral border was free. There was no attachment to the underlying bulbar conjunctiva or the cornea, and the globe moved freely underneath the membrane. The dimensions of the membrane were 20 mm horizontally and 18 mm vertically [Figs. 1 and 2]. Anterior segment examination of the left eye was normal, and pupil was 3 mm and reacting normally to light. Lens was normal and clear. Posterior segment revealed a healthy fundus. The right eye examination was normal. There were no signs of cicatrization in both eyes. Axial length of the right eye was 22.46 mm and of the left eye was 22 mm. Extraocular movements were full and free in both eyes. On dextroversion, the membrane covered up to three-fourth of the cornea of the left eye. General physical and psychological examination showed no pathology. There were no similar complaints in her family members. The patient was referred to a pediatrician to rule out occult systemic developmental abnormalities, and the results were normal. A clinical diagnosis of persistent nictitating membrane in the left eye was made. We posted the girl for excision, the membrane under general anesthesia. Consent for the surgery and general anesthesia was obtained from both of her parents. The membrane was released from its nasal, superior and inferior attachments. Raw area over the palpebral conjunctiva was closed with 8-0 Vicryl sutures. The underlying conjunctiva and cornea were normal; there were no attachments noted from the membrane. Fornices were normal and the plica semilunaris was restored. The sample was sent for histopathological examination. Postoperatively, tobramycin with dexamethasone eye drops in a tapering dose was given over 3 weeks and stopped along with a lubricant. Recovery was uneventful [Fig. 3]. Patching for the left eye for 3 h a day was advised at discharge, and at the end of 1 month, there was no improvement noted in the vision in the left eye, indicating a deep amblyopia in it. Histopathological report showed stratified squamous epithelium with underlying loose areolar connective tissue and nonspecific inflammatory cells around blood vessels. No elastic, reticular fibers, cartilaginous structures, or muscle cells could be found [Fig. 4]. This confirmed our diagnosis of a persistent nictitating membrane which is an extension of plica semilunaris.
Figure 1.
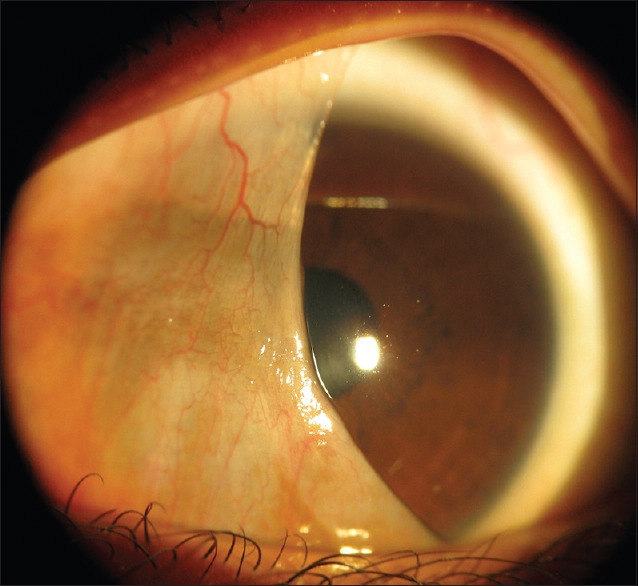
Left eye membrane, covering the bulbar conjunctiva and the cornea
Figure 2.
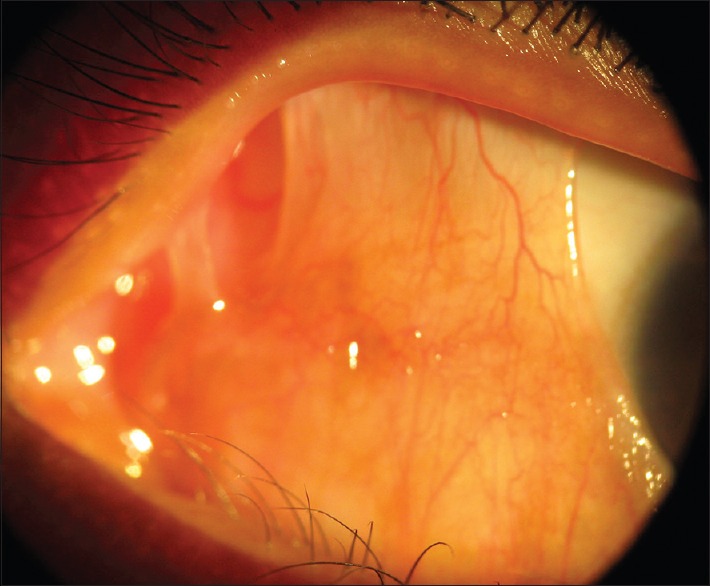
Left eye membrane, having attachment to medial canthus
Figure 3.

One-month postoperative, left eye showing complete resolution of membrane with normal conjunctiva and cornea
Figure 4.
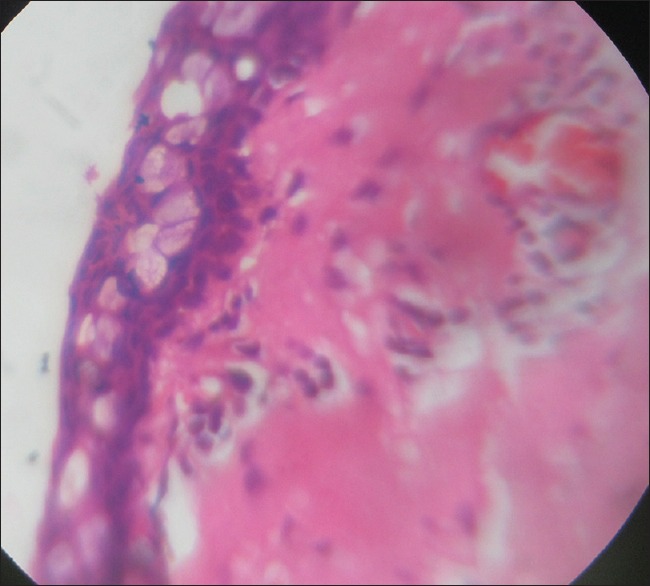
Histopathological picture showing stratified squamous epithelium with underlying loose areolar connective tissue and nonspecific inflammatory cells around blood vessels
Discussion
The nictitating membrane is a transparent or translucent third eyelid present in some animals that can be drawn across the eye for protection and to moisten it while maintaining visibility. Fully developed nictitating membranes are found in fish, amphibians, reptiles, birds, and mammals but are rare in primates. In humans, the plica semilunaris (also known as the semilunar fold) and its associated muscles are homologous to the nictitating membrane seen in some other mammals and other vertebrates.[2] The presence of nictitating membrane in humans is rare and only one such case report by García-Castro and Reyes de Torres was found in the literature where they describe a newborn with features of trisomy 18 syndrome having bilateral nictitating membrane.[3] Arends and Schramm in their study on the eyes of eleven fetuses at different stages of gestation, two newborns and an old man, found that in the early stages of its development, the plica semilunaris covered a bigger part of the orbit and later did not keep up with the growth of the eyeball and the lids. Histologically plica consists of a higher number of epithelial layers (two-layered cuboidal to a multilayered cylindrical epithelium) and more goblet cells. In the tight collagenous connective tissue, no elastic, reticular fibers, cartilaginous structures, or muscle cells are seen. A few unmyelinated neurofibers are usually found next to blood vessels and glands. Lymphoplasmacytic elements, granulocytes, and macrophages could also be seen around the blood vessels and in the subepithelial area, indicating that plica semilunaris could be a part of the human ocular immune system.[4] Our patient is the second case to be reported, with persistent nictitating membrane in one eye with no associated systemic disorder.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to acknowledge the Management of Sankara Eye Hospital, Shimoga
References
- 1.Owen R, editor. Anatomy of Vertebrates. 1st ed. London: Longmans, Green and Co.; 1866. Organ of sight in birds. Available from: https://www.archive.org/stream/onanatomyofverte02owen#page/142/mode/2up . [Google Scholar]
- 2.Stibbe EP. A comparative study of the nictitating membrane of birds and mammals. J Anat. 1928;62:159–76. [PMC free article] [PubMed] [Google Scholar]
- 3.García-Castro JM, Reyes de Torres LC. Nictitating membrane in trisomy 18 syndrome. Am J Ophthalmol. 1975;80:550–1. doi: 10.1016/0002-9394(75)90228-7. [DOI] [PubMed] [Google Scholar]
- 4.Arends G, Schramm U. The structure of the human semilunar plica at different stages of its development – A morphological and morphometric study. Ann Anat. 2004;186:195–207. doi: 10.1016/S0940-9602(04)80002-5. [DOI] [PubMed] [Google Scholar]