

Abstract
Background:
Tobacco use is one of the leading causes of preventable deaths in the world. The aim of this study was to determine the prevalence of all common types of tobacco use and identify factors associated with tobacco use among adults in Tehran based on information from the population-based Burden of Obstructive Lung Disease study in Tehran.
Materials and Methods:
This study had a stratified cluster sampling strategy with proportional allocation within strata. The target population was all noninstitutionalized residents of Tehran over 18 years of age in 2013. A total of 1798 individuals were visited in 22 districts of Tehran; 811 (45.1%) men and 987 (54.9%) women participated in structured interviews.
Results:
The estimated prevalence of current cigarette smoking was 10.6% overall, 20.9% in men and 2.2% in women. The prevalence of smoking was the highest among respondents between 45 and 54 years in both males and females. The mean age of initiation of tobacco smoking was 21.04 ± 6.42 years. The mean Fagerström test score was 2.87 ± 2.36 among current smokers. The mean number f cigarettes smoked daily by the participants was 11.39 ± 10.92 cigarettes/day (95% confidence interval = 12.58–10.21) (range 1–60 cigarettes).
Conclusions:
The 10.6% prevalence of cigarette smoking is alarming in Tehran. We found that male gender, hookah smoking experience, and poor health status were major risk factors in our study population. Hookah smoking can be considered as a reflection of tobacco smoking in the society.
KEY WORDS: Iran, prevalence, tobacco
INTRODUCTION
Tobacco use is one of the leading causes of preventable deaths in the world.[1,2] Smoking-related diseases such as chronic obstructive pulmonary disease (COPD), cancer, and cardiovascular disease are the main causes of premature death worldwide.[3] These days the prevalent rate of tobacco smoking estimated around 1.3 billion smokers are expected to increase to 1.6 billion by 2025, and the number of annual deaths because of smoking-related diseases is expected to reach 8.3 million. According to different studies, smoking kills more people than HIV/AIDS by 50% in 2015 and expected to be the main cause for 10% of all deaths in the world.[4]
Tobacco smoking by use of water pipe-also known as hookah or shisha is traditionally common in the Middle East and dates back to four centuries ago in ancient Persia and India.[5] According to studies, patterns of water pipe smoking vary across regions depending on the appearance, shape and size of the hookah, and the type of tobacco smoked.[6] A systematic review found that water pipe smoking is notably associated with wide range of diseases including lung cancer, respiratory diseases, low birth weight, and periodontal disease. The common practice of sharing water pipe paraphernalia (mouthpieces) increases the risk of transmission of tuberculosis and orally transmitted viral infections such as herpes simplex.[7]
The introduction of the Framework Convention on Tobacco Control in 2003 and its ratification by 177 countries around the world reflects the growing global efforts to control tobacco.[8] Like many countries, Iran has emphasized on the implementation of this law as an appropriate legal means to achieve tobacco control in country.[9,10] During the past years, attempts have been put into different tobacco control activities in Iran. Examples include fatwa of clergymen on the ban of smoking by the authoritative religious leaders ratified by the parliament on July 23, 1992 and by the government announcement on August 21, 1994 to decrease tobacco consumption, ban on public sale and use of tobacco by the government on October 29, 1997, Vice President's decree on July 15, 2002, and comprehensive tobacco control guidelines ratified by the parliament in October 2006.[9]
Developing countries comprise a large portion of global tobacco burden which reaches to 84% of all current smokers worldwide.[11] Studies on developing nations showed a smoking prevalence of 49% for men and 8% for women in low- and middle-income countries.[12] In addition, the harmful effects of passive smoking on nonsmokers have been previously confirmed.[13,14]
Recently, we advanced the 50th anniversary of the first report of the US surgeon general on health effects of tobacco smoking.[15]
The international, population-based “Burden of Obstructive Lung Disease” (BOLD) initiative was designed a decade ago to develop robust models that can be used to estimate the prevalence and current and future economic burden of COPD.[16]
It is necessary to have a wider perspective of the current cigarette smoking status to decrease its prevalence and eliminate the related health hazards. The majority of previous studies done in this realm of science only emphasized on industrial cigarette smoking with very little or no attention to other types of tobacco use such as hookah smoking. Therefore, the aim of the present study was to determine the prevalence of all common types of tobacco use and identify factors associated with tobacco use by adults in Tehran based on information from the population-based BOLD study in Tehran.
MATERIALS AND METHODS
Population and sampling strategy
The target population in this study was the population of Tehran, which was 8.1 million at the time of conduct of the study.
Sample size
Using design effect of 1.5 from the previous surveys, prevalence rate of 11% from previous similar studies, and a response rate of 60%, total sample size was estimated to be 750.
Sampling plan
This study followed a stratified cluster sampling strategy with proportional allocation within strata. The target population was all noninstitutionalized residents of Tehran between 18 and 40 years of age in one group and over forty in another group, in 2013.
Considering the 22 municipal districts of Tehran, the appropriate number of clusters was weighted for each district proportional to the number of households in the 22 districts. The number of clusters was based on total sample size, mean household members, and logistical facilities for subject enumeration, transport, and examination.
For each cluster, a team of three members (one male and one female younger than 28 years as interviewers and a driver between 40 and 55 years) approached the household selected through the aforementioned random selection of clusters and continued enumeration in 10 neighboring households in a systematic manner. If there was more than one person in the selected household, interviewers were advised to use the Kish method to choose the right participant(s). This method is based on a table of random numbers and is named according to the statistician who invented it (the number of people in the household is discovered, and a random number is chosen to select a particular person).[17]
Examination protocol
The examination protocol included a questionnaire covering respiratory symptoms, health status, activity limitation, and exposure to potential risk factors, such as tobacco smoke, occupational risk factors, and biomass exposure.
Questionnaires
The core questionnaire was developed from preexisting validated questionnaires used in multinational studies.[18] The questionnaire contained information about respiratory symptoms, exposure to potential risk factors such as smoking, occupation, respiratory diseases, comorbidities, healthcare provision, medication use, activity limitation, and health status. We used BOLD questionnaire, which includes sections adopted from the 1978 ATS/DLD Respiratory Symptom Questionnaire, Respiratory Health Study, the CNR study, and the OLIN study. It also includes the SF-12 to assess the overall health status.[19]
Participants also completed a “stages of change” questionnaire, which assessed readiness of current cigarette smokers to quit smoking. All questionnaires were translated to Persian first and then back-translated to English by a different translator. The questionnaires were administered by trained certified staff; self-administration of questionnaires was not allowed.
In this study, four levels were defined for smoking experience: (a) never-smokers, (b) ex-smokers (smoked < 100 cigarettes in their lifetime, but had not smoked in the past 90 days), (c) current smokers (smoked in the past 90 days and smoked more than 100 cigarettes in their lifetime), and (d) experienced smokers (smoked at least once in their lifetime, but had smoked < 100 cigarettes in their lifetime).
Statistical analysis
In calculating standard errors and the 95% confidence interval (CI) for categorical and continuous variables, the cluster sampling design was used and adjusted. In addition to descriptive statistics, the odds ratios (ORs) were calculated with multivariate logistic regression to control for the potential confounding variables and the cluster design effects. Full research design and spirometry protocol have been published elsewhere.[19]
RESULTS
Participants
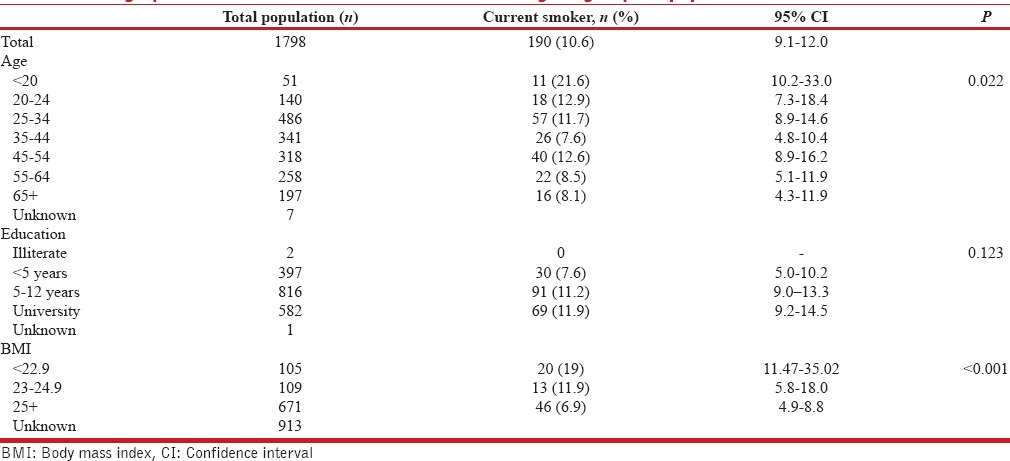
In total, 1798 individuals were questioned in all districts of Tehran; 811 (45.1%) men and 987 (54.9%) women participated in structured interviews. The selected districts were in the North, South, West, East, and center of Tehran. Table 1 shows the demographic characteristics of subjects including age groups and comorbidities.
Table 1.
Demographic characteristics of current smokers among subgroups of population
Tobacco smoking habits
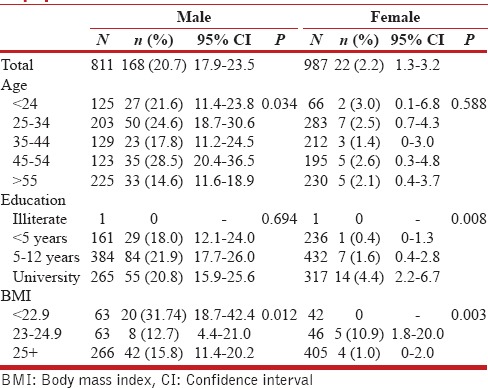
The prevalence of current cigarette smoking was found to be 190 (10.6%) overall, 168 (20.9%) in men and 22 (2.2%) in women [Table 2]. The prevalence of current smoking was the highest among respondents between 45 and 54 years irrespective of gender. Males with body mass index (BMI) of 18–23 had a higher prevalence of smoking (30.5% [95% CI = 18.7–42.4]).
Table 2.
Frequency of current smokers among subgroups of population in male and female
The prevalence of ever hookah smoking was 27.4% (n = 493), in men 18.7% (n = 336) and 8.7% (n = 157) in women (P ≤ 0.001), and the mean age of onset of hookah smoking was 25.2 (95% CI 23.6–26.7) years. One hundred (5.8%) participants smoked hookah daily (87 [4.9%] of men and 13 [0.7%] of women) and 168 (9%) smoked hookah at least once a month.
The prevalence of ever cigarette smoking was 37.6% (n = 676) in men and 3.6% (n = 65) in women (P ≤ 0.001). The mean age of onset of cigarette smoking was 20.4 (95% CI 19.5–21.2) years.
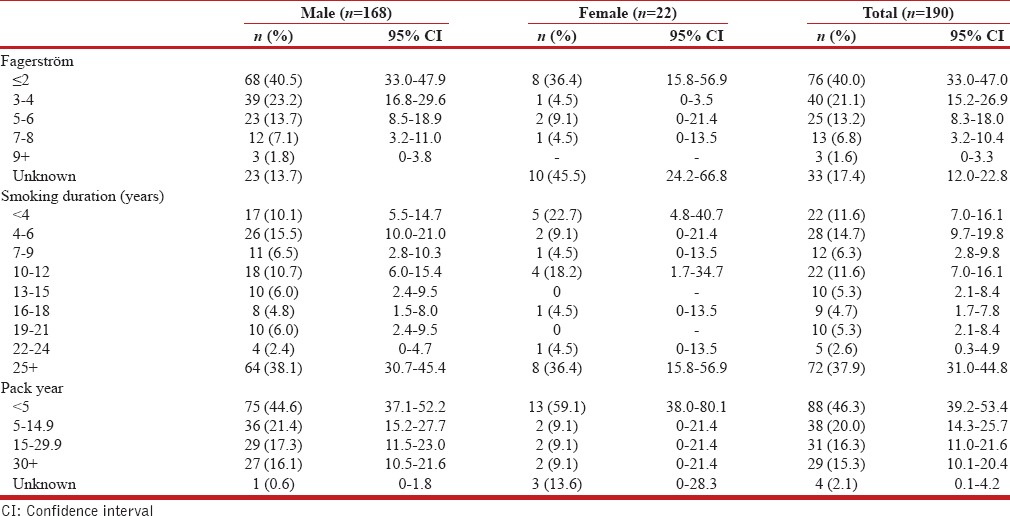
The mean age of initiation of tobacco use by ex-smokers and current smokers was 21.04 ± 6.42 years. The mean Fagerström test score in current cigarette smokers was 2.87 ± 2.36 [Table 3]. The mean number of cigarettes smoked daily by smokers was 11.39 ± 10.92 cigarettes/day (CI 95% =12.58–10.21) (range 1–60 cigarettes).
Table 3.
Characteristics of smokers in males, females, and total
We performed univariate and multivariate logistic regression analyses to assess the association of tobacco smoking in any form and risk factors. As presented in Table 4, in multivariate logistic regression analysis for cigarette smoking, the OR for age was 0.988 (95% CI: 0.978–0.997), and after including gender, parental smoking during childhood, education and BMI in the model, and after adjusting for all these potential factors in the model, we found that male gender, hookah smoking experience, and health status were all major risk factors in our study population [Table 5]. We performed logistic regression analysis for hookah smoking experience as well [Table 4].
Table 4.
The odds ratio for hookah smoking
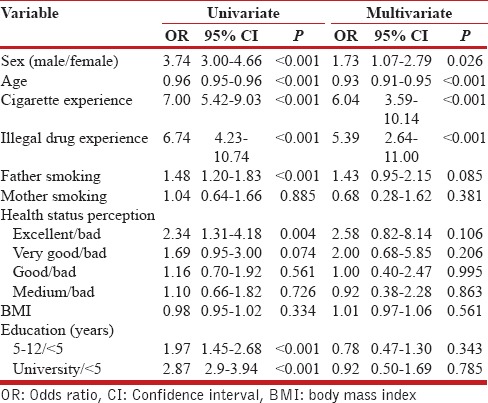
Table 5.
The odds ratio for cigarette smoking

DISCUSSION
In this study, we assessed the prevalence of tobacco smoking in residents of Tehran aged 18 and over using structured questionnaires. The sample of this survey was representative of the entire adult population in Tehran. A key finding of this study was that the prevalence of cigarette smoking was 10.6% (20.9% in men and 2.2% in women). According to a national survey on cigarette smoking prevalence from 1991 to 1999, this rate was 11.7% (24% in males and 1.5% in females).[20] Azizi reported an almost similar prevalence rate in Tehran (10.8%).[21] Furthermore, according to the WHO report in 2008 (the MPOWER package), the prevalence of daily tobacco smoking was 11.9% in the total population (20.9% in men and 2.9% in women).[22] It seems that the prevalence of tobacco smoking has been changed little among Iranians in a quarter of a century, i.e., from 1999 to 2014.
Considering the above-mentioned rates, it seems that in women, there has been an enhancement of tobacco consumption over time. Cigarette smoking by women is considered as a stigma in the Iranian mores. Thus, underreporting of smoking by women may occur in epidemiological studies. According to a study by Sarraf-Zadegan et al. in Isfahan, there was a significant difference between self-reported and biochemically indicated (by serum cotinine) rates of tobacco use by women (1.3% vs. 6.7%).[23] The difference between self-reported hookah and cigarette smoking experience by women points to the fact that since hookah smoking by women is more socially acceptable, women are more frank about reporting hookah smoking. Moreover, the prevalence of cigarette smoking is often higher in women with moderate or high level of education. Lund and Lindbak reported that the probability of being a current smoker was higher for those with secondary education compared to lower levels of education; this difference was statistically significant for Iranian women.[24]
Another factor contributing to the increased prevalence of waterpipe smoking is its higher social acceptability compared to other forms of tobacco smoking. In many countries, notably, in the Middle East region, water pipe smoking is commonly practiced in social activities, and all family members and friends smoke together.
In general, the estimated prevalence of daily tobacco smoking in men ranged from more than 50% in Russia, Indonesia, Armenia, Kiribati, Laos, Papua New Guinea, and Timor-Leste to < 10% in Antigua and Barbuda, Dominica, Ethiopia, Ghana, Niger, Nigeria, Sao Tome and Principe, Sudan, and Suriname. Low prevalence of tobacco smoking in men (<20%) in some developed countries shows that strategies to decrease the prevalence of smoking have been successful.[25] These variations of tobacco smoking rate are likely due to differences in the implementation and enforcement of tobacco control laws in different countries.[26]
Comparison of ever and/or current cigarette and/or hookah smoking between men and women shows 7–10-fold higher prevalence in men with the exception of hookah smoking prevalence, which is almost similar between males and females. Hookah smoking can be considered as a reflection of tobacco smoking in the society.
In our study, rate of tobacco use increased with age and was the highest in subjects aged 45–54 years. Meysamie et al. reported the highest rate of smoking in the same age group.[27]
The mean number of cigarettes smoked by the participants in our study was 11.39 ± 10.92 cigarettes/day, which was < 16.8 (CI 95% =15.4–18.3) cigarettes/day reported by Meysami et al. in 2004[28] and 22.19 cigarettes/day reported by Sharifi et al.[29] The reduction in the mean number of cigarettes smoked per day could be considered as a reflection of an actual decrease in tobacco demand in a population or even an increase in the price of tobacco products in the country over the past years. Moreover, we should have in mind that emerging and/or re-emerging of smoking and smokeless products such as e-cigarettes, hookah, and chewing tobacco is concerning, and this situation is worsening in countries with high prevalence of dual or multiple addictions to tobacco products. The percentage of smokers who use different types of tobacco products depends on the region of the world. El-Roueiheb et al.[30] reported that the prevalence of current hookah smoking was about ten times higher than that of current cigarette smoking in Lebanon. Analysis of the New York Theological Seminary data by Amrock et al. in 2014 revealed that of all the adolescents evaluated in developing and developed countries, 7.3% had occasionally tried hookah smoking, while 2.6% were current hookah users (defined as hookah smoking at least once in the past 30 days).[31] Ward et al. in 2006 reported the prevalence of cigarette smoking to be 3–4 times higher than that of hookah smoking in Syria.[32] Water pipe smoking is a health risk behavior that seems to be reemerging. Furthermore, adolescent smokers often mix the hookah tobacco with illicit drugs such as marijuana or hashish or replace the water in the pipe with alcoholic beverages, which further adds to the health hazards of hookah smoking. Water pipe smoking is believed to be a gateway to cigarette smoking or use of other psychoactive substances. In many countries, adolescents use water pipe as their initial smoking experience.[33,34] As stated above, it seems that hookah smoking is becoming increasingly popular in Iran and further studies are required in this realm.
An important finding of this study was that a large number of smokers had a BMI of 18–23. Similarly, Eisen et al.[35] in 1993 in Vietnam found that former smokers had higher BMI than smokers, and Xu et al.[36] in 2007 in China revealed a negative association between the number of cigarettes smoked daily and body weight indicated by BMI. Some other epidemiologic studies have demonstrated that smokers tend to have lower body weight than nonsmokers.[37,38] The main reason behind smoking-related weight change seems to be complex and involves various pathways. Nicotine inhaled from tobacco is the most important component affecting body weight. Nicotine increases the level of different neurotransmitters, such as catecholamines, dopamine and serotonin in the brain, and consequently reduces appetite and food intake.[38,39] This phenomenon could explain why tobacco smokers tend to lose weight, and on the contrary, smoking cessation is mostly followed by weight gain.[40]
We found a significant negative association between health status and cigarette smoking. Schmitz et al.[40] noticed that smokers reported a significantly poorer quality of life and greater disability than nonsmokers. Tavafian et al.[41] in 2009 reported that water pipe smoking was significantly associated with poorer health perception. In their study, the mean scores of the Short Form Health Survey for water pipe smokers were lower than those of nonsmokers. In our study, we did not find any negative association between hookah smoking and health status perception, which could be due to our inclusion criteria and the presence of occasional water pipe smokers in our study. Therefore, in our study, contrary to the trend observed for cigarette smoking, hookah smokers were not aware of the adverse health effects of hookah smoking.
Strengths and limitations of this study
The present study had some limitations. First, the BOLD protocol is based on a cross-sectional dataset; therefore, we could not establish a causality relationship between smoking and other important variables. The second limitation was that the information could be subject to reporting or recall bias as it was self-reported. However, many studies have shown that smoking prevalence reports based on biochemical data are comparable with self-reported data.[23]
Last but not least, for the purpose of this study, we selected subjects who were 18 years or older. Individuals aged 17 years or younger were excluded from the study, which might have been demonstrated a neglected risk factor for this group of age.
The strength of this study was that we used a population-based strategy with an acceptable response rate, in a broad age range. In addition, we recruited equal number of participants from both sexes.
CONCLUSION
The 10.6% prevalence of cigarette smoking in Tehran is concerning. It seems that the prevalence of cigarette smoking in Iran did not increase over the past 25 years; whereas, high prevalence of hookah smoking in both men and women is alarming. Comparison of ever and/or current smoking of cigarette and/or hookah between men and women showed 7–10-fold higher prevalence in men with the exception of hookah smoking prevalence, which was almost the same in men and women.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Tonstad S, Andrew Johnston J. Cardiovascular risks associated with smoking: A review for clinicians. Eur J Cardiovasc Prev Rehabil. 2006;13:507–14. doi: 10.1097/01.hjr.0000214609.06738.62. [DOI] [PubMed] [Google Scholar]
- 2.Brand RM, Jones DD, Lynch HT, Brand RE, Watson P, Ashwathnayaran R, et al. Risk of colon cancer in hereditary non-polyposis colorectal cancer patients as predicted by fuzzy modeling: Influence of smoking. World J Gastroenterol. 2006;12:4485–91. doi: 10.3748/wjg.v12.i28.4485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Beaglehole R, Bonita R, Horton R, Adams C, Alleyne G, Asaria P, et al. Priority actions for the non-communicable disease crisis. Lancet. 2011;377:1438–47. doi: 10.1016/S0140-6736(11)60393-0. [DOI] [PubMed] [Google Scholar]
- 4.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Maziak W, Fouad FM, Asfar T, Hammal F, Bachir EM, Rastam S, et al. Prevalence and characteristics of narghile smoking among university students in Syria. Int J Tuberc Lung Dis. 2004;8:882–9. [PubMed] [Google Scholar]
- 6.Riachy M, Rehayem C, Khoury C, Safi J, Khayat G, Aoun-Bacha Z, et al. Are narghile smokers different from cigarette smokers? Rev Mal Respir. 2008;25:313–8. doi: 10.1016/s0761-8425(08)71550-x. [DOI] [PubMed] [Google Scholar]
- 7.Akl EA, Gaddam S, Gunukula SK, Honeine R, Jaoude PA, Irani J. The effects of waterpipe tobacco smoking on health outcomes: A systematic review. Int J Epidemiol. 2010;39:834–57. doi: 10.1093/ije/dyq002. [DOI] [PubMed] [Google Scholar]
- 8.World Health Organization. WHO Framework Convention on Tobacco Control. [Last accessed on 2013 Oct 14]. Available from: http://www.who.int/fctc/text_download/en/index.html .
- 9.Sharifi H, Hessami Z, Masjedi MR. Health experts' opinions about tobacco control activities in Iran: Results from a Delphi panel of national experts. Tanaffos. 2012;11:50–5. [PMC free article] [PubMed] [Google Scholar]
- 10.Sharifi H, Ramezankhani A, Fallah Tafti S, Sharif Kashani B, Padyab M, Heydari G. Public awareness about framework convention on tobacco control (FCTC) in Tehran. Tanaffos. 2009;8:26–32. [Google Scholar]
- 11.Jha P, Chaloupka FJ. Tobacco Control in Developing Countries. Oxford, UK: Oxford University Press; 2000. [Google Scholar]
- 12.Slama K. Current challenges in tobacco control. Int J Tuberc Lung Dis. 2004;8:1160–72. [PubMed] [Google Scholar]
- 13.Health effects of exposure to environmental tobacco smoke. California Environmental Protection Agency. Tob Control. 1997;6:346–53. doi: 10.1136/tc.6.4.346. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cook DG, Strachan DP. Health effects of passive smoking-10: Summary of effects of parental smoking on the respiratory health of children and implications for research. Thorax. 1999;54:357–66. doi: 10.1136/thx.54.4.357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Smoking and Health: Report of the Advisory Committee to the Surgeon General of the Public Health Service, 1964. Washington, DC: US Department of Health, Education, and Welfare; 1964. [Last accessed on 2013 Dec 09]. Available from: https://www.profiles.nlm.nih.gov/ps/access/NNBBMQ.pdf . [Google Scholar]
- 16.Buist AS, Vollmer WM, Sullivan SD, Weiss KB, Lee TA, Menezes AM, et al. The burden of obstructive lung disease initiative (BOLD): Rationale and design. COPD. 2005;2:277–83. [PubMed] [Google Scholar]
- 17.Binson D, Catania JA. Random selection in a national telephone survey: A comparison of the Kish, next-birthday, and last-birthday methods. J Off Stat. 2000;16:53. [Google Scholar]
- 18.Global Initiative for Chronic Obstructive Lung Disease Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease. 2013. [Last accessed 2013 Jul 20]. Available from: http://www.goldcopd.org/uploads/users/files/GOLD_Report_2013_Feb20.pdf .
- 19.Sharifi H, Masjedi MR, Emami H, Ghanei M, Buist S. Burden of obstructive lung disease study in Tehran: Research design and lung spirometry protocol. Int J Prev Med. 2014;5:1439–45. [PMC free article] [PubMed] [Google Scholar]
- 20.Mohammad K, Nourbala AA, Madjdzadeh R, Karimlou M. Trend of smoking prevalence in Iran from 1991 to 1999 based on two national health survey. Hakim Res J. 2001;4:290–4. [Google Scholar]
- 21.Azizi F. Tehran Lipid and Glucose Study Tehran, Endocrine Research Center, Shaheed Beheshti University of Medical Sciences. J Res Med. 2003;27:47e52. [Google Scholar]
- 22.World Health Organization. WHO Report on the Global Tobacco Epidemic, 2008: The MPOWER package. Geneva: WHO; 2008. [Last accessed on 2008 Mar 26]. Available from: http://www.who.int/tobacco/mpower/mpower_report_full_2008.pdf . [Google Scholar]
- 23.Sarraf-Zadegan N, Boshtam M, Shahrokhi S, Naderi GA, Asgary S, Shahparian M, et al. Tobacco use among Iranian men, women and adolescents. Eur J Public Health. 2004;14:76–8. doi: 10.1093/eurpub/14.1.76. [DOI] [PubMed] [Google Scholar]
- 24.Lund M, Lindbak RL. Norwegian tobacco statistics 1973-2006. Oslo: Norwegian Institute for Alcohol and Drug Research; 2007. [Google Scholar]
- 25.Ng M, Freeman MK, Fleming TD, Robinson M, Dwyer-Lindgren L, Thomson B, et al. Smoking prevalence and cigarette consumption in 187 countries, 1980-2012. JAMA. 2014;311:183–92. doi: 10.1001/jama.2013.284692. [DOI] [PubMed] [Google Scholar]
- 26.Joossens L, Raw M. The Tobacco Control Scale: A new scale to measure country activity. Tob Control. 2006;15:247–53. doi: 10.1136/tc.2005.015347. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Meysamie A, Ghaletaki R, Haghazali M, Asgari F, Rashidi A, Khalilzadeh O, et al. Pattern of tobacco use among the Iranian adult population: Results of the national survey of risk factors of non-communicable diseases (SuRFNCD-2007) Tob Control. 2010;19:125–8. doi: 10.1136/tc.2009.030759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Meysami AP, Ghodsi SM, Eftekhar B. Pattern of cigarette smoking in an Iranian village. Tanaffos. 2004;10:53–61. [Google Scholar]
- 29.Sharifi H, Kharaghani R, Emami H, Hessami Z, Masjedi MR. Efficacy of harm reduction programs among patients of a smoking cessation clinic in Tehran, Iran. Arch Iran Med. 2012;15:283–9. [PubMed] [Google Scholar]
- 30.El-Roueiheb Z, Tamim H, Kanj M, Jabbour S, Alayan I, Musharrafieh U. Cigarette and waterpipe smoking among Lebanese adolescents, a cross-sectional study, 2003-2004. Nicotine Tob Res. 2008;10:309–14. doi: 10.1080/14622200701825775. [DOI] [PubMed] [Google Scholar]
- 31.Amrock SM, Gordon T, Zelikoff JT, Weitzman M. Hookah use among adolescents in the United States: Results of a national survey. Nicotine Tob Res. 2014;16:231–7. doi: 10.1093/ntr/ntt160. [DOI] [PubMed] [Google Scholar]
- 32.Ward KD, Eissenberg T, Rastam S, Asfar T, Mzayek F, Fouad MF, et al. The tobacco epidemic in Syria. Tob Control. 2006;15(Suppl 1):i24–9. doi: 10.1136/tc.2005.014860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Knishkowy B, Amitai Y. Water-pipe (narghile) smoking: An emerging health risk behavior. Pediatrics. 2005;116:e113–9. doi: 10.1542/peds.2004-2173. [DOI] [PubMed] [Google Scholar]
- 34.Kulwicki A, Hill Rice V. Arab American adolescent perceptions and experiences with smoking. Public Health Nurs. 2003;20:177–83. doi: 10.1046/j.0737-1209.2003.20304.x. [DOI] [PubMed] [Google Scholar]
- 35.Eisen SA, Lyons MJ, Goldberg J, True WR. The impact of cigarette and alcohol consumption on weight and obesity. An analysis of 1911 monozygotic male twin pairs. Arch Intern Med. 1993;153:2457–63. [PubMed] [Google Scholar]
- 36.Xu F, Yin XM, Wang Y. The association between amount of cigarettes smoked and overweight, central obesity among Chinese adults in Nanjing, China. Asia Pac J Clin Nutr. 2007;16:240–7. [PubMed] [Google Scholar]
- 37.Chiolero A, Faeh D, Paccaud F, Cornuz J. Consequences of smoking for body weight, body fat distribution, and insulin resistance. Am J Clin Nutr. 2008;87:801–9. doi: 10.1093/ajcn/87.4.801. [DOI] [PubMed] [Google Scholar]
- 38.Williamson DF, Madans J, Anda RF, Kleinman JC, Giovino GA, Byers T. Smoking cessation and severity of weight gain in a national cohort. N Engl J Med. 1991;324:739–45. doi: 10.1056/NEJM199103143241106. [DOI] [PubMed] [Google Scholar]
- 39.Du H, Bennett D, Li L, Whitlock G, Guo Y, Collins R, et al. Physical activity and sedentary leisure time and their associations with BMI, waist circumference, and percentage body fat in 0.5 million adults: The China Kadoorie Biobank study. Am J Clin Nutr. 2013;97:487–96. doi: 10.3945/ajcn.112.046854. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Schmitz N, Kruse J, Kugler J. Disabilities, quality of life, and mental disorders associated with smoking and nicotine dependence. Am J Psychiatry. 2003;160:1670–6. doi: 10.1176/appi.ajp.160.9.1670. [DOI] [PubMed] [Google Scholar]
- 41.Tavafian SS, Aghamolaei T, Zare S. Water pipe smoking and health-related quality of life: A population-based study. Arch Iran Med. 2009;12:232–7. [PubMed] [Google Scholar]