

Abstract
Vitamin D synthesis takes place in the skin due to solar ultraviolet-B (UVB) radiation. Several studies have shown the association between low sun exposure, non-melanoma skin cancer (NMSC) and a lack of vitamin D synthesis. Since such synthesis in the body depends on the exposure of the skin to solar UVB radiation (290–320 nm), experimental measurements of this type of solar radiation are important. Tarapaca University in Arica, Chile, established a solar UV radiation laboratory in 2006 and since then this laboratory has performed systematic experimental solar UVB measurements using a calibrated biometer instrument. The results, which are presented in the current study, showed the association between NMSC and MSC rates, and the time required to produce 1,000 IU vitamin D with latitudinal variation. Solar UV index (UVI) levels reported in 6 cities from the north to the south of Chile indicated that the UVI ratio of monthly mean values was 1.8 times higher in Arica than in Punta Arenas in January (summer in Chile), whereas it was 14 times higher in June (winter). This factor is an important consideration, since vitamin D synthesis is directly associated with the exposure of individuals to solar UVB radiation. A similar trend was observed in Antofagasta, Santiago, Concepcion, Valdivia and Punta Arenas. It can be concluded from these data that there is a direct association between NMSC rates and mortality, and UVB radiation, meaning that this type of cancer would not depend on vitamin D synthesis and therefore on calcium uptake. By contrast, MSC rates increased with decreased levels of vitamin D, and thus calcium uptake, in all cities, with the only exception being Punta Arenas.
Keywords: vitamin D, skin cancer, ultraviolet light
Introduction
The major role of vitamin D in vertebrate animals and humans is to increase calcium and phosphate absorption for the mineralization of the skeleton. The most important source of this vitamin for individuals living at mid and low latitudes is vitamin D synthesis induced by solar ultraviolet-B (UVB) radiation (1). The recommended daily allowance (RDA) for vitamin D in the United States is 200 IU (5.0 µg), which is reasonable for adults who receive some sun exposure; however, in the absence of sun exposure, this RDA may be 2 to 3 times lower than that actually required to satisfy what the body requires (2). Vitamin D3 is efficiently produced via pre-vitamin D3 from the precursor 7-dehydrocholesterol when human skin is exposed to solar UVB (3,4).
The total volume of atmospheric ozone and cloudiness are also important factors that control UVB radiation, and the area of exposed skin and skin type is relevant to the amount of vitamin D synthesis (5). At subtropical latitudes, there is no alteration of vitamin D production during winter. At low latitudes, vitamin D synthesis continues throughout the winter at reduced capacity, and at high latitudes, there is no production for 4–6 months of the year (6). Vitamin D synthesis originates from two sources, firstly from solar or artificial UVB exposure, and secondly from dietary products and supplements in individuals who live at higher latitudes where solar UVB radiation is weak in winter (3,4).
Vitamin D deficiency is commonly found in risk groups such as postmenopausal women and individuals suffering from rickets, osteomalacia and osteoporosis, since vitamin D is vital for normal calcium metabolism and the maintenance of bone density (7). Vitamin D deficiency is also associated with an increased cardiovascular risk and arterial stiffness (8). Furthermore, it is associated with epidemic influenza, as solar radiation produces a seasonal variation that profoundly affects the pathogenesis of the disease (9,10).
Non-melanoma skin cancer (NMSC) is the most commonly occurring cancer type in the Caucasian population. The non-melanoma tumors may originate from squamous or basal cells. These cells in the skin occasionally change and do not behave normally, resulting in precancerous conditions. As a consequence, there is a high chance that these abnormal cells will become cancerous (11). MSC is a result of the transformation of skin melanocytes. At present, MSC is the most common tumor diagnosed in the United States and numerous other countries, and NMSC and MSC cases have each markedly increased in number over the last few decades. Melanomas represent <10% of all skin cancers, but they are responsible for the majority of skin cancer-related mortalities due to a high metastatic potential and therapeutic resistance (9,12,13). Previous studies demonstrated that risk factors for cutaneous melanoma depended upon the anatomical site and the clinicopathological variant (14), and that there was an inverse association between vitamin D blood levels and cutaneous thickness melanoma at diagnosis (15).
The associations among skin type IV, the time to induce solar erythema (TEry) and the time required to produce 1,000 IU vitamin D (TVitD) have previously been studied in Arica, a city located in the northern region of Chile, close to the equator and surrounded by desert and ocean (16,17). The association between skin cancer rates per 100,000 inhabitants and the solar UV index (UVI) was previously studied between 2001 and 2006 in this city (18), and between 2007 and 2011 with latitude variation (19). The most common skin types in Chile have been found to be type III for women and type IV for men (20). The skin type is expressed as the number of standard erythema doses (SED) according to the Fitzpatrick skin type classification; skin type III for women (3–5 SED) induced erythema type III in Caucasian skin, whereas skin type IV for men (4.5–6 SED) induced type IV in Mediterranean skin (21). Vitamin D is formed mainly in the skin upon exposure to UVB and it is taken orally with food or through supplements (14,22–24). Since sun exposure is a known factor for skin cancer development, the aim of the present study was to analyze the association between NMSC and MSC rates, and solar UVI data obtained from 6 different cities in Chile ranging from latitude 18 to 53°S.
Materials and methods
Measurements
Solar UVI measurements were obtained using a YES-UVB-1 UV biometer (Yankee Environmental Systems, Inc., Turners Falls, MA, USA), according to the manufacturer's instructions (25), in the Solar Ultraviolet Laboratory of Tarapaca University in Arica, Chile. The data provided by this instrument included the latitude, longitude and altitude, as well as the ozone layer and cloudiness for each location. This laboratory is run in agreement with and as part of the Chilean Meteorological Organization network. This instrument is calibrated in accordance with their recommendations. It is accepted that solar UVI fluctuates from 1 to 11 according to the World Meteorological Organization. An algorithm developed by McKenzie et al (26) was used to calculate the TVitD from experimental measurements of solar UVI in different cities. The minimal erythema dose (MED) is the minimum amount of UV that produces redness 24 h after exposure, where one MED is equal to 240 J/m2 of UV doses required to induce erythema (27), according to the Fitzpatrick skin type classification (21). The Tery in unprotected skin (only hands and face, i.e., 10% of the body) was calculated using the following equation:
The amount of UV solar radiation to induce erythema (UVery) was directly obtained from the following equation [where the unit for UVery is milliwatt (mW) divided by square meters (m2)]:
Population data
The NMSC ratio was calculated in males and females for each city in comparison to Punta Arenas. NMSC and MSC rates were considered for each location and the data for skin cancer rate normalized by patient age was obtained between 2005 and 2007 from the Ministerio de Salud (Ministry of Health) of Chile, where open access to cancer population data has been established by Resolution number 23.01.2002, therefore Ethics/guidelines must be considered in each hospital of Chile.
Statistical analysis
Statistical analysis was performed using standard statistical criteria, and correlations were assessed by evaluating the quotient between covariance and standard deviation for each variable. Pearson's linear correlation was used for statistical purposes. Statistical analysis performed using StatDisk software (version 12.0.2; Pearson plc., London, UK). P<0.05 was considered to indicate a statistically significant difference.
Results
The present study considered solar UVI measurements, NMSC and MSC rates, mortality rates per 100,000 inhabitants and the association with the time required to synthesize adequate levels of vitamin D in different geographical locations of Chile. TVitD was calculated to explain the association between NMSC and MSC rates in 6 cities in Chile between latitude 18 and 53°S. The monthly averages of the TVitD were calculated from the maximum UVI daily values obtained from Arica, Antofagasta, Santiago, Concepción, Valdivia and Punta Arenas, with latitudes of 18, 23, 33, 36, 39 and 53°S, respectively. Fig. 1 shows the mean solar UVI per month considering the maximum value for each day (at noon) and the latitude of these cities between January and December. Solar UVI values fluctuated from a minimum in winter (June) to a maximum in summer (January), recorded as 5.6–12.3 in Arica, 3.7–11.7 in Antofagasta, 2.0–11.8 in Santiago, 1.7–10.7 in Concepción, 1.1–10.9 in Valdivia and 0.4–6.9 in Punta Arenas.
Figure 1.
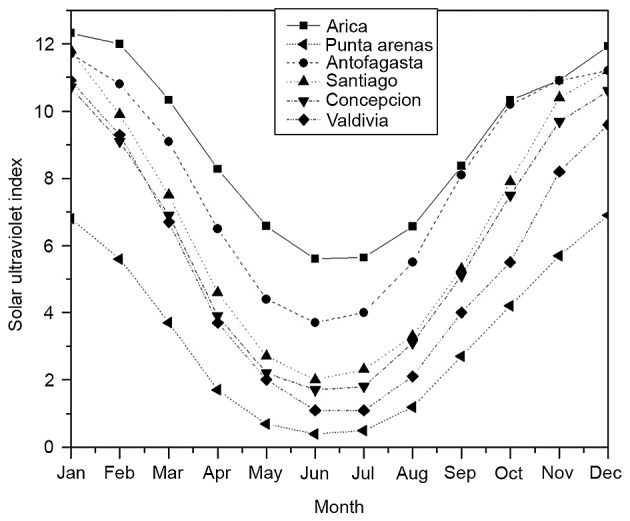
Solar ultraviolet index per month obtained in several cities of Chile between January and December.
Tables I–III show solar UVI data, and NMSC and MSC rates from different geographical locations in Chile. Table I presents latitude, longitude and altitude, and solar UVI data per year, from the following geographical locations in Chile: Arica, Antofagasta, Santiago, Concepción, Valdivia and Punta Arenas. Table II presents NMSC and MSC mortality rates per 100,000 inhabitants in the same locations as aforementioned between 1990 and 2005, while Table III presents NMSC and MSC rates in males and females in these cities between 2003 and 2007 (28). Data from Table III is also shown in Fig. 2A and B. The results indicated that the NMSC rates in males and females were greater in the northern cities of Chile, such as Arica and Antofagasta, compared with the rate in cities located farther south, such as Concepción and Valdivia (Fig. 2A). Fig. 2B shows MSC rates in males and females from Arica to Punta Arenas; the data indicated that the rate of MSC was lower in females than males in Arica and in cities located farther south, such as Santiago, Concepción and Valdivia. An inverse association was observed between NMSC and latitude in males and females, as observed at 18°S in Arica and 36°S in Concepción (Fig. 2C); thus rates decreased as latitude increased. Fig. 2D shows that the MSC rates in males and females increased as latitude increased (23 and 40°S), with the exception of Punta Arenas (53°S), in which the MSC rates in males and females decreased.
Table I.
Latitude, longitude, altitude and solar UVI data per year in different geographical locations of Chile.
| City | Latitude | Longitude | Altitude, m | Solar UVI data, years |
|---|---|---|---|---|
| Arica | 18°18′S | 70°18′W | 25 | 2006–2013 |
| Antofagasta | 23°38′S | 70°24′W | 40 | 1997–2005 |
| Santiago | 33°23′S | 70°47′W | 475 | 2004–2009 |
| Concepción | 36°46′S | 73°03′W | 8 | 2003–2007 |
| Valdivia | 39°48′S | 73°14′W | 9 | 2001–2004 |
| Punta Arenas | 53°00′S | 70°51′W | 37 | 2001–2005 |
UVI, ultraviolet index.
Table III.
NMSC and MSC rates per 100,000 individuals in males and females between 2003 and 2007 (28).
| NMSC rate | MSC rate | |||
|---|---|---|---|---|
| City | M | F | M | F |
| Arica | 69.7 | 52.4 | 3.7 | 1.2 |
| Antofagasta | 55.5 | 46.7 | 2.1 | 2.1 |
| Santiago | 24.7 | 16.5 | 2.9 | 2.5 |
| Concepción | 20.9 | 19.5 | 3.4 | 2.5 |
| Valdivia | 19.7 | 21.4 | 3.6 | 2.5 |
| Punta Arenas | 22.8 | 29.4 | 0.8 | 0.9 |
MSC, melanoma skin cancer; NMSC, non-MSC; M, male; F, female.
Table II.
NMSC and MSC mortality rates per 100,000 individuals between 1990 and 2005 (28).
| City | NMSC | MSC |
|---|---|---|
| Arica | 1.07 | 0.54 |
| Antofagasta | 1.89 | 0.75 |
| Santiago | 0.75 | 1.00 |
| Concepción | 0.84 | 1.07 |
| Valdivia | 0.57 | 0.82 |
| Punta Arenas | 0.89 | 1.21 |
MSC, melanoma skin cancer; NMSC, non-MSC.
Figure 2.

(A) NMSC and (B) MSC rates in 6 cities, and (C) NMSC and (D) MSC rates at different latitudes in males and females in Chile. MSC, melanoma skin cancer; NMSC, non-MSC.
In Chile, the most common skin types are type III for women that tan moderately and uniformly, with an MED of 0.30–0.50 kJ/m2, and skin type IV for men with corresponding light brown skin that tans minimally, moderately and easily with an MED of 0.40–0.60 kJ/m2 (27). Fig. 3 shows the TVitD in 6 cities of Chile every month. The maximum values were observed in June (winter) and varied from 18–700 min in Arica and Punta Arenas, respectively.
Figure 3.
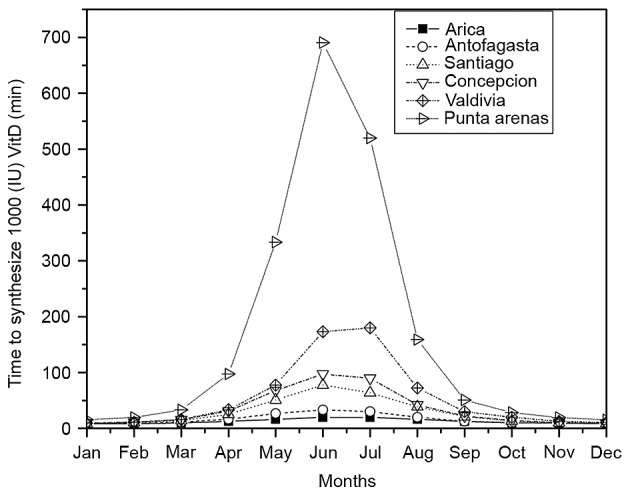
Exposure time to synthesize 1,000 IU vitamin D (min) in 6 cities of Chile per month.
Fig. 4A-B shows NMSC and MSC mortality rates with regard to latitude and TVitD accumulated over 1 year. Fig. 4A shows that there was a negative correlation between NMSC mortality rates and latitude (r=−0.53), and no correlation between NMSC mortality rate and TVitD accumulated in 1 year (r=−0.25). A strong correlation was also found between MSC mortality rates and latitude (r=0.88), and between MSC and TVitD accumulated over 1 year (r=0.72), as shown in Fig. 4B. The NMSC ratio was calculated in males and females for each city in comparison to Punta Arenas. This was found to be 3.1 and 1.8 in Arica, 2.4 and 1.6 in Antofagasta, 1.1 and 0.6 in Santiago, 0.9 and 0.7 in Concepción, and 0.9 and 0.7 in Valdivia, respectively. This was probably due to the low solar UVB radiation levels in the southern cities of Chile in winter (June 21 to September 20). The MSC ratio was calculated for each city in comparison to Punta Arenas in males and females. This was found to be 4.6 and 1.3 in Arica, 2.6 and 2.3 in Antofagasta, 3.6 and 2.8 in Santiago, 4.3 and 2.8 in Concepción, and 4.5 and 2.8 in Valdivia, respectively.
Figure 4.

(A) NMSC and (B) MSC mortality rate and mean TVitD accumulated over 1 year with respect to latitude. MSC, melanoma skin cancer; NMSC, non-MSC; TVitD, exposure time to synthesize 1,000 IU vitamin D.
Discussion
The dose-response associations between vitamin D and cancer risk reduction have been previously estimated, and data has indicated that it takes 1,500 IU vitamin D3 per day to obtain a 29% cancer risk reduction for male cancer mortality rates in the United States (29). The present study provides an analysis of solar UVI levels reported in 6 cities from the north to the south of Chile in different months. The results showed that the solar UVI ratio of monthly mean values was 1.8 times higher in Arica than in Punta Arenas in January (summer in Chile), whereas it was 14 times higher in June (winter in Chile). This factor is an important consideration since vitamin D synthesis is directly associated with the exposure of individuals to solar UVB radiation. A similar trend was observed in Antofagasta, Santiago, Concepcion, Valdivia and Punta Arenas.
Therefore, high solar UVB radiation levels imply a great capability to synthesize vitamin D in the northern regions of Chile. A recent analysis determined that the diagnosis of NMSC was associated with a reduced risk of several vitamin D-sensitive cancers (30,31). This was in accordance with low solar UVB radiation levels in the southern cities of Chile in winter. Therefore, high solar UVB radiation levels imply a lower capability to synthesize vitamin D in the southern regions of Chile than in the northern regions. Melanoma is another cancer that has been linked to solar UV irradiance. However, it has been associated with sun burning, limited solar UV irradiance (32), solar UVA irradiance (24,33,34), low dietary vitamin D intake (35) and a lack of chronic solar UVB irradiation at higher latitudes (36,37).
An inverse correlation was found between NMSC rates in males and females, and different latitudes of 18°S in Arica and 36°S in Concepción. NMSC rates decreased as latitude increased, which was in accordance with the low UVI values measured in those cities. There was a strong inverse correlation coefficient between NMSC rate and latitude (r=−0.84) among males, whereas there was a weak inverse correlation in females (r=−0.65). The NMSC rate in males in Punta Arenas was similar to the rates in Santiago and Concepcion, however, this rate was higher in females. NMSC appears to be directly associated with the Caucasian type of skin, that is, types II and III. It is notable that the population from Punta Arenas has a Croatian origin, with skin types II and III (50% of the population according to the Republic of Croatia State Office for Croats Abroad) (38). NMSC is the most common malignant neoplasm in fair-skinned people, and in a number of sunny countries this frequency exceeds the total number of all other neoplasms. The incidence of basal cell carcinoma is always greater than that of squamous cell carcinoma, varying by latitude from 10:1 to 2.5:1 (39). Studies have also indicated that NMSC has been increasing by 2–3% per year, at least in the United States, which is most likely caused by greater outdoor exposure for leisure and social reasons.
The results of the present study indicated that MSC decreased between latitude 18°S (Arica) and 23°S (Antofagasta) in males. MSC rates increased between latitude 23°S (Antofagasta) and 40°S (Valdivia) in males and females. However, MSC rates decreased at higher latitudes in each gender; this trend is consistent with the reported annual doses of UVA radiation, which decreased with increasing latitude (24).
There was a weak inverse coefficient correlation between MSC rate and latitude (r=−0.56) among males, and none (r=−0.12) in females. TVitD was similar in Arica, Antofagasta, Santiago and Concepción, with maximum values that varied from 175 to 700 min in Valdivia and Punta Arenas in winter, and where TvitD was 39 times higher in Punta Arenas than in Arica.
There was a weak inverse correlation coefficient between NMSC mortality rates and latitude (r=−0.53). However, there was a strong correlation between MSC mortality rates and latitude (r=0.88). Mortality rate and TVitD accumulated in 1 year were analyzed. Results showed that there was no correlation between NMSC and TVitD accumulated in 1 year. However, there was a strong correlation between MSC mortality rates and TVitD accumulated over the same period (r=0.72). In Punta Arenas, the MSC mortality rate was higher despite a lower MSC incidence.
When explaining the lack of correlation between different skin cancers and sunny cities, such as Arica, and less sunny cities, such as Punta Arenas, there are several aspects to take into consideration; for example, less body exposure to solar UVB, which thereby reduces the amount of vitamin D production (23,40), and lower UVB doses. The low risk for skin cancers in dark-skinned individuals is partly attributable to the photo-protection provided by the epidermal melanin barrier, which halves the penetration of UVB through the epidermis in black people compared with that in those of individuals of white European ethnicity (Caucasians, corresponding to type I and type II skin classification) (41). One study previously reported a comprehensive bibliographic search of the literature that identified studies on cutaneous malignant melanomas and non-melanomas, vitamin D receptor polymorphisms, vitamin D intake and 25(OH) D serum levels. An association was found for two types of polymorphisms and melanoma (42). It can be concluded from these studies that there is a direct correlation between NMSC rates and mortality with UVB radiation, meaning that this type of cancer would not depend on vitamin D synthesis and therefore on calcium uptake; by contrast, MSC rates increased with decreased levels of vitamin D and thus calcium uptake in all cities, with the only exception being Punta Arenas.
Acknowledgements
This study was supported by grants from Tarapacá University, Arica, Chile (Grant UTA-Mayor-4728-2016) (MR and ER) and Convenio de Desempeño UTA1117 (GMC). The authors would like to thank Mr. Leodán A. Crispin for his suggestions and the Chilean Metereological Organization (Santiago, Chile).
References
- 1.Engelsen O. The relationship between ultraviolet radiation exposure and vitamin D status. Nutrients. 2010;2:482–495. doi: 10.3390/nu2050482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Holick MF. The use and interpretation of assays for vitamin D and its metabolites. J Nutr. 1990;120:S1464–S1469. doi: 10.1093/jn/120.suppl_11.1464. (Suppl 11) [DOI] [PubMed] [Google Scholar]
- 3.Matsuoka LY, Wortsman J, Haddad JG, Kolm P, Hollis BW. Racial pigmentation and the cutaneous synthesis of vitamin D. Arch Dermatol. 1991;127:536–538. doi: 10.1001/archderm.1991.04510010104011. [DOI] [PubMed] [Google Scholar]
- 4.Porojnicu AC, Lagunova Z, Robsahm TE, Berg JP, Dahlback A, Moan J. Changes in risk of death from breast cancer with season and latitude: Sun exposure and breast cancer survival in Norway. Breast Cancer Res Treat. 2007;102:323–328. doi: 10.1007/s10549-006-9331-8. [DOI] [PubMed] [Google Scholar]
- 5.Matsuoka LY, Wortsman J, Dannenberg MJ, Hollis BW, Lu Z, Holick MF. Clothing prevents ultraviolet-B radiation-dependent photosynthesis of vitamin D3. J Clin Endocrinol Metab. 1992;75:1099–1103. doi: 10.1210/jcem.75.4.1328275. [DOI] [PubMed] [Google Scholar]
- 6.McKenna MJ. Differences in vitamin D status between countries in young adults and the elderly. Am J Med. 1992;93:69–77. doi: 10.1016/0002-9343(92)90682-2. [DOI] [PubMed] [Google Scholar]
- 7.Edvardsen K, Brustad M, Engelsen O, Aksnes L. The solar UV radiation level needed for cutaneous production of vitamin D3 in the face. A study conducted among subjects living at high latitude (68 degrees N) Photochem Photobiol Sci. 2007;6:57–62. doi: 10.1039/B613263D. [DOI] [PubMed] [Google Scholar]
- 8.Casado J, Parra P, Vega L, Suárez C. Relación entre hormona paratiroidea y riesgo cardiovascular en pacientes con insuficiencia de vitamina D. Med Clin. 2013;141:292–294. doi: 10.1016/j.medcli.2013.02.039. [DOI] [PubMed] [Google Scholar]
- 9.Miller DL, Weinstock MA. Non-melanoma skin cancer in the United States: Incidence. J Am Acad Dermatol. 1994;30:774–778. doi: 10.1016/S0190-9622(08)81509-5. [DOI] [PubMed] [Google Scholar]
- 10.Cannell JJ, Vieth R, Umhau JC, Holick MF, Grant WB, Madronich S, Garland CF, Giovannucci E. Epidemic influenza and vitamin D. Epidemiol Infect. 2006;134:1129–1140. doi: 10.1017/S0950268806007175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Lucena SR, Salazar N, Gracia-Cazaña T, Zamarrón A, González S, Juarranz A, Gilaberte Y. Combined treatments with photodynamic therapy for non-melanoma skin cancer. Int J Mol Sci. 2015;16:25912–25933. doi: 10.3390/ijms161025912. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Houghton AN, Polsky D. Focus on melanoma. Cancer Cell. 2002;2:275–278. doi: 10.1016/S1535-6108(02)00161-7. [DOI] [PubMed] [Google Scholar]
- 13.Donaldson MR, Coldiron BM. No end in sight: The skin cancer epidemic continues. Semin Cutan Med Surg. 2011;30:3–5. doi: 10.1016/j.sder.2011.01.002. [DOI] [PubMed] [Google Scholar]
- 14.Caini S, Gandini S, Sera F, Raimondi S, Fargnoli MC, Boniol M, Amstrong BK. Meta-analysis of risk factors for cutaneous melanoma according to anatomical site and clinic-pathological variant. Eur J Cancer. 2009;45:3054–3063. doi: 10.1016/j.ejca.2009.05.009. [DOI] [PubMed] [Google Scholar]
- 15.Caini S, Boniol M, Bazolli E, Tosti G, Bazolli B, Russel-Edu W, Giusti F, Testori A, Gandini S. The risk of developing a secondary primary cancer in melanoma patients: A comprehensive review of the literature and meta-analysis. J Dermatol Sci. 2014;75:3–9. doi: 10.1016/j.jdermsci.2014.02.007. [DOI] [PubMed] [Google Scholar]
- 16.Rivas M, Rojas E, Calaf GM. Prediction of skin cancer occurrence by ultraviolet solar index. Oncol Lett. 2012;3:893–896. doi: 10.3892/ol.2012.580. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Rivas M, Rojas E, Araya MC, Calaf GM. Ultraviolet light exposure, skin cancer risk and vitamin D production. Oncol Lett. 2015;10:2259–2264. doi: 10.3892/ol.2015.3519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rivas M, Araya MC, Durán V, Rojas E, Cortes J, Calaf GM. Ultraviolet light exposure and skin cancer in the city of Arica, Chile. Mol Med Rep. 2009;2:567–572. doi: 10.3892/mmr_00000138. [DOI] [PubMed] [Google Scholar]
- 19.Rivas M, Araya MC, Caba F, Rojas E, Calaf GM. Ultraviolet light exposure influences skin cancer in association with latitude. Oncol Rep. 2011;25:1153–1159. doi: 10.3892/or.2011.1164. [DOI] [PubMed] [Google Scholar]
- 20.Zemelman V, Alvarado O, Von Beck P, Valenzuela C. Assessment of skin type, eye and hair color, freckles tendency in Chilean adolescents. J Eur Acad Dermatol Venereol. 1990;12:321. [Google Scholar]
- 21.Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869–871. doi: 10.1001/archderm.1988.01670060015008. [DOI] [PubMed] [Google Scholar]
- 22.Grant WB. An ecologic study of cancer mortality rates in Spain with respect to indices of solar UVB irradiance and smoking. Int J Cancer. 2007;120:1123–1128. doi: 10.1002/ijc.22386. [DOI] [PubMed] [Google Scholar]
- 23.Grant WB. The effect of solar UVB doses and vitamin D production, skin cancer action spectra, and smoking in explaining links between skin cancers and solid tumours. Eur J Cancer. 2008;44:12–15. doi: 10.1016/j.ejca.2007.09.009. [DOI] [PubMed] [Google Scholar]
- 24.Grigalavicius M, Moan J, Dahlback A, Juzeniene A. Daily, seasonal, and latitudinal variations in solar ultraviolet A and B radiation in relation to vitamin D production and risk for skin cancer. Int J Dermatol. 2016;55:e23–e28. doi: 10.1111/ijd.13065. [DOI] [PubMed] [Google Scholar]
- 25.Systems YES. Operation manual calibrated high range YES-Biometer. Yankee Environmental Systems, Inc; Turners Falls, OK, USA: 2006. Sep 5, 2016. Accessed. [Google Scholar]
- 26.McKenzie RL, Liley JB, Björn LO. UV radiation: Balancing risks and benefits. Photochem Photobiol. 2009;85:88–98. doi: 10.1111/j.1751-1097.2008.00400.x. [DOI] [PubMed] [Google Scholar]
- 27.Holick MF. Biologic effects of light: Historical and new perspectives. In: Holick MF, Jung EG, editors. Biologic effects of light 1998. Boston: Kluwer Academic Publishers; 1999. pp. 11–32. Proceedings of a symposium Basel, Switzerland November 1–3, 1998. [DOI] [Google Scholar]
- 28.Vallebuono C. Primer informe de registros poblacionales de cáncer de Chile, quinquenio 2003–2007, unidad de vigilancia de enfermedades no transmisibles y estudios. Ministry of Health of Chile. Epidemiology Section. 2012 [Google Scholar]
- 29.Giovannucci E, Liu Y, Rimm EB, Hollis BW, Fuchs CS, Stampfer MJ, Willett WC. Prospective study of predictors of vitamin D status and cancer incidence and mortality in men. J Natl Cancer Inst. 2006;98:451–459. doi: 10.1093/jnci/djj101. [DOI] [PubMed] [Google Scholar]
- 30.De Hertog SA, Wensveen CA, Bastiaens MT, Kielich CJ, Berkhout MJ, Westendorp RG, Vermeer BJ, Bavinck Bouwes JN. Leiden Skin Cancer Study: Relation between smoking and skin cancer. J Clin Oncol. 2001;19:231–238. doi: 10.1200/JCO.2001.19.1.231. [DOI] [PubMed] [Google Scholar]
- 31.Milán T, Verkasalo PK, Kaprio J, Koskenvuo M. Lifestyle differences in twin pairs discordant for basal cell carcinoma of the skin. Br J Dermatol. 2003;149:115–123. doi: 10.1046/j.1365-2133.2003.05352.x. [DOI] [PubMed] [Google Scholar]
- 32.Garland FC, White MR, Garland CF, Shaw E, Gorham ED. Occupational sunlight exposure and melanoma in the U.S. Navy. Arch Environ Health. 1990;45:261–267. doi: 10.1080/00039896.1990.10118743. [DOI] [PubMed] [Google Scholar]
- 33.Moan J, Dahlback A, Setlow RB. Epidemiological support for an hypothesis for melanoma induction indicating a role for UVA radiation. Photochem Photobiol. 1999;70:243–247. doi: 10.1111/j.1751-1097.1999.tb07995.x. [DOI] [PubMed] [Google Scholar]
- 34.Garland CF, Garland FC, Gorham ED. Epidemiologic evidence for different roles of ultraviolet A and B radiation in melanoma mortality rates. Ann Epidemiol. 2003;13:395–404. doi: 10.1016/S1047-2797(02)00461-1. [DOI] [PubMed] [Google Scholar]
- 35.Millen AE, Tucker MA, Hartge P, Halpern A, Elder DE, Guerry D, VI, Holly EA, Sagebiel RW, Potischman N. Diet and melanoma in a case-control study. Cancer Epidemiol Biomarkers Prev. 2004;13:1042–1051. [PubMed] [Google Scholar]
- 36.Berwick M, Armstrong BK, Ben-Porat L, Fine J, Kricker A, Eberle C, Barnhill R. Sun exposure and mortality from melanoma. J Natl Cancer Inst. 2005;97:195–199. doi: 10.1093/jnci/dji411. [DOI] [PubMed] [Google Scholar]
- 37.Gandini S, Sera F, Cattaruzza MS, Pasquini P, Picconi O, Boyle P, Melchi CF. Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure. Eur J Cancer. 2005;41:45–60. doi: 10.1016/j.ejca.2004.10.015. [DOI] [PubMed] [Google Scholar]
- 38.http://www.hrvatiizvanrh.hr/en/hmiu/croatian-diaspora-in-chile/22. Republic of Croatia State Office for Croats Abroad. 2016 Sep 5; 2013–2016. Accessed. [Google Scholar]
- 39.Urbach F. Incidence of nonmelanoma skin cancer. Dermatol Clin. 1991;9:751–755. [PubMed] [Google Scholar]
- 40.Webb AR, Engelsen O. Calculated ultraviolet exposure levels for a healthy vitamin D status. Photochem Photobiol. 2006;82:1697–1703. doi: 10.1562/2006-09-01-RA-670. [DOI] [PubMed] [Google Scholar]
- 41.Brenner M, Hearing VJ. The protective role of melanin against UV damage in human skin. Photochem Photobiol. 2008;84:539–549. doi: 10.1111/j.1751-1097.2007.00226.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Gandini S, Raimondi S, Gnagnarella P, Doré JF, Maisonneuve P, Testori A. Vitamin D and skin cancer: A meta-analysis. Eur J Cancer. 2009;45:634–641. doi: 10.1016/j.ejca.2008.10.003. [DOI] [PubMed] [Google Scholar]