

Abstract
Background
Exercise-based interventions have shown promise in slowing cognitive decline, however there is limited evidence for scalability. Our previous research has linked a novel visuospatial memory exercise intervention, incorporating patterned walking or square-stepping exercise (SSE) with significant improvements in executive function and memory among older adults with normal cognition as well as those with subjective cognitive complaints (SCC) and mild cognitive impairment (MCI). The aim of the current study was to determine the feasibility and utility of the HealtheBrain smartphone app to deliver SSE outside the laboratory among older adults with and without cognitive impairment.
Methods
Previous healthy research subjects with and without SCC or MCI, who had previous exposure to SSE, and who owned or had access to an iPhone of iPad, were recruited to download the HealtheBrain app and use it up to 3 weeks. There were no restrictions on the number of times subjects could use the app. A 15-question survey was developed to assess feasibility and utility of the HealtheBrain app and completed online following the brief exposure period.
Results
Of 135 people who were identified, 95 were contacted between September 2014 to August 2015, 27 downloaded the HealtheBrain app on their iPhone or iPad from the App Store and 19 completed the questionnaire. Subjects (n=19) were an average age of 68.3±5.4; 74% female and had 15.5±2.8 years of education (84% post-secondary education), a mean Mini Mental State examination score of 29.1 (SD 1.2) out of 30 and Montreal Cognitive Assessment score of 26.3 (SD 1.9) out of 30. Subjects used the HealtheBrain app 1-7 days per week, mostly at home. Of possible stages of progression, subjects mainly used the stage 1 and 2 beginner patterns. Subjects reported perceived and technical challenges registering horizontal step patterns associated with stage 2 and greater progression. Sixty percent found the app was easy to use or similar to what they experienced with SSE in the laboratory setting. Most said they would continue to use the HealtheBrain app and would recommend it to friends and family.
Conclusions
The HealtheBrain app was feasible in providing SSE to older adults with the appropriate smartphone device outside the laboratory setting. Challenges were identified with perceived capture of higher levels of SSE stages that used horizontal step patterns. This as well as technical issues with horizontal step patterns will be addressed by newer GPS technology in current smartphone devices. Most subjects stated they would continue to use the HealtheBrain app and refer to their friends and family. We believe that our findings in a representative cohort support the HealtheBrain app as a scalable intervention to promote cognitive health in older adults.
Keywords: Mobile application, older adults, cognition, exercise intervention
Introduction
Global population aging has resulted in increased incidence of chronic disease including dementia. It has been estimated that dementia will cost Canada $16.6 billion per year by 2031 in direct and indirect costs (1). There are currently no effective pharmacological treatments available for prevention or treatment of cognitive decline or dementia (2,3). Additionally, while showing some short term benefits, exercise intervention trials have not demonstrated long term adoption or scalability (4,5).
Higher levels of physical activity are associated with: higher cognitive function (6), higher hippocampal volume (7), more white and grey matter volume (8) and higher levels of neurobiological health markers (9) compared to those who are sedentary. Evidence from cognitive training studies, such as computer-based and exergaming training programs, demonstrate that these interventions can maintain or improve cognitive functioning (9-12), may attenuate volume loss within the prefrontal cortex (13); and may provide cognitive vitality with increasing age (14). Therefore, combining physical and cognitive training may provide additive benefits to elicit an efficacious strategy to combat cognitive decline (15,16).
Square-stepping exercise (SSE) can be described as a visuospatial working memory task with a cued stepping response, also known as mind-motor exercise. An instructor demonstrates a stepping pattern and subjects must memorize and repeat the stepping patterns across a gridded mat (Figure 1). There are more than 200 patterns that progress in difficulty, which operate to challenge visuospatial executive function, memory skills and balance. We and others have previously shown that SSE improved balance (17,18), fitness (19), gait (20) and strength in healthy older adults (18,21). We have also observed that SSE improved global cognitive functioning, and specifically memory and executive functioning (22,23).
Figure 1.
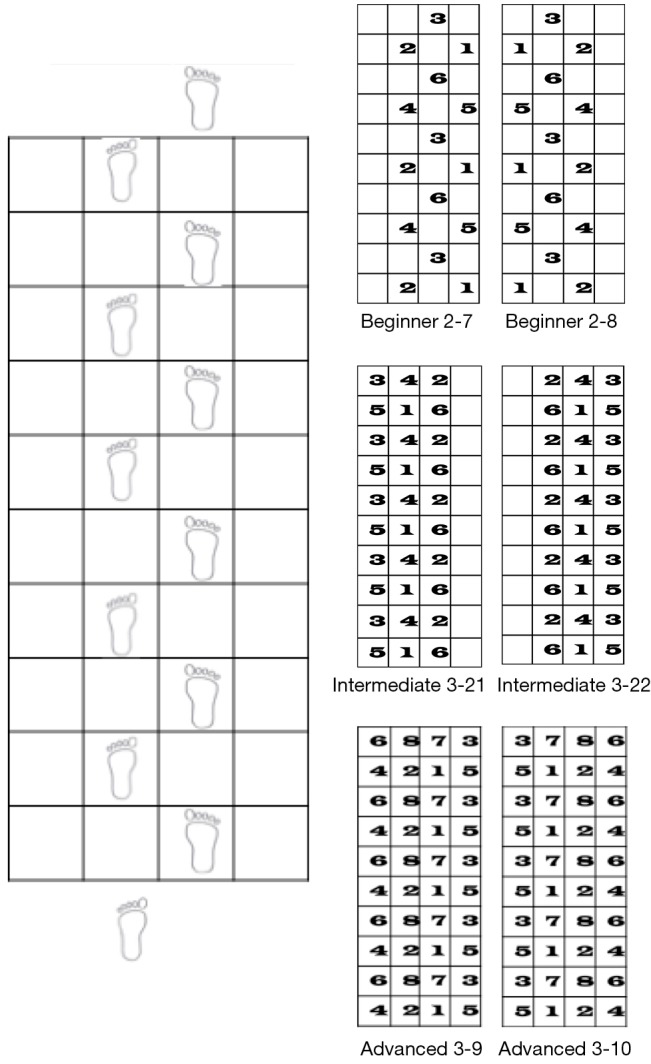
Schematic of Square-stepping exercise (SSE) program, where participants in groups, complete walking or stepping patterns across a gridded mat as demonstrated by an instructor. Original Publisher is Biomed Central. Reference: Gregory MA, Gill DP, Shellington EM, et al. Group-based exercise and cognitive-physical training in older adults with self-reported cognitive complaints: The Multiple-Modality, Mind-Motor (M4) study protocol. BMC Geriatr 2016;16:17.
We conducted a search of physical activity interventions available on smartphone platforms and showed that few apps were based on or provided evidence-based interventions (24); nor did they include end user input to the app target market. Similarly, few current apps linking cognition and exercise are evidence-based. Hence, this study was designed to provide input from the end users regarding the feasibility and utility of the HealtheBrain evidence-based app.
Methods
Recruitment
Community-dwelling older adults aged 55 years and older with or without mild cognitive impairment (MCI) who had participated in previous exercise and brain health studies in our laboratory with and without SSE exposure, were recruited for participation. Subjects were contacted from September 2014 to August 2015, completing the online questionnaire provided informed consent. Subjects were screened for access to an iPod touch 4+, iPhone 3GS+ or iPad 2+ due to the availability of the free HealtheBrain app on the Apple App Store.
Protocol
Step-by-step instructions were given on how to download the HealtheBrain app onto their device over the phone. Subjects were then asked to use the HealtheBrain app over the next 2–3 weeks; they were recommended to use the app at least 3 times per week after which they would complete a questionnaire on their perceptions of using the app. Subjects were advised to contact the study personnel if they had any questions, concerns or technical issues when using the app during the 3-week trial period.
Questionnaire
A 15-item questionnaire (combination of Likert, multiple choice and open text) was developed to obtain information relating to the feasibility and utility of the app (12 items).
The questionnaire was provided as an online survey (http://fluidsurveys.com/s/HealtheBrain/), which was sent by email to the subjects 3 weeks after the download. There was no identifying information on the questionnaire.
Once a subject downloaded and opened the app, a tutorial appeared on the screen with a series of images to guide use (Figure 2). After proceeding through tutorial screens, a subject was then automatically directed to a ‘home’ screen. At this point subjects were required to calibrate their usual step length by taking 10 steps in the calibration feature. Following calibration, the user started the program by selecting ‘Play’. At this point, only stage 1 of the 35 progressive SSE stages was unlocked, within each stage there are 4–8 patterns. Once a subject achieved at least 50% accuracy on 80% of patterns within the stage, the next stage would be unlocked. This ensured the subjects progressed through the patterns sequentially and had adequately progressed their SSE goal. To “reward” progression to the next stage of difficulty, a subject earns a new item or tool associated with the stage, which was added to a virtual garden on their app. This reward feature was aimed at providing a tangible marker of SSE progression, making the experience enjoyable or even competitive when shared with other users. With progress through the app, more items were added to the garden.
Figure 2.
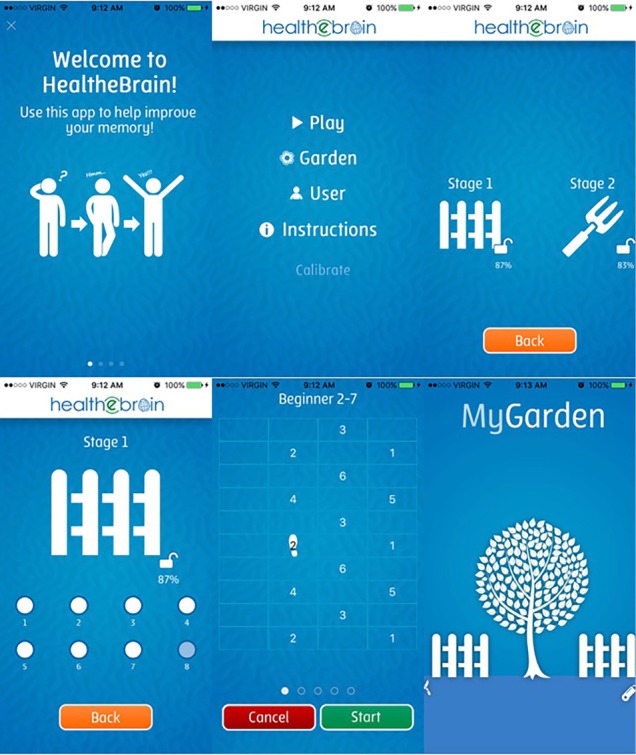
Screenshots of HealtheBrain smartphone application. Top (left to right): example of one of the 4 tutorial pages that appear at initial start-up; home page; stages of Square-stepping patterns that can be unlocked with features to add to their garden. Bottom (left to right): patterns within a stage; a Square-stepping pattern demonstrated on screen of phone for user to repeat, the ‘reward’ garden which earns tools as a subject progresses through HealtheBrain.
Within each session, the user was given the option of completing a standard ‘warm-up’ pattern. The “warm up” screen demonstrated a simple walking pattern, which the subject would be challenged to memorize and repeat. Once the subject had memorized the pattern, they would click ‘Start’, which would cause the pattern to disappear and indicated the device was ready to record the steps the subjects walked, by holding the device parallel to the floor, ideally at waist level in their dominant hand. If an iPad was being used, both hands were used to hold the device. After completing the warm-up pattern, the selected pattern would be shown on the screen in the same manner. A subject would need to memorize the pattern, press ‘Start’ and complete the pattern by walking whilst holding the device parallel to the floor. When the subjects were done walking the pattern, they indicated by pressing ‘Stop’ or 30 s had passed; the HealtheBrain app displayed the percentage accuracy based on an algorithm linked to forward, backward and lateral directions specific to that SSE pattern. The subject then repeated the SSE patterns selected within a specific stage until at least 50% accuracy was achieved in at least 80% of the stage patterns; at which time the subject was directed to the next stage of difficulty, or could select to repeat the current stage again.
The University of Western Ontario Health Sciences Research Ethics Board approved (No. 18858) this study and it is in accordance with the Helsinki Declaration as revised in 2013.
Analysis
Microsoft excel was used to input data and SPSS was used to analyze data from the questionnaire. Text responses were analyzed verbatim for themes by 2 independent researchers.
Results
Subject characteristics and feasibility
One hundred and thirty-five people were identified as potential subjects from previous exercise studies in our laboratory, of which 95 were contacted by research staff. Fifty responded they did not own a suitable smartphone device, 7 were not available, and 11 had a device but declined participation. Twenty-seven subjects had an iPhone or iPad device, consented to participate and downloaded the HealtheBrain app; however, 8 experienced technical issues with their device related to obtaining an Apple account, forgotten passwords, and understanding how to use and access the App Store so did not complete the questionnaire. Nineteen subjects successfully downloaded the HealtheBrain app and completed the survey, of which four had previous exposure to SSE and 12 required assistance downloading HealtheBrain from study personnel or family members. The 19 subjects ranged in age from 59–76 years of age, were 74% female, highly educated with an average of 15.5 (SD 2.8) years of education and Mini-Mental State examination score of 29.1 (SD 1.2) out of 30 and Montreal Cognitive Assessment score of 26.3 (SD 1.9) out of 30; and 9 said their memory was worse than 5 years ago (Table 1).
Table 1. Demographic information of subjects who completed questionnaire.
| Characteristics | Data (n=19) |
|---|---|
| Age (years) | 68.3±5.4 |
| Female sex [%] | 14 [74] |
| White race [%] | 18 [95] |
| Total years of education | 15.5±2.8 |
| MoCA score† | 26.3±1.9 |
| MMSE score‡ | 29.1±1.2 |
| Memory worse (ref to 5 years ago)§ [%] | 9 [47] |
†, Montreal cognitive assessment, scored out of 30; ‡, mini-mental state examination, scored out of 30; §, participants were asked to rate their memory on a scale of 5 (from much better to much worse).
Subjects tended to use the HealtheBrain app 1–3 times per week primarily at home; 6 responding they used it every day (Table 2). Eighty-four percent responded they felt the flow of the HealtheBrain app was sensible. Comments regarding utility included concern the app did not capture stepping variability (horizontal steps) within the patterns (stages) of SSE. Specifically, “the only difficulty was when I was doing more complicated steps. I found that it would not record the steps… Otherwise, worked well.”; “…so far I like it. I find it challenging”, “I think this is a great idea for inactive people, elderly individuals or someone participating in a rehab program…” but cautioned that “It seems likely many potential participants need more social interaction and therefore their level of participation may be increased by more human contact.” and “… for me it is easier to commit to class participation because it is scheduled. It is easier to just skip the smartphone application for a few days”.
Table 2. Responses obtained from the HealtheBrain app questionnaire from previous research subjects (n=19).
| Question | Multiple choice answers | No. of responses |
|---|---|---|
| 1. How many weeks have you been using the smartphone application | Less than 2 weeks | 9 |
| 2 weeks | 2 | |
| 3 weeks | 5 | |
| More than 3 weeks | 3 | |
| 2. Approximately how often did you use the HealtheBrain smartphone application each week? | Never | 2 |
| 1–3 times | 11 | |
| 4–6 times | 0 | |
| Every day | 4 | |
| More than once a day | 2 | |
| 3. Where do you most often use the HealtheBrain smartphone application? | At home | 18 |
| At work | 0 | |
| Outdoors (park, sidewalk, etc.) | 1 | |
| Other | 0 | |
| 4. Did you find the HealtheBrain smartphone application tutorial helpful? | Yes | 12 |
| No | 6 | |
| (If No) Please explain why the tutorial was not helpful. | (Open ended) | |
| 5. Did the flow of the HealtheBrain smartphone application make sense? | Yes | 16 |
| No | 3 | |
| (If No) What was problematic about the flow? | (Open ended) | |
| 6. Did you find the HealtheBrain smartphone application instructions to be clear? | Yes | 10 |
| No | 8 | |
| (If No) Please explain why the instructions were not clear. | (Open ended) | |
| 7. Will you continue to use the HealtheBrain smartphone application in the future? | Yes | 9 |
| No | 8 |
Subjects expressed the need to repeat the tutorial stating they “had a hard time figuring out what to do and holding device stable…”. These comments echoed statements made to the research staff over the telephone during the study where technical issues were the main points for contact and seemed to concern the perception the app did not detect step movement during horizontal steps and may not have allowed progression to the next stage as quickly as subjects would have anticipated.
Overall 63% of subjects were very satisfied, satisfied or neutral about the app providing a positive experience to support cognitive function improvement. Over half claimed they would continue to use the HealtheBrain app while also recommending it to family and friends. Fifty-six percent of subjects spontaneously reported that they thought the app could improve balance.
Discussion
With a growing number of older adults at risk for cognitive impairment, there is an urgent need for evidence-based interventions that are scalable. We have previously shown that visuospatial exercise training using SSE improves global and executive cognitive function and memory (25). We suggest that the HealtheBrain app could provide the opportunity to extend the reach of our research and scale up where and when subjects choose to participate. This study has shown the feasibility and utility of the HealtheBrain app in older adults concerned about their cognitive health. Specifically, our results suggest that the HealtheBrain app was accessible for those with an iPhone or iPad device, 27 of 34 participants with such devices. If we consider that 11 could not participate because they had an Android smartphone, of the potential 95 subjects, a total of 35.8% owned a smartphone, which is higher than the estimated national average for older adults of 27.4% (26). Given the boom in those over the age of 55 with a smartphone, providing the HealtheBrain app on the iOS and Android platforms could reach a significant proportion of the at-risk population.
The population that we recruited were highly educated and therefore we should view our findings with caution when extending the results to the general older population.
Subjects used the HealtheBrain app for only 3 weeks and ranged from 1–7 uses per week hence the exposure was variable compared to our laboratory based studies where exposure was 3 times per week for at least 12 weeks. Further, use of the HealtheBrain app differed from SSE delivered in the laboratory setting where it was group-based and benefitted from the social support of peers and a trainer—not only supporting performance but compliance and adherence to the SSE protocol. Nevertheless, over half of subjects of the HealtheBrain app claimed they would continue to use the app and refer it to their friends and family. Indeed, given that our users had previous exposure to the group based SSE program, the app could provide an ongoing “booster” support to similar programs once they have been completed while also providing those without access to group programs, the benefits of SSE. Some concerns were raised by subjects who felt the app did not capture their movements at higher stages of SSE. While ongoing enhancements to the GPS technology will alleviate technical concerns, we suggest that more tutorial repetition could also alleviate perceived concerns and enhance the app experience. Further, our experience also suggests that individual calibration is very important prior to using the app at any SSE stage and that with more use, the step movements are more accurately captured by the device.
There are some limitations with this report that require discussion. The population identified included previous exercise subjects from our laboratory, were mostly female, white and well educated potentially influencing generalizability. However, subjects did have concerns about their cognitive health and memory which is the target group we are considering. While restricting access to only those with an iPhone or iPad on the iOS platform, expansion to the Android platform and the growing number of seniors with smartphones should increase the exposure of potential users to the HealtheBrain app. While we restricted the exposure to only 3 weeks, we did find most claimed they would continue to use the app further and the intent was not to show objective changes in cognitive function but rather the user experience with the HealtheBrain app.
Acknowledgements
We would like to acknowledge Dr. Melanie Stuckey and Heather Morton for assisting our app developers, Mark Wilson and Linus Hiew, at IC Solutions.
T Felfeli was funded by Technology Evaluation in the Elderly Network to work on this project. R Shigematsu developed Square-stepping exercise program, which HealtheBrain is designed from.
Ethical Statement: The University of Western Ontario Health Sciences Research Ethics Board approved (No. 18858) this study and it is in accordance with the Helsinki Declaration as revised in 2013.
Footnotes
Conflicts of Interest: The authors have no conflicts of interest to declare.
References
- 1.Alzheimer Society of Canada. A new way of looking at the impact of dementia in Canada. Available online: http://www.alzheimer.ca/en/Get-involved/Raise-your-voice/A-new-way-of-looking-at-dementia
- 2.Tan CC, Yu JT, Wang HF, et al. Efficacy and Safety of Donepezil, Galantamine, Rivastigmine, and Memantine for the Treatment of Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J Alzheimers Dis 2014;41:615-31. [DOI] [PubMed] [Google Scholar]
- 3.Wang J, Yu JT, Wang HF, et al. Pharmacological treatment of neuropsychiatric symptoms in Alzheimer’s disease: a systematic review and meta-analysis. J Neurol Neurosurg Psychiatry 2015;86:101-9. 10.1136/jnnp-2014-308112 [DOI] [PubMed] [Google Scholar]
- 4.Colcombe SJ, Kramer AF, Erickson KI, et al. Cardiovascular fitness, cortical plasticity, and aging. Proc Natl Acad Sci 2004;101:3316-21. 10.1073/pnas.0400266101 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Erickson KI, Voss MW, Prakash RS, et al. Exercise training increases size of hippocampus and improves memory. Proc Natl Acad Sci U S A 2011;108:3017-22. 10.1073/pnas.1015950108 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Colcombe S, Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci 2003;14:125-30. 10.1111/1467-9280.t01-1-01430 [DOI] [PubMed] [Google Scholar]
- 7.Erickson KI, Prakash RS, Voss MW, et al. Brain-derived neurotrophic factor is associated with age-related decline in hippocampal volume. J Neurosci 2010;30:5368-75. 10.1523/JNEUROSCI.6251-09.2010 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Erickson KI, Raji C, Lopez O, et al. Physical activity predicts gray matter volume in late adulthood: The Cardiovascular Health Study. Neurology 2010;75:1415-22. 10.1212/WNL.0b013e3181f88359 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hanna-Pladdy B, MacKay A. The relation between instrumental musical activity and cognitive aging. Neuropsychology 2011;25:378-86. 10.1037/a0021895 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Plassman BL, Langa KM, Fisher GG, et al. Prevalence of dementia in the United States: The aging, demographics, and memory study. Neuroepidemiology 2007;29:125-32. 10.1159/000109998 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Wang HX, Jin Y, Hendrie HC, et al. Late Life Leisure Activities and Risk of Cognitive Decline. Journals Gerontol Ser A Biol Sci Med Sci 2013;68:205-13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Kelly ME, Loughrey D, Lawlor BA, et al. The impact of cognitive training and mental stimulation on cognitive and everyday functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res Rev 2014;15:28-43. 10.1016/j.arr.2014.02.004 [DOI] [PubMed] [Google Scholar]
- 13.Sluming V, Barrick T, Howard M, et al. Voxel-Based Morphometry Reveals Increased Gray Matter Density in Broca’s Area in Male Symphony Orchestra Musicians. Neuroimage 2002;17:1613-22. 10.1006/nimg.2002.1288 [DOI] [PubMed] [Google Scholar]
- 14.Kramer AF, Bherer L, Colcombe SJ, et al. Environmental Influences on Cognitive and Brain Plasticity During Aging. Journals Gerontol Ser A Biol Sci Med Sci 2004;59:M940-57. [DOI] [PubMed] [Google Scholar]
- 15.Eggenberger P, Schumacher V, Angst M, et al. Does multicomponent physical exercise with simultaneous cognitive training boost cognitive performance in older adults? A 6-month randomized controlled trial with a 1-year follow-up. Clin Interv Aging 2015;10:1335-49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Wayne PM, Walsh JN, Taylor-Piliae RE, et al. The Impact of Tai Chi on Cognitive Performance in Older Adults: A Systematic Review and Meta-Analysis. J Am Geriatr Soc 2014;62:25-39. 10.1111/jgs.12611 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Shigematsu R, Okura T, Nakagaichi M, et al. Square-Stepping Exercise and Fall Risk Factors in Controlled Trial. J Gerontol A Biol Sci Med Sci 2008;63:76-82. 10.1093/gerona/63.1.76 [DOI] [PubMed] [Google Scholar]
- 18.Teixeira CV, Gobbi S, Pereira JR, et al. Effect of square-stepping exercise and basic exercises on functional fitness of older adults. Geriatr Gerontol Int 2013;13:842-8. 10.1111/ggi.12011 [DOI] [PubMed] [Google Scholar]
- 19.Boa Sorte Silva NC, Gregory MA, Gill DP, et al. Multiple-modality exercise and mind-motor training to improve cardiovascular health and fitness in older adults at risk for cognitive impairment: A randomized controlled trial. Arch Gerontol Geriatr 2017;68:149-60. 10.1016/j.archger.2016.10.009 [DOI] [PubMed] [Google Scholar]
- 20.Gregory MA, Gill DP, Zou G, et al. Group-based exercise combined with dual-task training improves gait but not vascular health in active older adults without dementia. Arch Gerontol Geriatr 2016;63:18-27. 10.1016/j.archger.2015.11.008 [DOI] [PubMed] [Google Scholar]
- 21.Shigematsu R, Okura T, Sakai T, et al. Square-stepping exercise versus strength and balance training for fall risk factors. Aging Clin Exp Res 2008;20:19-24. 10.1007/BF03324743 [DOI] [PubMed] [Google Scholar]
- 22.Teixeira CV, Gobbi S, Pereira JR, et al. Effects of square-stepping exercise on cognitive functions of older people. Psychogeriatrics 2013;13:148-56. 10.1111/psyg.12017 [DOI] [PubMed] [Google Scholar]
- 23.Shigematsu R, Okura T, Nakagaichi M, et al. Effects of exercise program requiring attention, memory and imitation on cognitive function in elderly persons: a non-randomized pilot study. J Gerontol Geriatr Res 2014;3:1-6. 10.4172/2167-7182.1000147 [DOI] [Google Scholar]
- 24.Knight E, Stuckey MI, Prapavessis H, et al. Public Health Guidelines for Physical Activity: Is There an App for That? A Review of Android and Apple App Stores. Eysenbach G, editor. JMIR mHealth uHealth 2015;3:e43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gill DP, Gregory MA, Zou G, et al. The healthy mind, healthy mobility trial: A novel exercise program for older adults. Med Sci Sports Exerc 2016;48:297-306. 10.1249/MSS.0000000000000758 [DOI] [PubMed] [Google Scholar]
- 26.Berenguer A, Goncalves J, Hosio S, et al. Are Smartphones Ubiquitous? An in-depth survey of smartphone adoption by seniors. IEEE 2016;6:104-10.