

Abstract
Transposition of great arteries (TGA) is more commonly associated with D-malposition of great arteries where anterior aorta produces characteristic “I” sign in the three-vessel view (3VV) in fetal heart imaging. We describe two cases with TGA and L-malposition of aorta where 3VV imaging showed an apparently normal arrangement of vessels while outflow tract imaging proved vital in diagnosing transposition anatomy. Apparently, normal 3VV in the presence of disproportionate vessel caliber and inability to produce normal outflow images should raise the suspicion. Attempts should be made to produce views to show great arteries originating from respective ventricles to rule out ventriculoarterial discordance and to complete segmental analysis.
Keywords: “I” sign, fetal echocardiography, three-vessel view, transposition of great arteries with L-malposition
BRIEF SUMMARY
Three-vessel view (3VV) and arches view are important parts of fetal cardiac imaging. We describe two fetuses with an uncommon variant of transposition of great arteries (TGA) where both these views showed apparently normal arrangement of the great arteries.
Case 1
A second gravida mother at 23 weeks of gestation was referred for fetal echocardiography, due to suspected aortic dilatation in anomaly scan. Detailed fetal imaging showed situs solitus, levocardia with normal cardiac axis. Four-chamber view revealed atrioventricular concordance, normal atrioventricular valves, and good-sized ventricles. 3VV and arches views looked apparently normal [Figure 1a and b]. Further imaging showed pulmonary artery (PA) originating from the left ventricle, aorta from the right ventricle, and aorta was to the left of PA confirming the presence of TGA with the left and anterior aorta [Figure 1c–f]. The arches view simulated a normal pattern but had the aortic arch to the left of ductal arch, and the latter was seen coursing in front of the spine to join the isthmus [Figure 1b, Supplementary Figure 1 (566.5KB, tif) ]. Although the family was counseled in detail about the available postnatal corrective surgical treatment, they decided to discontinue pregnancy. Fetal autopsy confirmed ventriculoarterial discordance with the left and anterior aorta [Figures 2 and 4c].
Figure 1.
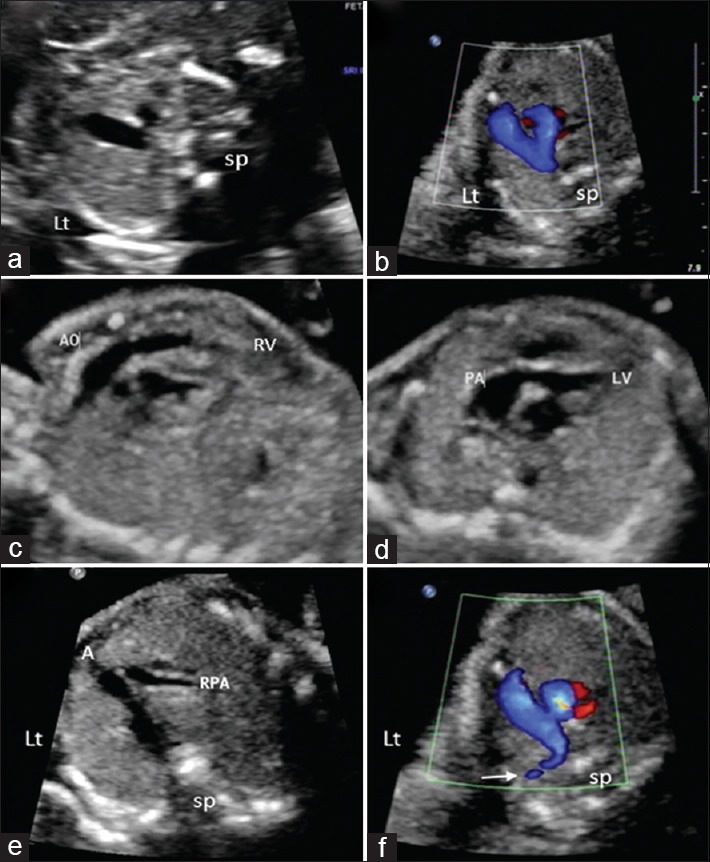
Fetal echocardiographic views of case 1: (a) three-vessel view showing the “dash-dot-dot” pattern from left to right; (b) arches view shows left-sided arch with longer limb on the left side and normal confluences of both arches; (c) anteriorly placed right ventricle giving off to the nonbifurcating vessel; (d) bifurcating vessel arising from the left ventricle; (e) the second vessel in three-vessel view giving off to right pulmonary artery; (f) one arch vessel (arrow) seen originating from the first vessel on the left confirming this as Aorta A: Aorta, PA: Pulmonary artery, LV: Left ventricle, RV: Right ventricle, SP: Spine, Lt: Left of fetus
Figure 2.

Fetal autopsy images of case 1: (a) aorta to the left and anterior of the pulmonary artery; (b) the branching pulmonary artery to the right; (c and d) aorta arising from the right ventricle and pulmonary artery from the left ventricle. Black star indicates aorta and arrow indicates pulmonary artery
Figure 4.

The relation of great vessels in normal heart, D- and L-transposition as seen in autopsy specimen (a, c, e) and in three-vessel view in fetal echocardiography (b, d, f). (a and b) normal three-vessel view where pulmonary artery is to the left and anterior; (c and d) images of case 1 where aorta is to the left and anterior; (e and f) transposition of great arteries where aorta is anterior and to the right of pulmonary artery. A: Aorta, P: Pulmonary artery, S: Superior vena cava, RV: Right ventricle, Lt: Left of fetus, SP: Spine
Fetal echo showing three-vessel view in case 2: (a) “dot-dot-dot” pattern in three-vessel view with aorta on the left and anterior to pulmonary artery both seen in cross section; (b) the “I sign” with only anterior aorta with the arch seen.
A: Aorta, P: Pulmonary artery, S: SVC
Case 2
In the following year, another 22 weeks old fetus who was referred for echocardiography had atrioventricular discordance with the L-malposed aorta. In this case also, 3VV resembled normal arrangement of vessels, but the caliber difference between aorta and PA was obvious [Figure 2a and b]. There was a large ventricular septal defect noted in addition. Unfortunately, this pregnancy was also discontinued, and the fetus was sent for autopsy which confirmed the echocardiography findings [Figures 2c–d and 3]. The additional finding was an unusually narrow ductal arch.
Figure 3.

Fetal echocardiography and autopsy images of case 2: (a) near-normal pattern of three-vessel view with aorta to the left of pulmonary artery; (b) right pulmonary artery (arrow) originating from the great vessel connected to the left ventricle; (c and d) aorta (star) from the right ventricle and the ventricular septal defect (broad arrow). A: Aorta, P: Pulmonary artery, LV: Left ventricle, SP: Spine, Lt: Left of fetus
DISCUSSION
Above-mentioned cases represent rare types of TGA where aorta is placed anterior and to the left of PA (Levoposition or L-malposed aorta or SDL arrangement) unlike the common type where aorta is to the right of PA. L-malposition of aorta in other conditions such as congenitally corrected TGA and double outlet right ventricle has been reported but remains an uncommon entity in D-looped ventricles.[1,2,3]
The most common association noted is conoventricular septal defect (90%) as seen in our second case. Goor and Edwards proposed isolated inversion of the conal septum in reverse as a cause for such malformation while Houyel et al. considered the involvement of ventricular component also.[3,4]
During fetal echocardiography, rightward convexity of the great vessel arising from the anterior ventricle and the “I sign” in 3VV have been considered as pointers for TGA.[5,6] In both cases, these signs were noted, but interestingly normal arrangement pattern of 3VV known as the “dash-dot-dot” also could be produced. In a normal 3VV, the arrangement of PA, aorta, and superior vena cava (SVC) is from left to right and anterior to posterior, with a “dash” pattern created by PA continuing into DA seen in long axis while aorta and SVC seen in cross section forming the “dot-dot” pattern [Figure 4a and b]. A similar pattern seen in TGA with L-malposition can be explained by the left and anteriorly placed aorta continuing as aortic arch giving the false “dash” pattern. The branch PA occupies the mid position simulating a smaller second vessel in 3VV [Figure 1e and 4d]. The 3VV in both cases seem to be at a cephalad section with less lung tissue, which may be a reason for the deceiving pattern.
Origin of arch vessels from the leftward great artery also is a clue to identify it as aorta [Figure 1f]. In the more common D-TGA, aorta will be anterior and to the right of PA where at times the “dash-dot-dot” pattern may be seen but with altered anteroposterior alignment [Figure 4f and corresponding autopsy figure Figure 4e]. The above-mentioned points stress on the importance of seeing normal arrangement, anteroposterior alignment, and caliber of the great vessels in 3VV.
Similarly, the arch view in case 1 had a normal “V to the left” pattern with longer limb seen on the left and shorter limb to the right, though the longer left-sided arch was aortic arch vice versa to the routine where ductal arch is to the left [Figure 1b]. In arch view with normal outflows, the longer limb is by the ductal arch as the PA arising from the anterior right ventricle takes a longer course to reach posteriorly [Supplementary Figure 2 (690.9KB, tif) ].
Fetal echo images of arches: (a) arches view in a normal fetal heat (tick-sign) shows ductal arch on the left and forms the longer limb; (b) arches view in case 1 shows similar pattern but aortic arch on the left and forms the longer limb. AA: Aortic arch, DA: Ductutal arch
These cases highlight the importance of sequential segmental analysis and outflow imaging to define ventriculoarterial connections without being biased by pattern recognition alone. Necessary angulation in 3VV and the “circle and sausage” outflow view would help to show PA branching. However, importance of pattern recognition in 3VV should not be ignored, as an unusual pattern during screening view remains the reason for referral in many outflow anomalies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Freedom RM, Harrington DP, White RI., Jr The differential diagnosis of levo-transposed or malposed aorta. An angiocardiographic study. Circulation. 1974;50:1040–6. doi: 10.1161/01.cir.50.5.1040. [DOI] [PubMed] [Google Scholar]
- 2.Coto EO, Jiménez MQ, Cabrera A, Deverall PB, Caffarena JM. Aortic levopositions without ventricular inversion. Eur J Cardiol. 1978;8:523–41. [PubMed] [Google Scholar]
- 3.Houyel L, Van Praagh R, Lacour-Gayet F, Serraf A, Petit J, Bruniaux J, et al. Transposition of the great arteries [S, D, L]. Pathologic anatomy, diagnosis, and surgical management of a newly recognized complex. J Thorac Cardiovasc Surg. 1995;110:613–24. doi: 10.1016/S0022-5223(95)70092-7. [DOI] [PubMed] [Google Scholar]
- 4.Goor DA, Edwards JE. The spectrum of transposition of the great arteries: With specific reference to developmental anatomy of the conus. Circulation. 1973;48:406–15. doi: 10.1161/01.cir.48.2.406. [DOI] [PubMed] [Google Scholar]
- 5.Menahem S, Rotstein A, Meagher S. Rightward convexity of the great vessel arising from the anterior ventricle: A novel fetal marker for transposition of the great arteries. Ultrasound Obstet Gynecol. 2013;41:168–71. doi: 10.1002/uog.11171. [DOI] [PubMed] [Google Scholar]
- 6.Ishii Y, Inamura N, Kawazu Y, Kayatani F, Arakawa H. ’I-shaped’ sign in the upper mediastinum: A novel potential marker for antenatal diagnosis of d-transposition of the great arteries. Ultrasound Obstet Gynecol. 2013;41:667–71. doi: 10.1002/uog.12312. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Fetal echo showing three-vessel view in case 2: (a) “dot-dot-dot” pattern in three-vessel view with aorta on the left and anterior to pulmonary artery both seen in cross section; (b) the “I sign” with only anterior aorta with the arch seen.
A: Aorta, P: Pulmonary artery, S: SVC
Fetal echo images of arches: (a) arches view in a normal fetal heat (tick-sign) shows ductal arch on the left and forms the longer limb; (b) arches view in case 1 shows similar pattern but aortic arch on the left and forms the longer limb. AA: Aortic arch, DA: Ductutal arch