

Summary
Background.
In Vietnam today, many generations remain living together in a family. With escalating urbanization and population aging, mental health disorders and the quality of life (QoL) among the elderly are gradually presenting themselves as of great concern. The objective of this study was to examine gender differences in QoL and some associated factors among the elderly in rural Vietnam using the QoL scale of WHO (WHOQOL-BREF).
Methods.
A cross-sectional study using quantitative methods.
Results and Conclusions.
The proportion of the elderly men having higher level of QoL in physical health, psychological health and environment was higher than that of their women counterparts. Reversely, of those having medium and lower QoL, females made up a larger proportion than males. The overall QoL score in elderly men (75.32) was higher than that of women (72.32) and the same pattern was witnessed in all four domains of QoL. While higher QoL in elderly men was significantly correlated with 5 factors, aged ≥ 80 years, following Buddhism and Christianity, having better connection and without illness in the past 6 months, these among female counterparts are aged ≥ 80 years, completing secondary level or above, having medium and high socioeconomic status and without illness in the last 6 months.
Key words: Quality of life, Elderly, Gender differences, Related factors, Vietnam
Introduction
Recently, Vietnam has witnessed an increasing aged population. According to the United Nations Population Fund (UNFPA), the elderly population in Vietnam, which increased from 3.71 million (1979) to 7.72 million (2009), is anticipated to reach 12 million people in 2020 [1]. It is concerned that this rapid growth may present great challenges to the provision of social services, including health care for older people. It is also worth noting the sensitive nature of the elderly's mental life. With the passing of time, Vietnamese seniors are increasingly prone to negative feelings, regarding themselves as onerous burdens to their descendants. Some people, after retirement, tend to feel lost and shunted sideways by the society. For this reason, the elderly are among susceptible age groups that should be attended to not only physically, but also emotionally. Considering the profound influence of quality of life (QoL) upon their well-being, the research on QoL among the elderly in a continuously changing context will provide significant inputs for designing and implementing appropriate policies and programs with regard to the enhancement of their QoL. The change of the quantity and structure of the elderly leads to changes of disease pattern, including changes of quality of life. Biological differences between elderly men and elderly women also have gender differences in quality of life.
Despite numerous prior studies on QoL in general among the elderly, few interesting studies on gender differences have been found. For instance, a study among the elderly in rural Thailand [2] indicated that more elderly females reported lowest and medium QoL than men, while more men reported highest QoL. Another study among the elderly living in rural and urban India showed while there was no gender difference in average score of QoL in three domains, physical health, psychological health and social relationships, a statistically significant difference in environmental QoL was detected with the average score of elderly men higher than that of women [3]. QoL among the elderly in general is subject to many factors. According to Mudey [3], a number of factors were associated with low QoL among the Indian elderly, separation from a spouse, poor socioeconomic status, lack of regular exercise, sleeping or hearing difficulty, suffering one kind of illness and history of a fall within the last 6 months. In Nigeria, traditional lifestyle, educational level, socioeconomic status, gender and marital stability were closely related to QoL of many senior citizens [4]. In addition, environment is also among the major determinants of high QoL. Living in a crowded environment had a negative impact on individuals' health status and QoL in the future [5, 6]. The role of other factors, recreational activities, job satisfaction and life security [5] was also important. A review by Djernes revealed that lack or loss of closeness and intimacy in social contacts were likely to predict depression and low QoL among the elderly [7]. In a study comparing QoL among senior citizens in Vietnam and Bangladesh, factors such as socioeconomic status, living environment, social relations, religion and beliefs are intimately associated with health and QoL [8]. Still, there is insufficient evidence available regarding gender differences in QoL of the elderly [9, 10] and little has been known about factors associated with QoL among each group of gender, male and female elderly.
Although QoL in Vietnam remained relatively lower compared to other countries in the world (116/182 countries), it ranked 4th in Southeast Asia and Association of South-East Asian Nations (ASEAN) after Laos, Cambodia and Myanmar [11]. However, the QoL among the elderly up to date remains in question, although there are some prior data on this regard. For instance, in 2009 when evaluating just the instrument for measuring QoL in Vietnam, Huong et al. revealed a higher average score of QoL in elderly men than elderly women [12]. Another study of Xoan in 2012 showed the similar pattern with more women reporting lower and medium QoL versus more men reporting higher QoL [13]. A study by Hoi et al. on QoL of 600 seniors in rural district of Hanoi, Vietnam using European scale of QoL (EQ-5D Index) also revealed a higher average score of QoL in elderly men than elderly women [14]. Although some of the prior studies as mentioned suggested differences in QoL between elderly men and women, these differences along with QoL related factors have not been elaborated. Moreover, inconsistency in using the WHO scale of QoL might impede the comparison and evaluation to a certain degree. A study about QoL among people aged 50+ years by Ninh Thi Ha et al., WHOQOL-BREF is a reliable instrument to measure QoL among hypertensive patients. The results revealed low QoL in psychological domain and inequality in QoL across socio-demographic characteristics [15].
Given limitations of previous research on gender differences in QoL, the purpose of this study was to examine gender differences in QoL and factors associated with it by gender in rural district of Thai Binh province, Vietnam. A conceptual model for this research was based on a model by Kamp et al. (Fig. 1). This theoretical framework consists of six factors influencing health, security, physical environment, personal development, resources and community development as contributors to QoL [16]. We used this model of Kamp et al. in our study because it is relatively comprehensive and applicable to many research subjects including older people. As we used in the elderly population, it is necessary to adapt it, especially in rural setting of developing countries. The factors used in adapting the Kamp model were identified based on the previous research in people living in rural areas of some European countries [16]. In the current context of Vietnam, we focused on a number of factors, health (mental health and physical health); physical environment; natural resources; goods and services; community development; and personal development.
Fig. 1.
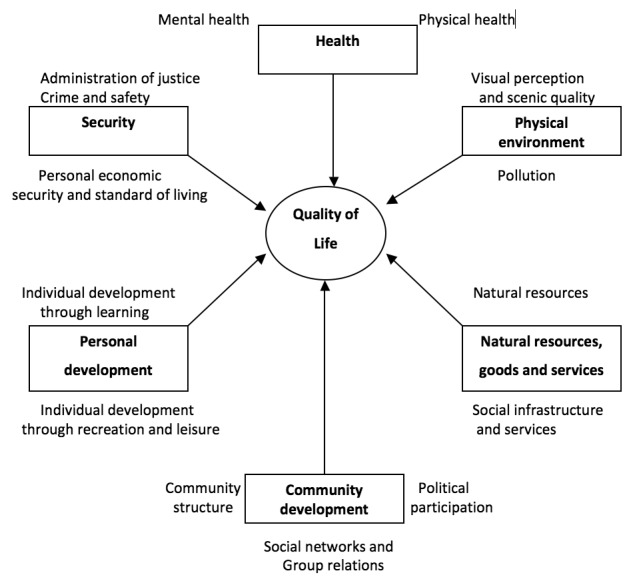
Theoretical model of some QoL related factors in the elderly.
Methods
DESIGN
This is a cross-sectional study adopting quantitative method with face-to-face interviews using WHO instruments to measure QoL, WHOQOL-BREF [17].
SITES AND SAMPLING
The study was carried out in three communes of Kien Xuong district in Thai Binh province. Thai Binh is the granary of Northern Vietnam, one of the strategic provinces in the national target program on new rural construction which has achieved encouraging successes in improving living standards in rural areas. Kien Xuong is an agricultural district in Thai Binh province. With a large area of 200 km2, it is located in the north west of Thai Binh city, consisting of one town and 36 communes. Its population was 274,318 people in 2012, including 34,898 senior citizens [18]. We chose these communes for the study because they could represent a typical rural community in Vietnam such as income sources mainly from agriculture, an increasing number of the elderly people, and quite far from urban setting; they also have received limited support and interventions to improve QoL of the elderly over the past decades [19].
Participants were screened if they were elderly aged 60 years or more, living in the selected area for at least 5 years, being available at the time of the survey and willing to participate voluntarily in the survey. The sample size was generated based on the sample formula to test the difference between the proportion of elderly males and females in QoL:
Where: p1 is the percentages of higher QoL among elderly men and women, respectively. In a previous study in Myanmar in 2010, p1 was 0.218 and p2 was 0.135 [20]; (P1-P2) is the desired relative precision higher QoL between elderly men and elderly women. The desired precision in our study was set at 0.30; a is the significant level and the probability of making type I error (reject the null hypothesis H0 when it is true). Take a = 0.05 with the 95% confidence interval, and b is the probability of making type II error (accept H0 when it is false) take b = 0.1. Then (Z(a,b))2 = 10.8
Using these above values, a sample size of 402 elderly subjects were calculated.
Applying systematic random sampling technique the study subjects were chosen in two phases: phase 1, sample 3 communes in Kien Xuong district from Thai Binh province, and phase 2, select the number of participants in each commune using by systematic random sampling. From the data provided by People's Committee in three communes: make a list of the elderly, then identify kinterval in each commune (average of k-interval = 4).
Measurement
DEPENDENT VARIABLE
QoL: Given the prior literature, there have been quite numerous QoL measures widely studied. Of the QoL measures, the Quality of life Instruments developed by WHO (WHOQOL-BREF) has been one of the most widely used tools in QoL research as it is able to assess individual perceptions in the context or their culture, personal goals, standards and concerns [9, 21] as well as has been widely field-tested and validated [22, 23]. We adopted his tool as it was developed for international cross-culturally comparable QoL evaluation and have been widely field-tested [22, 23].
In our current study, when examined for internal consistency, with 26 items, the WHOQOL-BREF instrument was of relatively high consistency [Cronbach's alpha (a) = 0.89, and each item presents one facet of QoL and two "benchmark" items for an individual's overall QoL and general health]. The facets were defined as aspects of life considered to have contribution to a person's QoL. QoL comprised four main domains-physical health (7 items, a = 0.73), psychological health (6 items, a = 0.76), social relationship (3 items, a = 0.63) and environment (8 items, a = 0.66). These facets were scored on a Likert scale of 1 to 5 with 1 = very poor, 2 = poor, 3 = neither poor or good, 4 = good and 5 = very good; and 1 = very satisfied, 2 = dissatisfied, 3 = neither dissatisfied or satisfied, 4 = satisfied and 5 = very satisfied; 1 = not at all, 2 = a little, 3 = a moderate amount, 4 = very much and 5 = extremely; or 1 = never, 2 = seldom, 3 = quite often, 4 = very often and 5 = always.
If the use of scores obtained in the WHOQOL-BREF domains is a goal to be pursued in this research, additional clarification of factors that influence the responses in distinct areas becomes a key objective to be explained. Therefore, categorizations of the physical, psychological, social relationships and environmental factors QoL score is necessary. The scores for the physical health assessment were divided into 3 levels: 7-16 points, low level; 17-26 points, middle level; and 27-35 points, high level QoL. The scores of the psychological health assessment were divided into 3 levels: 6-14 points, low level; 15-22 points, middle level; and 23-30 points, high level mental QoL. The scores for the social relationships assessment were divided into 3 levels: 3-7 points, low level; 8-11 points, middle level; and 12-15 points, high level of quality of social relationships. The scores of the environmental factors were divided into 3 levels: 8-18 points, low level; 19-29 points, middle level; and 30-40 points, high level environmental factors. The overall interpretation of the quality of life was divided into 3 levels: 26-60 points, low level; 61-95 points, middle level; and 96-130 points, high level QoL [24].
INDEPENDENT VARIABLES
Demographics: demographical data were collected including age groups (60-79 and ≥ 80 years old), marital status (single, divorced, widowed, and married), religion (no religion, Christianity and Buddhism); educational level (illiteracy, not completing primary level, not completing secondary level, secondary level or above), living circumstance (living with spouses, children, friends, relatives or living alone).
Social connection: the indicator of social connection was measured with seven yes/no items and is the sum of 7 variables of social engagement (retirement clubs, women's associations, veterans' associations, communist party cells, sport clubs and street population groups, religious groups). The number of organizations that an individual participated in correspondence to the number of point. As this scale was of relatively high reliability (Cronbach's α = 0.67) and of good construct validity (most of the factor loading coefficients or b's values > 0.30), we formed a composite of all items as a single common variable. In particular, a composite score was obtained by summing responses to items with higher composite scores indicating higher levels of social connection.
Socioeconomic status: it was assessed with three levels of income (low, medium and high). The classification of socioeconomic status was based on the self-reported assessment of elderly themselves.
Illness during the past 6 months: it was measured with yes/no item asking participant if she/he got ill over the past 6 months.
DATA COLLECTION
Prior to the survey, the field researchers were trained to become familiar with the key contents of research, survey methods, data collection, sampling methods, selecting study subjects, recording the responses of study subjects.
In the survey, participants were introduced about the objectives and main content so they can decide to participate voluntarily. Those who were not available at the interview time were set another appointment. Each interview lasted about 30-45 minutes. The interviews took place within 2 months from June 2013 to August 2013. During the survey, the principal investigator was present in the field to supervise data collection.
STATISTICAL ANALYSIS
Data were cleaned by checking missing data before being entered into database using Epidata software. The data continued to be cleaned for outliers and illogical data and were converted into Stata version 12.0 file for analysis.
Each item of physical health, psychological, environment and social relationships domain was scored on a Likert scale of 1 to 5. The total score of each domain was then computed to form a scale of 0 to 100 with low scores reflecting poor QoL. A domain was treated as missing when over 20.0% of its items were missing.
Both descriptive and inferential statistics were used. Means and standard deviations (SD) were for continuous variables if data are normally distributed. Percentages were presented for nominal variables. As QoL scores were normally distributed, we applied parametric tests for continuous variables. To be specific, inferential tests included t-test to compare means between groups and chi-square test to compare the gender proportions in QoL. Linear regression was used to detect the fit model. To be specific, coefficient R2, standardized b and model fit indicators were critically looked to detect factors associated with the level of the QoL among the elderly. To find a suitable model both bivariate and multiple linear regression analysis were employed. The final model was selected through a process of performing stepwise linear regression, if R2 was of great value and other indicators of model fit were met. Statistical significance was set at * p < 0.05, ** p < 0.01 and *** p < 0.001.
RESEARCH ETHICS
The research was approved by the Scientific and Education Panel from the Institute for Preventive Medicine and Public Health, Hanoi Medical University. During the survey, participants were verbally informed about the study that their participation was voluntary, that they had the right to withdraw at any point, and that data would be confidentially managed. All the respondents was anonymous in the study.
Results
KEY CHARACTERISTICS OF THE SAMPLE
In Table I, among 402 elderly people interviewed, the majority was in the age of 60-69 groups (49.8% males and 60.2% females) while those aged 80 accounted for a small proportion. Most of the elderly were nonreligious (88.1%), had completed secondary level (49.0%) and were married (67.2%). Most of the elderly were living with their families and being cared for. Previous occupations were mainly farmers. 26.1% of participants depended on their descendants, which was higher than the percentage of those having wages, salaries, and pensions and depending on their spouses. Overall, the majority of the elderly were of low and average socioeconomic status.
Tab. I.
General information of the elderly by gender.
| Characteristics (n = 402) |
Male (n1 = 201) |
Female (n2 = 201) |
General | |
|---|---|---|---|---|
| Frequency (%) | Frequency (%) | Frequency (%) | ||
| Age groups | 60-69 | 100 (49.8) | 121 (60.2) | 221 (55.0) |
| 70-79 | 70 (34.8) | 60 (29.9) | 130 (32.2) | |
| ≥ 80 | 31 (15.4) | 20 (10.0) | 51 (12.7) | |
| Religion | None | 184 (91.5) | 170 (84.6) | 354 (88.1) |
| Buddhism | 14 (7.0) | 28 (13.9) | 42 (10.4) | |
| Christianity | 3 (1.5) | 3 (1.5) | 6 (1.5) | |
| Educational level | Illiteracy | 4 (2.0) | 13 (6.5) | 17 (4.2) |
| Not completing primary level | 35 (17.4) | 57 (28.4) | 92 (22.9) | |
| Not completing secondary level | 49 (24.4) | 47 (23.4) | 96 (23.9) | |
| Secondary level | 75 (37.3) | 63 (31.3) | 138 (34.3) | |
| High school level | 27 (13.4) | 10 (5.0) | 37 (9.2) | |
| College or above | 11 (5.5) | 11 (5.5) | 22 (5.5) | |
| Marital Status | Single | 13 (6.5) | 16 (8.0) | 29 (7.2) |
| Divorced | 6 (3.0) | 12 (6.0) | 18 (4.5) | |
| Widowed | 26 (12.9) | 59 (29.4) | 85 (21.1) | |
| Married | 156 (77.6) | 114 (56.7) | 270 (67.2) | |
| Caregiver | Yes | 193 (96.0) | 188 (93.5) | 381 (94.8) |
| No | 8 (4.0) | 13 (6.5) | 21 (5.2) | |
| Previous occupation | None | 1 (0.5) | 3 (1.5) | 4 (1.0) |
| Farmer | 121 (60.2) | 140 (69.7) | 261 (64.9) | |
| Civil servant | 42 (20.9) | 23 (11.4) | 65 (16.2) | |
| Manual worker | 23 (11.4) | 23 (11.4) | 46 (11.4) | |
| Househusband/ housewife | 1 (0.5) | 6 (3.0) | 7 (1.7) | |
| Freelance | 8 (4.0) | 5 (2.5) | 13 (3.2) | |
| Others | 5 (2.5) | 1 (0.5) | 6 (1.5) | |
| Living circumstance | Alone | 12 (6.0) | 20 (10.0) | 32 (8.0) |
| With other people | 189 (94.0) | 181 (90.0) | 370 (92.0) | |
| Social connection | Yes | 162 (80.6) | 163 (81.1) | 325 (80.8) |
| No | 39 (19.4) | 38 (18.9) | 77 (19.2) | |
| The main source of income |
Wage/ Salary | 31 (15.4) | 29 (14.4) | 60 (14.9) |
| Personal savings | 37 (18.4) | 26 (12.9) | 63 (15.7) | |
| Pension | 59 (29.4) | 34 (16.9) | 93 (23.1) | |
| Depending on spouse | 20 (10.0) | 28 (13.9) | 48 (11.9) | |
| Depending on descendants | 39 (19.4) | 66 (32.8) | 105 (26.1) | |
| Social welfare | 15 (7.5) | 18 (9.0) | 33 (8.2) | |
| Socioeconomic status | Low | 40 (19.9) | 55 (27.4) | 95 (23.6) |
| Average | 131 (65.2) | 133 (66.2) | 264 (65.7) | |
| High | 30 (14.9) | 13 (6.5) | 43 (10.7) | |
QUALITY OF LIFE OF THE ELDERLY
In Table II, QoL of the elderly men was higher than that of women (p < 0.05). In physical health, at high QoL, the percentage of males (6.5%) was higher than that of females (0.5%); at middle and low level, the percentage of females was higher than that of males (p < 0.01). As regards psychological health, at high level, the percentage of men was higher than that of women (12.4 and 2.0%), at medium and low level, elderly women accounted for a higher percentage than elderly men (p < 0.001). However, in social domain, there was no gender difference found at all 3 levels. As for environment domain, at high level, the elderly men amounted to a higher percentage than women (12.9 and 6.5%) whereas the reverse was true at medium and low levels (p < 0.01).
Tab. II.
The distribution of QoL in the elderly by gender.
| Dimensions of QoL | Male (n1 = 201) |
Female (n2 = 201) |
p-value (chi-square) |
|---|---|---|---|
| Frequency (%) | Frequency (%) | ||
| Physical health Low Middle High |
18 (9.0) 170 (84.6) 13 (6.5) |
25 (12.4) 175 (87.1) 1 (0.5) |
** |
| Mental health Low Middle High |
21 (10.4) 155 (77.1) 25 (12.4) |
22 (10.9) 175 (87.1) 4 (2.0) |
*** |
| Social relationships Low Middle High |
10 (5.0) 143 (71.1) 48 (23.9) |
10 (5.1) 158 (78.6) 33 (16.4) |
|
| Environment Low Middle High |
3 (1.5) 172 (85.6) 26 (12.9) |
12 (6.0) 176 (87.6) 13 (6.5) |
** |
| Overall Low Middle High |
11 (5.5) 182 (90.5) 8 (4.0) |
20 (10.0) 180 (89.6) 1 (0.5) |
* |
p < 0.05;
p < 0.01;
p < 0.001.
According to Table III, the average scores of QoL in the elderly men (75.32) was overall higher than elderly women (72.32) (p < 0.01). In 3 out of 4 domains, the elderly men had higher average scores than their female counterparts (p < 0.05 and p < 0.01). However, no gender difference was found in the average score for social relationships.
Tab. III.
The distribution of scores of QoL among the elderly by gender.
| Factor (n = 402) |
Male | Female | p-value (t-test) |
|---|---|---|---|
| X ± SD | X ± SD | ||
| Physical health | 21.04 ± 3.60 | 20.04 ± 3.07 | ** |
| Psychological health | 18.84 ± 3.14 | 18.11 ± 2.84 | * |
| Social relationships | 10.26 ± 1.60 | 10.13 ± 1.53 | |
| Environment | 25.20 ± 3.53 | 24.03 ± 3.70 | ** |
| Overall | 75.32 ± 9.94 | 72.32 ± 9.21 | ** |
p < 0.05;
p < 0.01;
p < 0.001.
FACTORS ASSOCIATED WITH QOL AMONG ELDERLY MEN AND ELDERLY WOMEN
For women, factors related to better QoL included being at the age of 60-69, completing secondary level or above, previously working in the public sector, having pensions or descendants to rely on, having medium or high socioeconomic status, not widowed; having favorable social relationships and social engagement; having close social relationships, and experiencing no illness in the past 6 months. Among these factors, social relationships and social engagement and health status in the last 6 months have considerable association with QoL in both genders (with high value of standardized regression coefficient b and p < 0.001).
Table IV compares the correlation of a number of factors with QoL by gender. In both elderly men and women, those aged ≥ 80 and experienced illness in the past 6 months were more likely to have lower QoL than their younger counterparts (|b| > 0.2, p < 0.05). However, in elderly men, there were other factors associated with QoL, including Buddhism and Christianity, and having good social connection. For elderly women, completing secondary level or above, having medium and high socioeconomic status were the predictors of higher QoL.
Tab. IV.
Some factors associated with QoL in the elderly by gender (the results of multivariable analysis).
| Independent variables | Male | Female |
|---|---|---|
| Standardized regression coefficient b |
Standardized regression coefficient b |
|
| Age 60-69 70-79 ≥ 80 |
0.04 -0.2* |
-0.1 -0.3*** |
| Religion None Buddhism Christianity |
0.2** 0.13* |
0.01 -0.1 |
| Educational background Illiteracy Not completing primary level Not completing secondary level Secondary level or above |
0.0 -0.04 0.1 |
-0.02 0.14 0.31** |
| Socioeconomic status Low Average High |
0.1 0.1 |
0.17* 0.2** |
| Social connection | 0.3*** | 0.3*** |
| Illness during the past 6 months | -0.2** | -0.23*** |
| Adjusted R2 Model fit indicator (F) p |
0.523 (52.3%) 15.1 *** |
0.39 (39.0%) 6.22 *** |
p < 0.05;
p < 0.01;
p < 0.001.
Discussion
GENDER DIFFERENCES IN QOL BETWEEN ELDERLY MEN AND ELDERLY WOMEN
Our study showed that QoL of elderly men was generally higher than women and there were discernible gender differences in all four domains and thatmen displayed a higher percentage of men with high QoL than women and a higher percentage of women with low QoL than men. Our findings resemble some prior studies in both developed and developing countries. The study by Apidechkul in 2011 on elderly people in rural and suburban areas in Thailand, for instance, showed that the percentage of elderly women (2.9%) with low level of QoL was higher than men (0.0%) whereas at high level, the former was lower with 33.8% and 50.0%, respectively [2]. However, at average level, the percentage of elderly women was lower than that of elderly men [2]. Our results are also consistent with that of Huong's study in Hai Duong which indicated a higher percentage of men at high level of QoL with 3.4% compared to 2.7% of women [12]. Research conducted in Myanmar was also of the similar result with 21.8% and 13.5% respectively [20]. These similarities are possibly derived from the fact that our research was carried out in the rural setting which has the population with the same cultural, economic and environmental characteristics as those in other studies and/or in other settings.
Regarding the distribution of average points of QoL between elderly men and women, gender differences were also found. In fact, the data showed that the elderly men had higher average score than their female counterparts. This result is similar to that of previous research on rural Vietnam with 239.3 for men and 228.7 for women in Huong's study and 230.2 and 220.9 [12] respectively in Xoan's study [13]. Research of Luong in Hai Duong also revealed a higher average score in men with 64.1 ± 10.4 compared to women with 61.0 ± 10.1 (25). Some reports by Nilsson on the elderly living in rural Bangladesh also gave the similar findings (2005) [8-10].
Looking specifically at 3 dimensions of QoL (physical health, psychological health and environment), it was found that elderly men also had higher average scores than elderly women. Our results were consistent with those of Nilsson's study on QoL of seniors in rural Bangladesh [9]. This can be explained by the cultural norms that male and female roles differ in the family and society that can affect QoL. Currently in many developing countries including Vietnam, women are expected to assume two responsibilities concurrently, work commitments and home chores. They not only have their own career to handle but also have to assume the role of main caregiver at home, which exert unavoidable pressure both on their professional and personal lives to a certain extent. In Vietnam, women sometimes suffer from domestic violence, especially in rural areas, which massively affect their mental life and QoL. According to the 2010 report of General Statistics Office of Vietnam and United Nations, more than half of Vietnamese women (58%) had ever fallen victim to at least one form of domestic violence (physically, sexually and mentally) triggered by their spouses [26]. While husbands and wives both make contribution to household income, women are actually dedicated to family more than their male partners considering their contributing time and effort. Yet, most major decisions in the family are normally made by men whereas women only sort out minor issues related to housework and caregiving. Our results also resemble those of the research of Mudey et al. on average scores of QoL among Indian elderly [3]. This resemblance is explainable as both Vietnam and India located in Southern East Asia share many similarities in socioeconomic status, cultural characteristics and living environment. Due to this high profile of gender differences in QoL among the elderly, it is crucial to understand what factors would affect determine QoL in each gender.
FACTORS ASSOCIATED WITH QOL IN ELDERLY MEN AND ELDERLY WOMEN
According to the result of multivariate linear regression, it was identified that predictors of QoL differed between elderly women and men. Yet, in both sexes, those who belonged to the oldest age group (aged 80 and above) and experienced illness in the past 6 months had higher QoL than other elderly. The common tendency is that aging is very often accompanied by impaired health, increased vulnerability to ailments, and fewer opportunities for social engagement, which in turn lead to a decrease in QoL. Some other studies in the world also accentuated the influence of health on the QoL of the elderly [27]. In 2010, the research of Luong revealed the intricate relationship between age and QoL, the higher the age, the lower QoL [25]. Our results are also in concert with several studies in other countries such as of Jan (2005) and Rana (2009) in rural Bangladesh [9, 18]. In 2010, the research of Luong revealed the intricate relationship between age and QoL, the higher the age, the lower QoL [25].
For elderly women, however, their QoL was significantly associated with educational level and socioeconomic status. Those who graduated secondary level and above and having average socioeconomic status or above were more likely to have desirable QoL than those who had lower level of education and socioeconomic status. Naing's findings in Myanmar also indicated that those who had more favorable socioeconomic status had better QoL than others [20]. As identified in Nigeria [4], educational level, socioeconomic status, genders and marital stability had a certain impact on QoL of the elderly. Among elderly men, the QoL is associated to several factors including Buddhism and Christianity, socioeconomic status and social connection. Those who followed Buddhism and Christianity, had better socioeconomic status and better social connection were likely to have better QoL. Generally in developing countries, males have a tendency to enjoy more privileges than their female counterparts now that they have better constitution and have more opportunities to participate in political, cultural, social activities than females. Our findings which are relevant to this perception also tally with the findings of previous studies. Research of Luong on the elderly in Hai Duong, Nilsson on the elderly in rural Bangladesh and Bowling 2002 all confirmed the relationship between social connections and QoL of the elderly [10, 25, 27, 28].
Also, according to our study, social engagement including socializing and visting pagodas is important to QoL. This is possible because most elderly hold the belief that visting pagodas an socializing would bring them more opportunities and luck in life. Many Vietnamese elderly today go to pagodas to seek peak and tranquillity of mind which may explain why they are more likely to develop a more positive attitude towards life than others. According to Luong, scores of QoL for those who visited pagodas on a regular basis were 4.9 times as high as those who did not [25]. Our findings also accord with the assessment of other studies in England and Bangladesh [10, 27]. Based on the analysis of factors associated with QoL, intervening programs for the elderly should be developed to encourage their active involvement in social activities like visiting pagodas, socializing or joining clubs, and other activities.
Limitations
As this is a cross-sectional study, it may have precluded the ordering of causality to a certain extent. It is therefore difficult to determine temporal relationships between the predictors and QoL. Another limitation would be related to the QoL measure (WHOQOL-BREF) which has not been widely applied in Vietnam. Yet, we piloted and validated this tool in our research with relatively good internal consistency and validity (both Cronbach's α and b's were relatively high). Besides, on the course of the survey, we had some questions asking for the subjects' past experience which may result in recall bias. However, this study was designed with a survey on a fairly large, representative sample with anonymous and confidential commitment, it would partly reduce that bias. As the majority of studies previously conducted in Vietnam and around the world focused mainly on QoL and its related factors among the elderly in general, our research aims to provide a fundamental understanding about QoL between genders along with its associated factors and make a solid foundation for further research on this topic.
Conclusions and implications
In this study, there were notable differences in QoL and predictors between elder women and men. Contributors to QoL including 80 years of age and older, and sickness in the past 6 months were significantly correlated with lower QoL in both sexes.
There were other factors related to the QoL of elderly men. Those who followed Buddhism and Christianity were more likely to have a favorable QoL than those who did not. The good social connections they had, the higher their scores of QoL were. As for elderly women, who completed secondary level or above, had medium and high socioeconomic status were more likely to have better QoL than others.
These findings suggest some strategies to improve QoL in the elderly. First, intervention programs need to take gender issues into account due to differences in QoL related factors between men and women. To be specific, local authority, civil and mass organizations should design interventions that help to develop to promote social connections in elderly men in order to improve their QoL. For elderly women, local governments are anticipated to invest more on the development of their educational levels which is greatly expected to give women an edge in promoting their well- being both mentally and physically, which in turn improve their QoL. This is especially integral in rural areas where any advance in academic background will possibly enhance people's awareness on their standing which is of great value to a desirable QoL. In both genders, the elderly who are 80 years of age and over, and experience sickness in the past 6 months need relevant support by healthcare and social organizations to gain more access to medical and social service in case of difficulties and ailments. Besides, State officials and organizations are highly anticipated to provide duly care for the lone elderly, elderly women and those who do not have income. The elderly need to be encouraged to exercise more and participate more in family and social activities. Local clubs for the elderly deserve public attention to be consistently developed with more diversified and enriching activities to encourage socializing, knowledge enhancement, and cultural exchange among members. As Vietnam has much in common with other developing countries in Southeast Asia, we immensely hope that this research could be of great help to public heath systems in similar countries. Moreover, a longitudinal study is needed to address this concern, especially needed are studies of gender, the role of family, marriage and social networks for the elderly QoL.
Recommendations
The education branch needs to have policies to ensure gender equitable young people in access to education and where possible educational facilities for middleaged people to catch up.
ACKNOWLEDGMENTS
We are indebted to the local authority and commune clinic centres whose useful supports profoundly facilitated our research implementation. We express our deep gratitude to the field teams for their enthusiasm and tirelessness in data collection. The largest debts are owed to the elderly whose enthusiastic participation helped us successfully complete this research.
The authors declare that they have no competing interests.
References
- 1. UNFPA , author. The aging population in Vietnam: Current status, prognosis, and possible policy responses. 2011.
- 2.Apidechkul T. Comparison of quality of life and mental health among elderly people in rural and suburban areas, ThaiLand. South Asian J Tropical Med Public Health. 2011;42:1282–1292. [PubMed] [Google Scholar]
- 3.Mudey A, Ambekar S, C.Goyal R, Agarekar S, Wagh VV. Assessment of quality of life among rural and urban elderly population of Wardha district, Maharashtra, India. EthnoMed. 2011;5:89–93. [Google Scholar]
- 4.Fajem Ilehin BR, Odebiyi AI. Redictors of elderly persons' quality of life and health pratices in Nigeria. Int J Sociolo Anthropol. 2011;3:245–252. [Google Scholar]
- 5.Campbell F, Bodley A, Berkley C. Measuring quality of life: Does local environmental quality matter? Environmental Campaigns Ltp. 2007 [Google Scholar]
- 6.Sarmiento OL, Schmid TL, Parra DC, Díaz-del-Castillo A, Gómez LF, MichaelPratt EJ, Jacoby E, Pinzón JD, Duperly J. Quality of life, physical activity, and built environment characteristics among Colombia adults. J Phys Act Health. 2010;7:181–195. doi: 10.1123/jpah.7.s2.s181. [DOI] [PubMed] [Google Scholar]
- 7.Djernes JK. Prevalence and predictors of depression in populations of elderly: a review. Acta Psych Scand. 2006;113:372–387. doi: 10.1111/j.1600-0447.2006.00770.x. [DOI] [PubMed] [Google Scholar]
- 8.Nilsson J, Rana AKMM, Huy LD, Winblad B, Kabir ZN. Health-related quality of life in old age: A comparison between Bangladesh and Vietnam. Asia Pacific J Public Health. 2005;24:610–619. doi: 10.1177/1010539510396699. [DOI] [PubMed] [Google Scholar]
- 9.Nilsson J, Grafstrom M, Zamand S, Kabir ZN. Role and function: Aspects of quality of life of older people in rual Bangladesh. J Aging Studies. 2005;19:63–74. [Google Scholar]
- 10.Nilsson J. Understanding health – related quality of life in old age – A cross-sectional study of elderly people in rural Bangladesh. 2005. [PhD Thesis]
- 11. Quality of living worwide city rankings - Mercer survey. Available from: http://www.mercer.com/qualityoflivingpr#city-rankings.
- 12.Huong NT. Applying the modified measurement for assessing quality of life of elderly and tested on a number of groups of Vietnamese elderly. Hanoi: 2009. [Google Scholar]
- 13.Xoan KT. Assessment of quality of life and several related factors among the elderly in Yen So, Hoai Duc, Hanoi in 2012. 2012. [Master of Public Health]
- 14.Hoi Le Van, Nguyen TK Chuc, Lindholm L. Health-related quality of life and its determinants, among older people in rural Vietnam. BMC Public Health. 2011;10:549–549. doi: 10.1186/1471-2458-10-549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ha NT, Duy HT, Le NH, Khanal V, Moorin R. Quality of life among people living with hypertension in a rural Vietnam community. BMC Public Health. 2014;14:833–833. doi: 10.1186/1471-2458-14-833. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kamp Iv, Leidelmeijera K, Marsman G, Hollander Ad. Urban environmental quality and human well-being towards a conceptual framwork and demarcation of concepts; a literature study. Landscape and Urban Planning. 2003;65:5–18. [Google Scholar]
- 17.Orley J. WHOQOL-BREF, Introduction, Administration, Scroring and Generic version of the assessment. Progr Mental Health WHO. 1996:5–18. [Google Scholar]
- 18.Masud Rana AKM, Wahlin A, Lundborg CS, Kabir ZN. Impact of health education on health-related quality of life among elderly persons: results from a community-based intervention study in rural Bangladesh. Health Prom Int. 2009;24:36–45. doi: 10.1093/heapro/dan042. [DOI] [PubMed] [Google Scholar]
- 19. National criteria for new rural areas. Available from: http://newcountryside.gov.vn/vn/htvb/vbpq/Lists/LawDocument/View_Detail.aspx?ItemID=1222&Page=1.
- 20.Naing MM, Nanthamongkolchal S, Munsawaengsub C. Quality of life of the elderly people in Einme township Irrawaddy Division, Myanmar. Asia J Public Health. 2010;1:4–10. [Google Scholar]
- 21. WHO Quality of Life-BREF (WHOQOL-BREF). Available from: http://www.who.int/substance_abuse/research_tools/whoQoLbref/en/.
- 22.Asnani MR, Lipps GE, Reid ME. Utility of WHOQOL-BREF in measuring quality of life in sickle cell disease. Health and Quality of Life Outcomes. 2009;7:75–75. doi: 10.1186/1477-7525-7-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Osborne RH, Hawthorneb G, Lewc EA, Gray LC. Quality of life assessment in the community-dwelling elderly: validation of the assessment of quality of Life (AQOL) instrument and comparison with the SF-36. J Clin Epidemiol. 2003;56:138–147. doi: 10.1016/s0895-4356(02)00601-7. [DOI] [PubMed] [Google Scholar]
- 24.Blay SL, Marchesoni MSM. Association among physical, psychiatric and socioeconomic conditions and WHOQOL-Bref scores. Cadernos De Saúde Pública Reports in Public Health. 2011;27:677–686. doi: 10.1590/s0102-311x2011000400007. [DOI] [PubMed] [Google Scholar]
- 25.Luong DH. Examining quality of life among the elderly and experimenting intervening programs in Chi Linh, Hai Duong. Military Medical University; 2010. [Master of Public health] [Google Scholar]
- 26. Equality UN-GoVNJPoG. Results from the national study on domestic violence against women in Viet Nam 2010.
- 27.Kharicha K, Iliffe S, Harari D, Swift C, Gillmann G, Stuck AE. Health risk appraisal in older people living alone an at risk group? Br J Gen Practice. 2007;57:271–276. [PMC free article] [PubMed] [Google Scholar]
- 28.Bowling A, Gabriel Z. Lay theories of quality of life in order age. Ageing Society. 2007;27:827–848. [Google Scholar]