

Abstract
Progress in locomotor rehabilitation has created an increasing need to understand the factors that contribute to motor behavior, to determine whether these factors are modifiable, and if so, to determine how best to modify them in a way that promotes improved function. Currently available measures do not have the capacity to distinguish between neuromotor recovery and compensation for impaired underlying body structure/functions. The purpose of this Special Interest article is to examine the state of outcomes measurement in physical therapy in regards outcomes to locomotor rehabilitation, and to suggest approaches that may improve assessment of recovery and clinical decision-making capabilities. We examine historical approaches to measurement of locomotor rehabilitation outcomes including rating scales, timed movement tasks, and laboratory-based outcome measures, and we discuss the emerging use of portable technology to assess walking in a free living environment. The ability to accurately measure outcomes of rehabilitation, both in and away from the laboratory setting, allows assessment of skill acquisition, retention, and long-term carryover in a variety of environments. Accurate measurement allows behavioral changes to be observed and assessments to be made, not only regarding an individual's ability to adapt during interventions, but also their ability to incorporate new skills into a real-world behavior. The result of such an approach to assessment may be that interventions truly translate from laboratory to real-world environments. Future locomotor measurement tools must be based on a theoretical framework that can guide their use to accurately quantify treatment effects and provide a basis upon which to develop and refine therapeutic interventions.
Introduction
The ever-expanding knowledge base of rehabilitation science is producing substantial opportunities for both clinicians and researchers to improve clinical effectiveness. Clinical research is continually evolving due to the growing understanding of neuroplasticity and its impact on rehabilitation,1 the increased emphasis on recovery-based versus compensation-based to programs,2 and the infusion of biomedical engineering into emerging interventions and clinical research. Translational research is bridging the gap between basic and clinical sciences, and partnerships spanning research domains are allowing knowledge to grow at an unprecedented rate. Furthermore, there are growing opportunities to partner with existing clinical enterprises to translate research findings into clinical practice to provide clinicians with more “evidence-based” options and to promote improved clinical decision making. While there is mounting research indicating that therapy aimed at remediating neuromotor deficits is possible, and may be best practice for some with neurological injury or disease, the evidence to confirm this has been limited.3,4
The measurement tools commonly used in the clinic to assess changes in locomotion generally do not provide specific information about what aspects of gait have been responsive to training. Given the need for evidence to guide practice, attention to the “measurement” tools used to define the outcomes of therapy is critical, and as such, questions such as: “what does a measurement tool actually measure” and “what does the score or time mean?” must be considered. In the past, assessment tools have focused on the end result of a motor behavior. However, there is need to understand factors that contribute to the performance of a motor behavior, and whether/how these contributing factors are alterable.
Traditional assessment tools may provide information about whether or not a task is accomplished, but little information about the mechanisms underlying the accomplishment of the task. They are unable to discern, for example, whether observed increases in walking speed are due to compensatory strategies such as increased speed of hip hiking and circumduction, or through restoration of normal movement patterns that lead to more efficient gait. Therefore, there is a need for task performance measures that provide information about the underlying neuromotor mechanisms. Rehabilitation outcomes measurement has not adapted to the requirements of interventions designed to remediate neuromotor deficits, and as a result traditional outcomes measurement instruments leave clinicians and researchers unable to answer two important questions: 1) does improvement in a measure imply that the patient “recovered” neuromotor behavior or simply compensated more efficiently for impaired underlying body function/structures? and 2) does the measurement instrument assist clinical decision-making by providing information that will allow the clinician/researcher to select the most appropriate treatment option? The purpose of this article is to examine the state of outcomes measurement in neurologic physical therapy specific to locomotor rehabilitation and to suggest potential avenues for improvement to assess recovery and improve clinical decision-making capabilities.
Defining Recovery
Moving toward a neurorehabilitation framework that targets recovery requires careful definition of the term “recovery”. The current literature can be confusing as “recovery” is often used interchangeably to refer to the amelioration of structural deficits within the nervous system (body functions and structures of the International Classification of Function, Disability, Health [ICF])5 as well as improvement in physical capacity and performance (activity and participation levels of the ICF)5 as the result of a neurorehabilitation intervention.6 At a neural level, most researchers would agree that “recovery” after stroke connotes reactivation of neural substrates previously deactivated either directly by the stroke or indirectly by the post-stroke maladaptive plasticity.6 “Recovery” of walking performance, however, often does not distinguish between restitution of a pre-pathological pattern of movement versus an adaptive compensatory response relying on altered performance of various neuroanatomical structures.
Examining performance of a motor task to distinguish neuromotor recovery from compensatory adaptations requires a level of measurement that is currently uncommon and largely unapplied to the field of rehabilitation in general, and neurorehabilitation specifically. Now that the potential for restorative therapy is clear, neurorehabilitation should no longer be limited to the compensatory frame of reference that guided most 20th century therapy techniques.2 This restricted view of recovery has been based on the predominant theory that the nervous system is hard-wired and incapable of repairing itself after injury and disease,7 and therapists relied on strategies to compensate for the irremediable effects of weakness, decreased balance, and limited motor control.2
Assessment of Task Performance
The following discussion of task performance assessment will focus on walking ability for purposes of illustration, as walking is a common focus of rehabilitation efforts in many neurologic clinical populations. Current clinical tools for assessing walking ability are based on physical performance measures such as walking speed, distance walked, physical independence, and observational methods of balance control. However, the assessment of gains in walking performance, as currently clinically measured often do not provide an understanding of whether the improvements were attained via neuromotor restitution or acquisition of new compensatory strategies. This failure to distinguish adequately the effect of the interventions not only limits determination of therapeutic efficacy, but it also fails to distinguish those who may maximally benefit from recovery-based interventions from those who would perhaps optimize their ability to perform valued activities with a compensatory approach. Historically, locomotor rehabilitation measurement has incorporated assessments using 1) rating scales, 2) timed movement tasks, and 3) laboratory-based outcomes measurement. As a progression of these assessments, we will discuss the emerging use of portable technology to assess non-laboratory walking outcomes and task-specific motor control. In the following sections, each of these categories of measurement will be discussed and future directions will be suggested.
Rating scales
Many rehabilitation outcomes are measured by documenting a patient's ability to perform a set of items using an ordinal rating scale. For example, the Berg Balance Test (BBT, which is not an assessment of gait performance but often used to document outcomes from locomotor rehabilitation studies)8,9 documents the ability to accomplish 14 balance tasks using a 5-point rating scale (0 = unable or requires maximal assistance, 4 = safe and independent).10 Although many rating scale assessments such as the BBT have well-established measurement properties, rating scale assessments can be inefficient to administer, have limited precision, and often yield scores that are difficult to interpret. These limitations are due, at least in part, to traditional psychometric methodologies which evaluate the assessment at the whole-test rather than item-level.11 Reliability, validity, and responsiveness are established for the whole test, which means that all items must be administered regardless of whether an item is appropriate for a patient's situation or appropriately matched to his/her skill level, and requirements to administer a whole test sacrifice both efficiency and precision.11 In addition, as there are a myriad of item-level ratings that contribute to a rating scale summary scores, individuals may have similar summary scores, yet exhibit dissimilar patterns of motor behavior. Lastly, rating-scale assessments do not indicate how underlying neuromotor mechanisms changed (or did not change) with therapy and therefore fail to distinguish between recovery and compensation.
Timed movement assessments
The flaws inherent in rating scales of task performance may be improved upon by timing individual tasks, thus improving interpretability of scores and reducing confusion over interpretation of summary scores. For example, much of the literature regarding locomotor rehabilitation has used self-selected walking speed as the primary outcome variable. Walking speed has been advocated as the sixth vital sign and has been described as an ideal measure12 because it is simple to measure, inexpensive, reliable, valid, sensitive, and specific.13 In addition, it is an important outcome measure of locomotor rehabilitation because it reflects both physical performance and physiological changes,14,15 remains reliable and sensitive to change even as recovery advances,16 and is a predictor of health status17 as well as quality of life.15 Walking speed has been used as the primary outcome measure for many clinical trials of locomotor-related interventions for persons with stroke, such as exercise therapy,18 lower extremity strength training,19,20 functional electrical stimulation,21 treadmill walking,22,23 and locomotor training with treadmill and body weight support.24,25 A recent meta-analysis demonstrated that these approaches, although very different, led to similar gains in walking speed.4 The analysis indicated that no intervention was superior to others, and therefore the author suggested clinical decision-making should be guided by a “pragmatic approach”.4 The inability to detect an interaction between type of treatment and treatment effect may be related to limitations of walking speed as an outcome measure, as it fails to reflect true neuromotor recovery. In other words, many interventions increase walking speed, but it is not clear which are the types of interventions lead to changes in underlying mechanisms (recovery) versus promote acquisition of new, compensatory walking strategies (compensation). Because of this failure to link treatment type with a specific treatment effect, a measure of walking speed does not provide the information necessary to guide treatment approaches. Therefore, it is important to develop walking-specific measures of motor control in order to target intervention at a well-defined motor control deficit. Such measures will specify an effective treatment approach and more clearly define intervention effects.
Laboratory-based measurement of walking specific motor control
Uncertainties about the specific benefits of different types of locomotor treatment approaches may also be due to the heterogeneity of motor control problems that exist in persons with neurologic injury. These problems must be well quantified in order to assure a homogenous sample and to more clearly define treatment effects. Biomechanical measurements of joint angle, ground reaction force, velocity, and acceleration precisely quantify movement and force production.26 In the past decade, researchers have begun using quantifiable biomechanical variables as outcome measures for interventions intend to reduce impairments (such as strength training27-29) and for improving task performance (such as locomotor training30,31). Modern movement science laboratories may contain advanced equipment such as split-belt instrumented treadmills, capable of measuring the three-dimensional ground reaction forces and the ground reaction moments, from which the center of pressure under each foot is calculated. The most important advantage of this type of advanced instrumentation is that bilateral kinematics, kinetics, and electromyography can all be continuously monitored for a large number of consecutive cycles in order to precisely determine the steady state walking pattern with its associated variability. Additionally, portable sensored walkways allow for immediate interpretation of the spatial and temporal components of the gait cycle, and these components may be related to specific motor control deficits.32,33
Advanced instrumentation allows for investigation into underlying mechanisms of motor control impairment, and thus may allow for differentiation between neuromotor recovery and behavioral compensation. As an example, using the anterior-posterior component of the ground reaction force (AP GRF), we recently proposed paretic propulsion (Pp) as a single measure of coordinated motor control specific to walking.34 Figure 1 illustrates the AP GRF propulsion values for two representative participants with poststroke hemiparesis. In order to maintain steady state walking speeds, reduced net propulsion by the paretic leg must be offset by increased propulsion in the non-paretic leg. In the group analysis of 18 subjects, Pp was significantly correlated with both speed (r=0.551) and with severity of hemiparesis as measured by Brunnstrom staging (r=0.737). Five of the 18 individuals with severe hemiparesis, however, walked faster than 0.8 m/s (associated with community ambulation potential)14 and all had propulsion values of Pp ≤ 25%. Attainment of near-normal speeds in this group implies that a compensatory strategy was utilized to overcome the lack of ability to generate propulsive forces.
Figure 1. Comparison of the anterior-posterior ground reaction forces (AP GRF) for the paretic (black lines) and non-paretic legs (grey lines) of subjects of differing severity of hemiparesis.
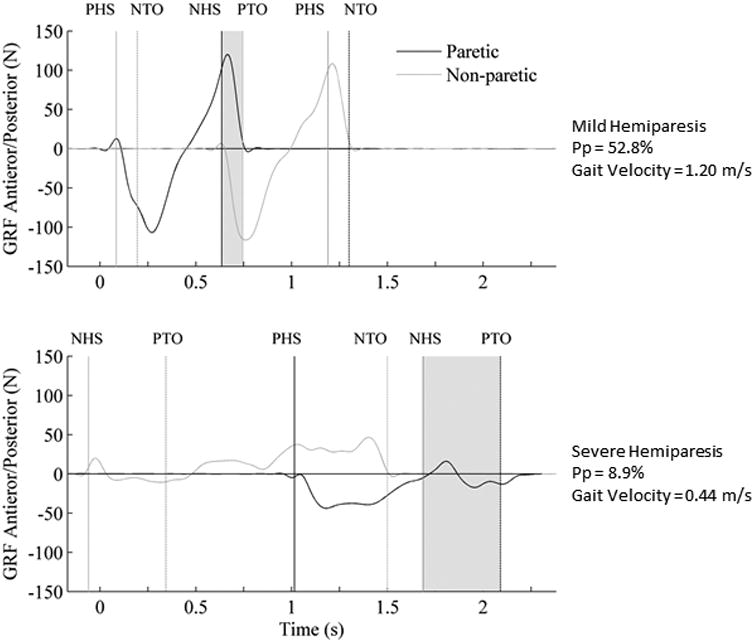
Positive values represent propulsion, and the positive area under the curve is the propulsive impulse. Solid vertical lines indicate heel strike and dashed vertical lines indicate toe-off. Increased hemiparetic severity was associated with decreased paretic propulsion (Pp) and decreases in self-selected walking speed. (PHS = paretic heel strike; NTO = non-paretic toe off; NHS=non-paretic heel strike; PTO = paretic toe off; PHS = paretic heel strike; and NTO = non-paretic toe off)
The level of Pp may be useful in directing treatment strategies. A low Pp value indicates a low level of force production relative to the non-paretic leg, and may cue the clinician to prescribe extensor strengthening exercises (to increase active force production) and encourage increased hip extension (to increase mechanical force production). Conversely, while a high Pp indicates that more propulsion is achieved in the paretic leg than in the non-paretic leg, it does not imply that the force production approximates normal in the paretic leg, but rather that the biomechanical positioning required to achieve propulsion (excessive hip extension and prolonged double limb support) compromise contralateral force production. Normalizing timing and coordination of the gait cycle focusing on stance-to-swing transition may be target goals for this subgroup. Lastly, a sub-group that demonstrates speed deficiencies with no symmetry deficits, and may benefit from high intensive, task-specific walking training.
Paretic propulsion and other biomechanical measures, however, require costly equipment and technological expertise, and the data can require a great deal of time to acquire and analyze, making their application in the clinic almost impossible. However, technological advancements are allowing data collection to be expanded beyond the walls of the research laboratory and capture not only quantifiable physical walking performance data, but also information to guide understanding of underlying mechanisms. For example, from data captured using an instrumented walkway, we determined that Pp has a very strong inverse relationship with the paretic step ratio (PSR).33 PSR is calculated by dividing the paretic step length by the stride length, yielding a symmetry value of 0.5 (similar to Pp). A high PSR value (ie, a longer step with the paretic leg) represents a similar measurement construct to low Pp and mechanistically relates to larger and poorly timed flexor muscle activity.35 Low PSR values (taking a shorter step with the paretic leg) are analogous to high PSR and reflect the previously described difficulty with timing and coordination. High and low PSR values are defined as greater than 0.535 and less than 0.465, respectively, representing values outside the range of ideal symmetry of 0.5 ± three standard deviations.36 Pp and PSR, therefore represent measures that are capable of representing neuromotor recovery through the improvement in interlimb coordination of both kinematic and kinetic parameters. In addition, a theoretical framework exists for ways that these measures may guide clinical decision-making.
Portable technology-based assessment of walking specific motor control
In recent years, an alternative approach to collecting quantitative gait data with a traditional motion capture system has been developed, using activity monitor that use accelerometers (and in some cases gyroscopes and magnetometers) that are capable of measuring three dimensional (3D) accelerations to describe human movement patterns.37-39 Activity monitors permit the clinician/researcher to both count strides and also observe activity during pre-determined time spans.40-43 Cavanaugh et al44 used activity monitor data not only to count steps but also to capture the number of minutes of activity, number of activity bouts, variability of minute-to-minute activity, and randomness of minute-to-minute activity fluctuations. Additionally accelerometry systems have been utilized to quantify the “smoothness” of the gait pattern, a metric based on the harmonic ratio of the anterior-posterior accelerations that has been correlated to both the neural control of walking and the environmental demands.45 Preliminary studies demonstrate success at using portable accelerometer-based systems for quantifying basic spatiotemporal parameters.46-49
Portable methods of measuring human movement have the advantage of being considerably less expensive than traditional laboratory-based gait analysis equipment, allowing for testing beyond the confines of a laboratory setting. These devices are also small and unobtrusive allowing for less restricted movement, and may have the added benefit of measuring acceleration directly as opposed to requiring mathematical calculation based on position data.50 For example, gait assessment using accelerometers enables analysis of an approximation of the full body center of mass (CoM) anterior acceleration with less than 5% error.51 Such assessment tools can allow for collection of quantitative biomechanical data outside of the laboratory setting over a variety of terrains, yet represent the same constructs as data collected within the laboratory. The ability to perform assessments outside of the confines of a laboratory allows clinicians and researchers to assess skill acquisition, retention, and long-term carryover that result from therapeutic interventions in a variety of environments. Using this type of assessment, behavioral changes may be observed and evaluations can be made not only regarding an individual's ability to adapt during training but also regarding the ability to incorporate new skills into a real-world behavior. Furthermore, portable assessments will allow measurement of the multiple dimensions of community mobility such as varying terrain characteristics, transient ambient conditions, and obstacle avoidance that are critical to truly independent walking ability.52
Technology, therefore, may allow for the development of new measurement techniques based on the critical features of laboratory-based characteristics that appear to accurately measure neuromotor recovery. The goal of this measurement is not to reproduce inverse dynamics and provide all of the moments, powers, accelerations, and other data available in the laboratory but rather to capture, outside of the laboratory, the same critical constructs measured within the laboratory. For example, force production is one of the critical features available within a biomechanical laboratory, but at this point we are unaware of any valid and reliable mechanisms for reproducing 3-dimensional ground reaction forces (GRF) in the non-laboratory open environment. However, force production is mathematically equal to acceleration that has been normalized by mass (F=ma), and CoM acceleration curves are capable of yielding important biomechanical data. CoM acceleration can be obtained by any portable device capable of measuring linear acceleration. Most importantly, the construct of CoM directly parallels the laboratory-based measures and may potentially provide a valid surrogate, thus allowing clinical quantification of motor control deficits that may be directly addressed in therapeutic interventions. As an example of the utility of using CoM acceleration as part of assessment, symmetric propulsion, high Pp, and low Pp all yield distinctive CoM acceleration profiles (Figure 2). While peaks and areas under the curve are quantifiable variables, the shapes imply different motor control problems that are analogous to Pp and PSR. While the symmetric group (Figure 2a) demonstrates equal accelerations during each step (represented by the positive peaks), completely different patterns represent high and low Pp. Low Pp is characterized by a 2nd peak of decreased magnitude illustrating decreased acceleration/force occurring during paretic pre-swing (Figure 2b). However, the high Pp profile (Figure 2c) demonstrates only positive momentum (area under the acceleration curve) during the first half of the gait cycle and only negative momentum throughout paretic pre-swing and paretic swing phase. This persistent negative momentum throughout the swing phase indicates that the acceleration exceeding that associated with the non-paretic step comes at a cost of sacrificing positive momentum. Different treatment options may be indicated for these three profiles as described above.
Figure 2. COMa sorted by Pp.
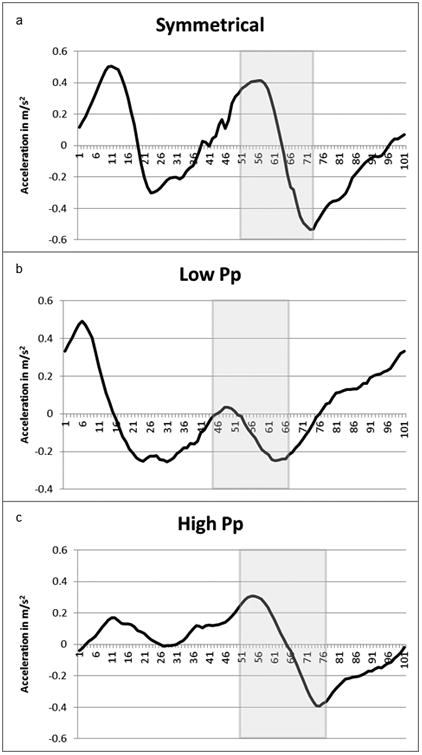
Sorting by Pp yields three distinctly different acceleration profiles, although the double support phase (shaded area) are similar in shape. The low Pp group (b) generates very little acceleration in the double support phase. However, the high Pp group (c) demonstrates only positive acceleration through the first half of the gait cycle, while remaining negative throughout late double support and swing. These profiles potentially indicate different treatments focusing on increasing propulsive force in the low Pp group while the high Pp group may benefit from swing initiation assistance to prevent prolonged negative acceleration.
The acceleration curves (Figure 2) illustrate a biomechanical element that is not targeted in either conventional physical therapy or contemporary task-specific walking interventions incorporating repetitive step training on a treadmill. For example, in locomotor training, a trainer may work to stabilize the pelvis, promote upright posture, assist with lateral weight shift, and assist pelvic rotation.53 Robotic gait have been more recently used for locomotor rehabilitation,54 but offer even fewer degrees of freedom at the pelvis/trunk as the torso is tightly constrained within the exoskeleton. Both of these interventions may be sub-optimal in providing the anterior translation of the CoM over the center of pressure, which is critical in the production of propulsive impulses responsible for moving the body forward during the latter half of stance phase.55 While much more work needs to be done to determine the utility of CoM acceleration measures in informing interventions and interpreting outcomes, these measures provide concrete examples of directions in which technology-based assessment tools may lead in the future.
The future of outcomes measurement
Scientists are currently using advanced techniques to more directly measure changes in neural function associated with rehabilitation interventions. Technology is being used to explore recovery, such as transcranial magnetic stimulation and motor evoked potentials to examine corticospinal tract changes after locomotor training trials,56 or fMRI to examine changes in cortical activity in response to a locomotor intervention. 57 Advanced MRI techniques utilizing diffusion tensor imaging are shedding light on the importance of descending white matter tracts from the brain and how they may be improved during neurorehabilitation.58 These measurements are being developed in order to ascertain the degree to which CNS structures adapt to injury and subsequent rehabilitation intervention and to discover the capacity for recovery that individuals have after neurologic injury.
Summary
Rehabilitation technology is progressing rapidly, improving our ability to provide interventions and capture necessary, quantifiable data to describe neuromotor recovery and to determine its role in improved performance. Such knowledge will help clinicians determine the most appropriate balance of recovery- versus compensatory-based intervention strategies depending on the capacity of the system to respond to therapy and ultimately optimize performance.
Measures of biomechanical movement patterns demonstrate the capability of describing neuromotor recovery and are already plausible for clinical translation. These biomechanical measures, and especially portable measures that can be used in the clinic and real-world environments, represent great potential in advancing measurement of locomotor rehabilitation outcomes in particular. One major advantage of these measurement tools is that their use would allow researchers and clinicians to more readily assess the relationship between restorative changes in the factors that contribute to walking performance and changes in the performance of the endpoint behavior. Those with neurologic injury demonstrate a myriad of gait deviations, combinations of which are unique to the individual, and improvements in some deviations will likely have a greater impact on walking performance than will improvements in others. Understanding the relationship between recovery of normal walking patterns and improved walking performance would enhance clinical decision-making regarding targeted gait intervention. This understanding, however, is contingent on the use of quantitative measurement tools that represent well-defined and ecologically valid metrics.
New applications for these advanced assessment tools are continuously being developed, but are presently underutilized. Specific to portable biomechanical measures, a 2008 review of quantification of walking patterns with accelerometry cited more than 50 articles addressing quantifiable and portable movement analyses,50 with the earliest mention of portable movement analysis dating back to 1936.59 Topics addressed in this review include not only segmental accelerations, but also studies of shock absorption, spatiotemporal gait parameters, control of stability, age-related changes in movement patterns, and relating quantifiable movement patterns to falls.50 However, a more recent review of accelerometry specific to stroke yielded only ten articles using portable technology to assess walking, and eight of them were specific to step counts.60
Technological advances in outcomes measurement, in and of itself however, will not advance neurorehabilitation, and having the capacity to measure a parameter is not sufficient justification for doing so. The necessity of locomotor rehabilitation measurement does not lie in replacing measurements obtained with rating scales or walking speed, but rather in developing additional and complimentary measurements that are capable of quantifying motor control mechanisms contributing to walking ability and that distinguish between recovery and compensation. Future locomotor measurement tools must be based on a theoretical framework guiding their use in order to clarify treatment effects and provide a rationale for the selection of therapeutic interventions.
Acknowledgments
Funding Acknowledgement: VA Career Development Award (Phase I): B7177
K12 HD055929 National Institutes of Health – National Center for Medical and Rehabilitation Research (NICHD) and National Institute for Neurological Disorders & Stroke
VA Merit Review grant B3983-R
VA Center of Excellence grant # F2182C (Brain Rehabilitation Research Center).
This material is the result of work supported with resources and the use of facilities at the Ralph H. Johnson VA Medical Center in Charleston, SC and the NF/SG Veterans Health System in Gainesville, FL. The contents do not represent the views of the Department of Veterans Affairs or the United States Government
Contributor Information
Mark G. Bowden, Ralph H. Johnson VA Medical Center, Charleston, SC. Department of Health Sciences and Research, Medical University of South Carolina, Charleston, SC.
Andrea L. Behrman, Department of Physical Therapy, University of Florida, Gainesville, FL. NF/SG Veterans Health System, Gainesville, FL.
Michelle Woodbury, Ralph H. Johnson VA Medical Center, Charleston, SC. Department of Health Sciences and Research, Medical University of South Carolina, Charleston, SC.
Chris M. Gregory, Ralph H. Johnson VA Medical Center, Charleston, SC. Department of Health Sciences and Research, Medical University of South Carolina, Charleston, SC.
Craig A. Velozo, Department of Occupational Therapy, University of Florida, Gainesville, FL. NF/SG Veterans Health System, Gainesville, FL.
Steven A. Kautz, Ralph H. Johnson VA Medical Center, Charleston, SC. Department of Health Sciences and Research, Medical University of South Carolina, Charleston, SC.
References
- 1.Kleim JA, Jones TA. Principles of experience-dependent neural plasticity: implications for rehabilitation after brain damage. Journal of speech, language, and hearing research : JSLHR. 2008 Feb;51(1):S225–239. doi: 10.1044/1092-4388(2008/018). [DOI] [PubMed] [Google Scholar]
- 2.Behrman AL, Bowden MG, Nair PM. Neuroplasticity After Spinal Cord Injury and Training: An Emerging Paradigm Shift in Rehabilitation and Walking Recovery. Physical therapy. 2006 Oct 1;86(10):1406–1425. doi: 10.2522/ptj.20050212. 2006. [DOI] [PubMed] [Google Scholar]
- 3.Mehrholz J, Kugler J, Pohl M. Locomotor training for walking after spinal cord injury. Spine. 2008 Oct 1;33(21):E768–777. doi: 10.1097/BRS.0b013e3181849747. [DOI] [PubMed] [Google Scholar]
- 4.Dickstein R. Rehabilitation of gait speed after stroke: a critical review of intervention approaches. Neurorehabilitation and neural repair. 2008 Nov-Dec;22(6):649–660. doi: 10.1177/1545968308315997. [DOI] [PubMed] [Google Scholar]
- 5.WHO International Classification of Functioning, Disability and Health: ICF. Geneva, Switzerland: World Health Organization; 2001. [Google Scholar]
- 6.Levin MF, Kleim JA, Wolf SL. What do motor “recovery” and “compensation” mean in patients following stroke? Neurorehabilitation and neural repair. 2009 May;23(4):313–319. doi: 10.1177/1545968308328727. [DOI] [PubMed] [Google Scholar]
- 7.Ramon y, Cajal S. Degeneration and Regeneration of the Nervous System. London: Oxford University Press; 1928. [Google Scholar]
- 8.Duncan P, Sullivan K, Behrman A, et al. Protocol for the Locomotor Experience Applied Post-stroke (LEAPS) trial: a randomized controlled trial. BMC Neurology. 2007;7(1):39. doi: 10.1186/1471-2377-7-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Dobkin B, Apple D, Barbeau H, et al. Weight-supported treadmill vs over-ground training for walking after acute incomplete SCI. Neurology. 2006 Feb 28;66(4):484–493. doi: 10.1212/01.wnl.0000202600.72018.39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Berg KO, Wood-Dauphinee SL, Williams JI, Maki B. Measuring balance in the elderly: validation of an instrument. Can J Public Health. 1992 Jul-Aug;83(2):S7–11. [PubMed] [Google Scholar]
- 11.Velozo C. Objective Measurement: The Influence of Item Response Theory on Research and Practice. In: Kielhofner G, editor. Research in Occupational Therapy: Methods of Inquiry for Enhancing Practice. Philadelphia, PA: F. A. Davis Company; 2006. pp. 177–200. [Google Scholar]
- 12.Wade DT. Measurement in neurological rehabilitation. Oxford: Oxford University Press; 1992. [PubMed] [Google Scholar]
- 13.Garcia-Araez N, Brosseau CL, Rodriguez P, Lipkowski J. Layer-by-layer PMIRRAS characterization of DMPC bilayers deposited on a Au111 electrode surface. Langmuir. 2006 Dec 5;22(25):10365–10371. doi: 10.1021/la061217v. [DOI] [PubMed] [Google Scholar]
- 14.Perry J, Garrett M, Gronley JK, Mulroy SJ. Classification of walking handicap in the stroke population. Stroke. 1995 Jun;26(6):982–989. doi: 10.1161/01.str.26.6.982. [DOI] [PubMed] [Google Scholar]
- 15.Schmid A, Duncan PW, Studenski S, et al. Improvements in speed-based gait classifications are meaningful. Stroke; a journal of cerebral circulation. 2007 Jul;38(7):2096–2100. doi: 10.1161/STROKEAHA.106.475921. [DOI] [PubMed] [Google Scholar]
- 16.Richards CL, Malouin F, Dumas F, Tardiff D. Gait velocity as an outcome measure of locomotor recovery after stroke. In: Oatis C, editor. Gait analysis: theory and applications. St. Louis: Mosby; 1995. pp. 355–364. [Google Scholar]
- 17.Studenski S, Wallace D, Chandler J, et al. Gait speed as a clinical vital sign in the care of older adults. J Am Geriatr Soc. 2002 [Google Scholar]
- 18.Olney SJ, Nymark J, Brouwer B, et al. A randomized controlled trial of supervised versus unsupervised exercise programs for ambulatory stroke survivors. Stroke; a journal of cerebral circulation. 2006 Feb;37(2):476–481. doi: 10.1161/01.STR.0000199061.85897.b7. [DOI] [PubMed] [Google Scholar]
- 19.Teixeira-Salmela LF, Olney SJ, Nadeau S, Brouwer B. Muscle strengthening and physical conditioning to reduce impairment and disability in chronic stroke survivors. Archives of physical medicine and rehabilitation. 1999 Oct;80(10):1211–1218. doi: 10.1016/s0003-9993(99)90018-7. [DOI] [PubMed] [Google Scholar]
- 20.Teixeira-Salmela LF, Nadeau S, McBride I, Olney SJ. Effects of muscle strengthening and physical conditioning training on temporal, kinematic and kinetic variables during gait in chronic stroke survivors. J Rehabil Med. 2001;33(2):53–60. doi: 10.1080/165019701750098867. [DOI] [PubMed] [Google Scholar]
- 21.Burridge JH, Taylor PN, Hagan SA, Wood DE, Swain ID. The effects of common peroneal stimulation on the effort and speed of walking: a randomized controlled trial with chronic hemiplegic patients. Clinical rehabilitation. 1997 Aug;11(3):201–210. doi: 10.1177/026921559701100303. [DOI] [PubMed] [Google Scholar]
- 22.Macko RF, Ivey FM, Forrester LW, et al. Treadmill exercise rehabilitation improves ambulatory function and cardiovascular fitness in patients with chronic stroke: a randomized, controlled trial. Stroke; a journal of cerebral circulation. 2005 Oct;36(10):2206–2211. doi: 10.1161/01.STR.0000181076.91805.89. [DOI] [PubMed] [Google Scholar]
- 23.Ada L, Dean CM, Hall JM, Bampton J, Crompton S. A treadmill and overground walking program improves walking in persons residing in the community after stroke: a placebo-controlled, randomized trial. Archives of physical medicine and rehabilitation. 2003 Oct;84(10):1486–1491. doi: 10.1016/s0003-9993(03)00349-6. [DOI] [PubMed] [Google Scholar]
- 24.Sullivan KJ, Knowlton BJ, Dobkin BH. Step training with body weight support: effect of treadmill speed and practice paradigms on poststroke locomotor recovery. Archives of Physical Medicine and Rehabilitation. 2002 May;83(5):683–691. doi: 10.1053/apmr.2002.32488. [DOI] [PubMed] [Google Scholar]
- 25.Sullivan KJ, Brown DA, Klassen T, et al. Effects of task-specific locomotor and strength training in adults who were ambulatory after stroke: results of the STEPS randomized clinical trial. Physical therapy. 2007 Dec;87(12):1580–1602. doi: 10.2522/ptj.20060310. [DOI] [PubMed] [Google Scholar]
- 26.Yavuzer G, Oken O, Elhan A, Stam HJ. Repeatability of lower limb three-dimensional kinematics in patients with stroke. Gait & posture. 2008 Jan;27(1):31–35. doi: 10.1016/j.gaitpost.2006.12.016. [DOI] [PubMed] [Google Scholar]
- 27.Teixeira-Salmela LF, Olney SJ, Nadeau S, Brouwer B. Muscle strengthening and physical conditioning to reduce impairment and disability in chronic stroke survivors. Arch Phys Med Rehabil. 1999 Oct;80(10):1211–1218. doi: 10.1016/s0003-9993(99)90018-7. [DOI] [PubMed] [Google Scholar]
- 28.Parvataneni K, Olney SJ, Brouwer B. Changes in muscle group work associated with changes in gait speed of persons with stroke. Clin Biomech (Bristol, Avon) 2007 Aug;22(7):813–820. doi: 10.1016/j.clinbiomech.2007.03.006. [DOI] [PubMed] [Google Scholar]
- 29.Gregory CM, Bowden MG, Jayaraman A, et al. Resistance training and locomotor recovery after incomplete spinal cord injury: a case series. Spinal cord : the official journal of the International Medical Society of Paraplegia. 2007 Jul;45(7):522–530. doi: 10.1038/sj.sc.3102002. [DOI] [PubMed] [Google Scholar]
- 30.Sullivan K, Klassen T, Mulroy S. Combined task-specific training and strengthening effects on locomotor recovery post-stroke: a case study. J Neurol Phys Ther. 2006 Sep;30(3):130–141. doi: 10.1097/01.npt.0000281950.86311.82. [DOI] [PubMed] [Google Scholar]
- 31.McCain KJ, Pollo FE, Baum BS, Coleman SC, Baker S, Smith PS. Locomotor treadmill training with partial body-weight support before overground gait in adults with acute stroke: a pilot study. Arch Phys Med Rehabil. 2008 Apr;89(4):684–691. doi: 10.1016/j.apmr.2007.09.050. [DOI] [PubMed] [Google Scholar]
- 32.Balasubramanian CK, Neptune RR, Kautz SA. Foot placement in a body reference frame during walking and its relationship to hemiparetic walking performance. Clinical biomechanics. 2010 Jun;25(5):483–490. doi: 10.1016/j.clinbiomech.2010.02.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Balasubramanian CK, Bowden MG, Neptune RR, Kautz SA. Relationship between step length asymmetry and walking performance in subjects with chronic hemiparesis. Arch Phys Med Rehabil. 2007 Jan;88(1):43–49. doi: 10.1016/j.apmr.2006.10.004. [DOI] [PubMed] [Google Scholar]
- 34.Bowden MG, Balasubramanian CK, Neptune RR, Kautz SA. Anterior-posterior ground reaction forces as a measure of paretic leg contribution in hemiparetic walking. Stroke. 2006 Mar;37(3):872–876. doi: 10.1161/01.STR.0000204063.75779.8d. [DOI] [PubMed] [Google Scholar]
- 35.Turns LJ, Neptune RR, Kautz SA. Relationships between muscle activity and anteroposterior ground reaction forces in hemiparetic walking. Arch Phys Med Rehabil. 2007 Sep;88(9):1127–1135. doi: 10.1016/j.apmr.2007.05.027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Kautz SA, Bowden MG, Clark DJ, Neptune RR. Comparison of motor control deficits during treadmill and overground walking poststroke. Neurorehabil Neural Repair. doi: 10.1177/1545968311407515. IN PRESS. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hodt-Billington C, Helbostad JL, Moe-Nilssen R. Should trunk movement or footfall parameters quantify gait asymmetry in chronic stroke patients? Gait & posture. 2008 May;27(4):552–558. doi: 10.1016/j.gaitpost.2007.07.015. [DOI] [PubMed] [Google Scholar]
- 38.Kavanagh JJ, Morrison S, James DA, Barrett R. Reliability of segmental accelerations measured using a new wireless gait analysis system. Journal of biomechanics. 2006;39(15):2863–2872. doi: 10.1016/j.jbiomech.2005.09.012. [DOI] [PubMed] [Google Scholar]
- 39.Saremi K, Marehbian J, Yan X, et al. Reliability and validity of bilateral thigh and foot accelerometry measures of walking in healthy and hemiparetic subjects. Neurorehabilitation and neural repair. 2006 Jun;20(2):297–305. doi: 10.1177/1545968306287171. [DOI] [PubMed] [Google Scholar]
- 40.Coleman KL, Smith DG, Boone DA, Joseph AW, del Aguila MA. Step activity monitor: long-term, continuous recording of ambulatory function. J Rehabil Res Dev. 1999 Jan;36(1):8–18. [PubMed] [Google Scholar]
- 41.Shepherd EF, Toloza E, McClung CD, Schmalzried TP. Step activity monitor: increased accuracy in quantifying ambulatory activity. J Orthop Res. 1999 Sep;17(5):703–708. doi: 10.1002/jor.1100170512. [DOI] [PubMed] [Google Scholar]
- 42.Macko RF, Haeuber E, Shaughnessy M, et al. Microprocessor-based ambulatory activity monitoring in stroke patients. Med Sci Sports Exerc. 2002 Mar;34(3):394–399. doi: 10.1097/00005768-200203000-00002. [DOI] [PubMed] [Google Scholar]
- 43.Bowden MG, Behrman AL. Step Activity Monitor: accuracy and test-retest reliability in persons with incomplete spinal cord injury. Journal of rehabilitation research and development. 2007;44(3):355–362. doi: 10.1682/jrrd.2006.03.0033. [DOI] [PubMed] [Google Scholar]
- 44.Cavanaugh JT, Coleman KL, Gaines JM, Laing L, Morey MC. Using step activity monitoring to characterize ambulatory activity in community-dwelling older adults. Journal of the American Geriatrics Society. 2007 Jan;55(1):120–124. doi: 10.1111/j.1532-5415.2006.00997.x. [DOI] [PubMed] [Google Scholar]
- 45.Brach JS, McGurl D, Wert D, et al. Validation of a Measure of Smoothness of Walking. The journals of gerontology Series A, Biological sciences and medical sciences. 2010 Oct 5; doi: 10.1093/gerona/glq170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Houdijk H, Appelman FM, Van Velzen JM, Van der Woude LH, Van Bennekom CA. Validity of DynaPort GaitMonitor for assessment of spatiotemporal parameters in amputee gait. Journal of rehabilitation research and development. 2008;45(9):1335–1342. [PubMed] [Google Scholar]
- 47.Maffiuletti NA, Gorelick M, Kramers-de Quervain I, et al. Concurrent validity and intrasession reliability of the IDEEA accelerometry system for the quantification of spatiotemporal gait parameters. Gait & posture. 2008 Jan;27(1):160–163. doi: 10.1016/j.gaitpost.2007.01.003. [DOI] [PubMed] [Google Scholar]
- 48.Tura A, Raggi M, Rocchi L, Cutti AG, Chiari L. Gait symmetry and regularity in transfemoral amputees assessed by trunk accelerations. Journal of neuroengineering and rehabilitation. 2010;7:4. doi: 10.1186/1743-0003-7-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Hartmann A, Murer K, de Bie RA, de Bruin ED. Reproducibility of spatio-temporal gait parameters under different conditions in older adults using a trunk tri-axial accelerometer system. Gait & posture. 2009 Oct;30(3):351–355. doi: 10.1016/j.gaitpost.2009.06.008. [DOI] [PubMed] [Google Scholar]
- 50.Kavanagh JJ, Menz HB. Accelerometry: a technique for quantifying movement patterns during walking. Gait Posture. 2008 Jul;28(1):1–15. doi: 10.1016/j.gaitpost.2007.10.010. [DOI] [PubMed] [Google Scholar]
- 51.Betker AL, Szturm T, Moussavi Z. Center of mass approximation during walking as a function of trunk and swing leg acceleration. Conf Proc IEEE Eng Med Biol Soc. 2006;1:3435–3438. doi: 10.1109/IEMBS.2006.259881. [DOI] [PubMed] [Google Scholar]
- 52.Patla A, Shumway-Cook A. Dimensions of mobility: defining the complexity and difficulty associated with community mobility. Journal of Aging and Physical Activity. 1999;7:7–19. [Google Scholar]
- 53.Behrman AL, Lawless-Dixon AR, Davis SB, et al. Locomotor training progression and outcomes after incomplete spinal cord injury. Phys Ther. 2005 Dec;85(12):1356–1371. [PubMed] [Google Scholar]
- 54.Hidler J, Nichols D, Pelliccio M, et al. Multicenter randomized clinical trial evaluating the effectiveness of the Lokomat in subacute stroke. Neurorehabil Neural Repair. 2009 Jan;23(1):5–13. doi: 10.1177/1545968308326632. [DOI] [PubMed] [Google Scholar]
- 55.Perry J. Gait Analysis: Normal and Pathological Function. Thorofare, NJ: Slack, Inc.; 1992. [Google Scholar]
- 56.Thomas SL, Gorassini MA. Increases in corticospinal tract function by treadmill training after incomplete spinal cord injury. J Neurophysiol. 2005 Oct;94(4):2844–2855. doi: 10.1152/jn.00532.2005. [DOI] [PubMed] [Google Scholar]
- 57.Dobkin BH, Firestine A, West M, Saremi K, Woods R. Ankle dorsiflexion as an fMRI paradigm to assay motor control for walking during rehabilitation. Neuroimage. 2004 Sep;23(1):370–381. doi: 10.1016/j.neuroimage.2004.06.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Sterr A, Shen S, Szameitat AJ, Herron KA. The role of corticospinal tract damage in chronic motor recovery and neurorehabilitation: a pilot study. Neurorehabilitation and neural repair. 2010 Jun;24(5):413–419. doi: 10.1177/1545968309348310. [DOI] [PubMed] [Google Scholar]
- 59.Liberson WT. Une nouvelle application du quartz piezoelectrique: piezoelectrographie de la marche et des mouvements volontaires. Le Travail Humain. 1936;4:1–7. [Google Scholar]
- 60.Gebruers N, Vanroy C, Truijen S, Engelborghs S, De Deyn PP. Monitoring of physical activity after stroke: a systematic review of accelerometry-based measures. Archives of Physical Medicine and Rehabilitation. 2010 Feb;91(2):288–297. doi: 10.1016/j.apmr.2009.10.025. [DOI] [PubMed] [Google Scholar]