

Abstract
Osteoarthritis is characterized by the degeneration of articular cartilage. Cartilage metabolic markers have been explored as possible markers for osteoarthritis, and osteogenic protein -1 (OP-1) has emerged out to play a major role in cartilage repair. Oxidative stress has been implicated as a mediator of cartilage damage in patients with osteoarthritis. The aim of this study was to correlate the cartilage metabolic markers and antioxidants with the severity of knee osteoarthritis.
Keywords: Antioxidants, cartilage metabolic markers, osteoarthritis, osteogenic protein-1
Osteoarthritis (OA) is characterized by the destruction of articular cartilage, sub-chondral bone thickening and formation of osteophyte. Knee OA represents one of the most prevalent forms of OA1. Based on racial and ethnic groups, research findings have supported the role of ethnicity in the progression of OA2. Andersen et al3 have reported that occupation involving heavy physical workload is a determinant for hip and knee OA. Biomarkers such as osteogenic protein-1 (OP-1), keratan sulphate (KS) and hyaluronic acids (HAs) present in the synovial fluid (SF) have been studied as cartilage metabolic markers4 and these may also be markers of biosynthetic or degradative changes5. OP-1, a member of the bone morphogenetic protein family, is reported to have beneficial anabolic and anti-catabolic effect on cartilage5. Reactive oxygen species (ROS) are deleterious agents having an important role in pathogenesis of OA by causing oxidative damage produced within the cell6. Different biochemical markers have been studied for monitoring the cartilage destruction and repair7. The severity of OA is graded radiographically and using other techniques for determining the pathology, but the severity may not correlate with the patient's therapeutic needs.
We have earlier studied the correlation of synovial fluid OP-1 with age, antioxidants levels in the blood and also cartilage metabolic markers such as HA and KS in the synovial fluid of OA patients8. The present study was an extension of the earlier study with the aim to look for relationship between the cartilage metabolic markers and the severity of OA along with the demographic characteristics (age, gender, ethnicity, occupation and family size) in the same patients8. The correlation between cartilage metabolic markers, antioxidants and the severity of OA was analysed by Spearman's rank coefficient.
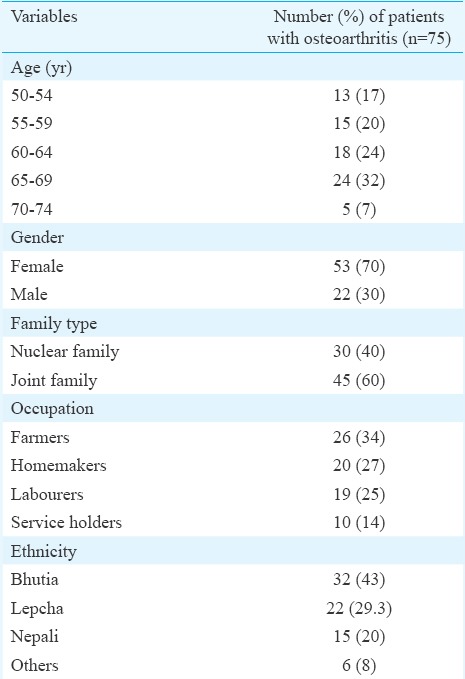
The demographic characteristics of patients suffering from knee OA are shown in Table I. Of the 75 patients suffering from knee OA, 24 (32%) were in the age group of 65-69 yr followed by 18 (24%) patients between 60 and 64 years of age. More females (n=53, 70%) were found to be suffering from knee OA than males (n=22, 30%). By occupation, 34 per cent (n=26) were farmers suffering from knee OA, 27 per cent (n=20) were homemakers and 25 per cent (n=19) were labourers (Table I). Ethnic groups were classified into Bhutia, Lepcha and Nepali9. It was observed that the most predominant ethnic group with knee OA was the Bhutias (43%, n=32) followed by 29.3 per cent Lepchas (n=22). Fifteen (20%) were Nepalis and only six (8%) belonged to other communities.
Table I.
Frequency distribution of patients suffering from knee osteoarthritis according to demographic characters
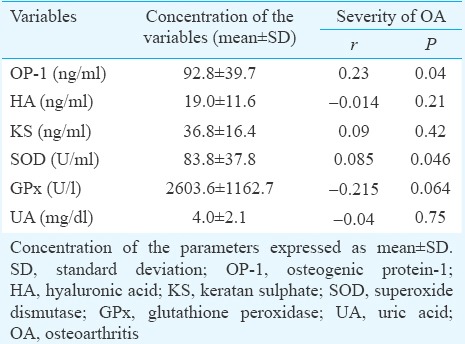
The correlation between the cartilage metabolic markers (HA, KS, OP-1) in the SF and the antioxidants (SOD, GPx, UA) in the blood of the osteoarthritic patients is shown in Table II. OP-1 showed a positive significant correlation (r=0.23, P<0.05) with the severity of OA whereas antioxidants and cartilage metabolic markers did not show significant correlation with the severity of OA.
Table II.
Correlation of cartilage metabolic markers and antioxidants with severity of knee osteoarthritis
The highest number of patients suffering from knee OA was found to be in the 65-69 yr age group. The strong association between age and increasing incidence of OA marks OA as an age-related disease10. Several studies have observed that the incidence of knee OA increases by age and increases further with longer life span11,12. High frequency of knee OA (46.7%) has been reported among people of 60 years of age and above13. The changes in the articular cartilage are age dependent with increased risk of the synovial joint degeneration leading to the clinical syndrome of OA.
It was observed that more women were suffering from knee OA than men. Population-based studies in developed and developing countries have reported a higher prevalence of radiographic knee OA in women than in men14. At the time of menopause, loss of oestrogen increases the women's risk of getting OA15 influencing the joint tissues activities by acting at various levels through complex molecular pathways16.
The Bhutias were found to be more commonly affected by knee OA than other communities of Sikkim. Dietary and genetic factor may be one of the causes of progression and development of OA. There is evidence from a longitudinal study that low dietary and serum levels of vitamin D may be associated with the development and progression of knee OA17. It has been reported that there are ethnic differences in arthritis-related disease, such as disability and pain18. Further studies on genetic and dietary factors will be required to substantiate the cause of increased incidence of knee OA in certain ethnic groups of Sikkim.
The significant positive correlation between OP-1 and the severity of OA may suggest the anabolic role of OP-1 in cartilage repair and regeneration in knee OA. Similar results were also observed by Honsawek et al19. This could be due to increased expression and production of OP-1 residing in extracellular matrix in an autocrine or a paracrine manner20.
In conclusion, the present results showed that OP-1 might serve as a biochemical parameter for determining disease severity in primary knee OA. Further studies with larger sample size need to be carried out to confirm OP-1 as a marker of disease status. Studies are required to be done to examine the genetic and lifestyle factors that may contribute to the development of knee OA.
Acknowledgment
Authors acknowledge the North Eastern Region of NER-BMPC, Department of Biotechnology (DBT), India, for the grant under the Institutional level Biotechnology Hub Project.
Footnotes
Conflicts of Interest: None.
References
- 1.Arden N, Nevitt MC. Osteoarthritis: epidemiology. Best Pract Res Clin Rheumatol. 2006;20:3–25. doi: 10.1016/j.berh.2005.09.007. [DOI] [PubMed] [Google Scholar]
- 2.Zhang Y, Jordan JM. Epidemiology of osteoarthritis. Clin Geriatr Med. 2010;26:355–69. doi: 10.1016/j.cger.2010.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Andersen S, Thygesen LC, Davidsen M, Helweg-Larsen K. Cumulative years in occupation and the risk of hip or knee osteoarthritis in men and women: a register-based follow-up study. Occup Environ Med. 2012;69:325–30. doi: 10.1136/oemed-2011-100033. [DOI] [PubMed] [Google Scholar]
- 4.Chubinskaya S, Frank BS, Michalska M, Kumar B, Merrihew CA, Thonar EJ, et al. Osteogenic protein 1 in synovial fluid from patients with rheumatoid arthritis or osteoarthritis: relationship with disease and levels of hyaluronan and antigenic keratan sulfate. Arthritis Res Ther. 2006;8:R73. doi: 10.1186/ar1947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Thonar EJMA, Manicourt DH. Noninvasive markers in Osteoarthritis. In: Markowitz R, Goldberg V, Vowell DS, Altman RD, Buckwalter J, editors. Osteoarthritis: diagnosis and medical/surgical management. 3rd ed. Philadelphia, PA: WB Saunders; 2001. pp. 293–313. [Google Scholar]
- 6.Henrotin Y, Deby-Dupont G, Deby C, Franchimont P, Emerit I. Active oxygen species, articular inflammation and cartilage damage. EXS. 1992;62:308–22. doi: 10.1007/978-3-0348-7460-1_31. [DOI] [PubMed] [Google Scholar]
- 7.Rueger DC, Chubinskaya S. BMPs in articular cartilage repair. In: Vukicevic S, Sampath KT, editors. Bone morphogenetic proteins: regeneration of bone and beyond. Basel: Birkhauser Verlag AG; 2004. pp. 109–32. [Google Scholar]
- 8.Bhutia SC, Singh TA, Sherpa ML. Correlation of Osteogenic Protein-1 (OP-1) with age, cartilage metabolic markers and antioxidants in the osteoarthritic patients of Sikkim. J Clin Diagn Res. 2013;7:1565–7. doi: 10.7860/JCDR/2013/5296.3209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bhasin V. Ethnic relations among the people of Sikkim. J Soc Sci. 2002;6:1–20. [Google Scholar]
- 10.Martin JA, Buckwalter JA. Aging, articular cartilage chondrocyte senescence and osteoarthritis. Biogerontology. 2002;3:257–64. doi: 10.1023/a:1020185404126. [DOI] [PubMed] [Google Scholar]
- 11.Losina E, Weinstein AM, Reichmann WM, Burbine SA, Solomon DH, Daigle M, et al. Lifetime risk and age of diagnosis of symptomatic knee osteoarthritis in the US. Arthritis Care Res. 2013;65:10. doi: 10.1002/acr.21898. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Saraswathi K, Prakasamma M. Analysis of the problems of the aged above 60 years in a selected urban community in Hyderabad. Nurs J India. 2000;91:86–8. [PubMed] [Google Scholar]
- 13.Bliddal H, Christensen R. The treatment and prevention of knee osteoarthritis: a tool for clinical decision-making. Expert Opin Pharmacother. 2009;10:1793–804. doi: 10.1517/14656560903018911. [DOI] [PubMed] [Google Scholar]
- 14.World Health Organization. The burden of musculoskeletal conditions at the start of the new millennium, Report of a WHO Scientific Group. WHO Technical Report Series No. 919. Geneva: WHO; 2003. [PubMed] [Google Scholar]
- 15.Spector TD, Campion GD. Generalised osteoarthritis: a hormonally mediated disease. Ann Rheum Dis. 1989;48:523–7. doi: 10.1136/ard.48.6.523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Roman-Blas JA, Castañeda S, Largo R, Herrero-Beaumont G. Osteoarthritis associated with estrogen deficiency. Arthritis Res Ther. 2009;11:241. doi: 10.1186/ar2791. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.McAlindon TE, Jacques P, Zhang Y, Hannan MT, Aliabadi P, Weissman B, et al. Do antioxidant micronutrients protect against the development and progression of knee osteoarthritis? Arthritis Rheum. 1996;39:648–56. doi: 10.1002/art.1780390417. [DOI] [PubMed] [Google Scholar]
- 18.Dominick KL, Baker TA. Racial and ethnic differences in osteoarthritis: prevalence, outcomes, and medical care. Ethn Dis. 2004;14:558–66. [PubMed] [Google Scholar]
- 19.Honsawek S, Chayanupatkul M, Tanavalee A, Sakdinakiattikoon M, Deepaisarnsakul B, Yuktanandana P, et al. Relationship of plasma and synovial fluid BMP-7 with disease severity in knee osteoarthritis patients: a pilot study. Int Orthop. 2009;33:1171–5. doi: 10.1007/s00264-009-0751-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Rueger DC, Chubinskaya S. BMPs in articular cartilage repair. In: Vukicevic S, Sampath KT, editors. Bone morphogenetic proteins: regeneration of bone and beyond. Basel: Birkhauser; 2004. pp. 109–32. [Google Scholar]