

Sir,
Dengue fever, a mosquito-borne viral disease, is a major public health problem globally1. It has been estimated that more than 390 million dengue infections occur every year, of which 96 million manifest clinically2,3. India contributes to about a third of global burden of apparent dengue infections2,3. As per India's Integrated Disease Surveillance Programme, more than 100 dengue outbreaks were reported in 20154. Good laboratory-based disease surveillance is essential for early detection of dengue outbreaks and implementation of effective preventive and control measures1.
Department of Health Research (DHR) and Indian Council of Medical Research (ICMR), Government of India, have established Virus Research and Diagnostic Laboratory Network (VRDLN) to strengthen the laboratory capacity in the country for providing timely diagnosis of disease outbreaks5. The fully functional network would consist of 120 laboratories at the medical college level, 30 State level and 10 regional level laboratories5. VRDLs receive samples from the district public health authorities for laboratory confirmation of disease clusters (suspected outbreaks). Besides, providing diagnosis to disease outbreaks, VRDLs also provide virological diagnosis to patients seeking healthcare at the medical colleges where VRDLs are located. In January 2016, 34 VRDLs (24 medical college level, 5 State level and 5 regional level) were operational established in 23 Indian States. VRDLs, which follow a uniform protocol for laboratory testing, have a facility to test up to 27 viral aetiologies (hepatitis: hepatitis A, B, C and E; arboviruses: Japanese encephalitis, West Nile, dengue, chikungunya, Chandipura virus and Kyasanur Forest Disease; respiratory viruses: influenza, parainfluenza, RSV, adenovirus, rhinovirus; fever with rash: measles, rubella, varicella zoster, mumps and parvovirus B 19; herpesvirus family: EB virus, herpes simplex virus and cytomegalovirus; enteric viruses: rotavirus, enteric adenoviruses, norovirus and astrovirus).
In this study, the laboratory surveillance data collected by VRDLN from January 2014 to December 2015 were analysed at the ICMR-National Institute of Epidemiology, Chennai, India, to describe the epidemiology of dengue fever in India. Between January 2014 and December 2015, VRDLs received samples from 205 suspected outbreaks (70 in 2014 and 135 in 2015) for laboratory diagnosis; 42 of which were due to dengue (13 in 2014 and 29 in 2015). A total of 4952 patients from these 42 clusters were investigated for IgM antibodies or NS1 antigen against dengue virus and 2442 (49.3%) were found positive (Table). The dengue clusters were reported from 39 districts of 12 Indian States (Figure). Most of the clusters reported in 2015 were from States of Rajasthan (n=6), Tamil Nadu (n=4), Odisha (n=4), Jharkhand (n=4), Punjab (n=3) and Assam (n=3). Twenty nine of the 42 clusters occurred during 33-48 wk of the calendar year corresponding to August-November months.
Table.
Details of dengue fever cases investigated by VRDLs during 2014-2015, with age and sex distribution of dengue positive patients
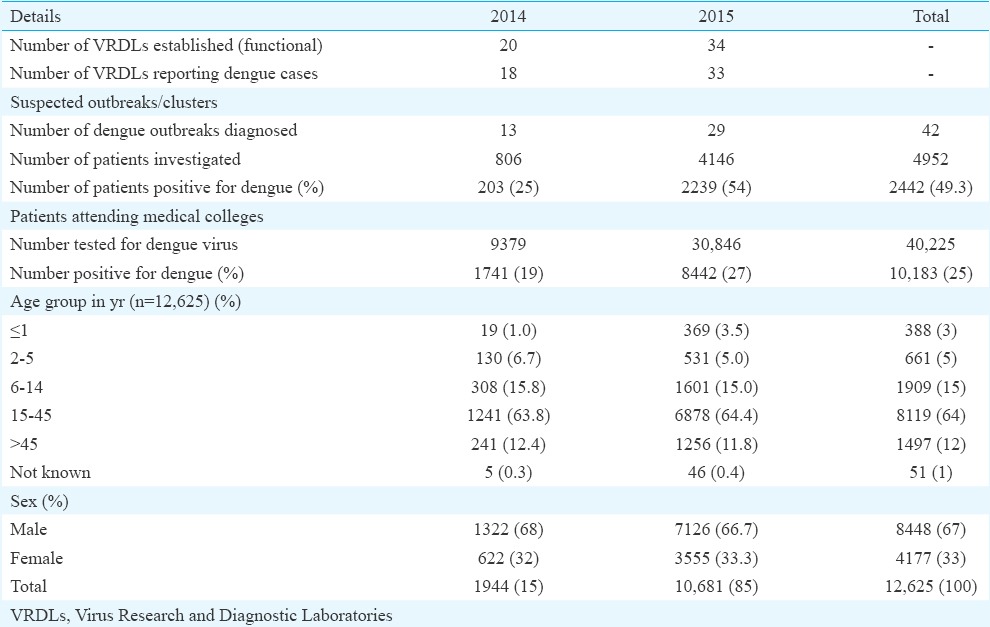
Figure.

Distribution of dengue fever outbreaks diagnosed by VRDLs in 2014-2015. [Maps generated through ESRI ArcGIS Desktop: Release 9.2. software (Redlands, CA, USA)].
In addition, during 2014 and 2015, VRDLs investigated 40,225 febrile patients attending the medical colleges that housed the VRDLs for dengue, of whom, 10,183 patients (25.3%) were sero-positive. Suspected and confirmed dengue cases increased from the month of June and peaked in the month of October (data not shown).
During this two year period, a total of 12,625 (2442 from suspected outbreaks and 10,183 amongst patients attending medical colleges) laboratory-confirmed dengue cases were diagnosed by the VRDLN. Nearly two-third of these cases were in the age group of 15-45 yr, whereas 23.6 per cent of the cases were reported amongst children aged ≤14 yr (Table). About two-third of the positive cases were males (67 vs. 33%, P<0.001, Chi square test) and male preponderance was observed in all the age groups (<1 yr: males=237, females=151, P<0.001; 2-5 yr: males=404, females=257, P<0.001; 6-14 yr: males=1187, females=722, P<0.001; 15-45 yr: males=5707, females=2412, P<0.001; >45 yr: males=876, females=621, P<0.001). This pattern of male predominance was consistent with the reports from several other countries and could be on the account of (i) greater exposure of males to dengue-carrying mosquitoes, or (ii) differences in the health-seeking behaviour of males and females5,6,7.
Our analysis had certain limitations. The analysis was based on the data collected from patients seeking care at the medical college hospitals covered under VRDLN and might not be generalizable to the entire country. Although the network collected information about the basic epidemiological characteristics (time: date of onset of illness and date of seeking care; place: village, subdistrict/tehsil and district; person: age, sex and clinical presentation), information about haematological investigations and outcome was not available. In spite of these limitations, the data generated by this network were useful to describe the epidemiology of dengue, which was one of the most common viral diseases prevalent in different parts of India. The data from the network indicated that dengue fever was the most common viral aetiology investigated by the VRDLs during 2014 and 2015.
In India, the laboratory capacity for diagnosis of outbreaks under Integrated Disease Surveillance Programme is limited8. The VRDLN aimed to provide timely diagnosis of disease outbreaks in the country, can be considered as a complementary effort. It is important to note that VRDLN investigated 205 disease clusters during 2014-2015, of which 42 were due to dengue fever. This network also generated case-based data on dengue fever to understand its epidemiology. Dengue serotype surveillance is important, as large dengue outbreaks tend to follow changes or re-introductions of serotypes9. In India, systematic dengue serotype surveillance is not conducted. The VRDLN may provide a unique opportunity for systematically generating dengue serotype information in future.
Acknowledgment
Authors acknowledge the Principal Investigators and staff of the following Virus Research and Diagnostic Laboratories: Manipal Centre for Virus Research, Manipal University, Manipal, Karnataka; ICMR-Regional Medical Research Centre, Port Blair, Andaman and Nicobar; King George's Medical University, Lucknow, Uttar Pradesh; ICMR-Regional Medical Research Centre, Bhubaneswar, Odisha; Late Sri Baliram Kashyap Memorial Government Medical College, Jagdalpur, Chattisgarh; SMS Medical College, Jaipur, Rajasthan; Rajiv Gandhi Centre for Biotechnology, Thiruvananthapuram, Kerala; ICMR-National Institute of Virology (field unit), Alappuzha, Kerala; King Institute of Preventive Medicine and Research, Chennai, Tamil Nadu; Rajendra Institute of Medical Sciences, Ranchi, Jharkhand; Andhra Medical College, Vishakhapatnam, Andhra Pradesh; ICMR-National Institute of Research in Tribal Health, Jabalpur, Madhya Pradesh; ICMR-Rajendra Memorial Research Institute of Medical Sciences, Patna, Bihar; ICMR-Regional Medical Research Centre for NE Region, Dibrugarh, Assam; Government Medical College, Agartala, Tripura; Osmania Medical College, Hyderabad, Telangana; Indira Gandhi Medical College, Shimla, Himachal Pradesh; Government Medical College, Jammu, Jammu and Kashmir; Sher-I-Kashmir Institute of Medical Sciences, Srinagar, Jammu and Kashmir; BJ Medical College, Ahmadabad, Gujarat; Patna Medical College, Patna, Bihar; Government Medical College, Amristar, Punjab; Pt. B.D. Sharma Post Graduate Institute of Medical Sciences, Rohtak, Haryana; Postgraduate Institute of Medical Education and Research, Chandigarh; North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong, Meghalaya; M.P. Shah Government Medical College, Jamnagar, Gujarat; Indira Gandhi Government Medical College, Nagpur, Maharashtra; Madurai Medical College, Madurai, Tamil Nadu; Sri Venketswara Institute of Medical Science, Tirupati, Andhra Pradesh; Government Theni Medical College, Theni, Tamil Nadu; Gauhati Medical College, Guwahati, Assam; Government Medical College, Thiruvananthapuram, Kerala; All India Institute of Medical Sciences, Bhopal, Madhya Pradesh; Siddhartha Medical College, Vijayawada, Andhra Pradesh. Authors also thank the Principal Investigator, scientists and staff from Resource Centre, VDL, NIV, Pune.
Footnotes
Conflicts of Interest: None.
References
- 1.World Health Organization. Dengue: guidelines for diagnosis, treatment, prevention and control. Geneva: World Health Organization; 2009. [accessed on February 16, 2016]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK143159/ [PubMed] [Google Scholar]
- 2.Fredericks AC, Fernandez-Sesma A. The burden of dengue and chikungunya worldwide: Implications for the Southern United States and California. Ann Glob Health. 2014;80:466–75. doi: 10.1016/j.aogh.2015.02.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, et al. The global distribution and burden of dengue. Nature. 2013;496:504–7. doi: 10.1038/nature12060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Integrated Disease Surveillance Programme (IDSP) [accessed on February 16, 2016]. Available from: http://www.idsp.nic.in/
- 5.Department of Health Research Ministry of Health and Family Welfare, Government of India, New Delhi. Annual Report 2014-2015. [accessed on February 16, 2016]. Available from: http://www.dhr.gov.in/sites/default/files/DHR%20Annual%20Report%20English_2014-15.pdf .
- 6.Anker M, Arima Y. Male-female differences in the number of reported incident dengue fever cases in six Asian countries. Western Pac Surveill Response J. 2011;2:17–23. doi: 10.5365/WPSAR.2011.2.1.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Arima Y, Chiew M, Matsui T. Emerging Disease Surveillance and Response Team, Division of Health Security and Emergencies, World Health Organization Regional Office for the Western Pacific. Epidemiological update on the dengue situation in the Western Pacific Region, 2012. Western Pac Surveill Response J. 2015;6:82–9. doi: 10.5365/WPSAR.2014.5.4.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Raut DK, Bhola A. Integrated disease surveillance in India: Way forward. [accessed on February 16, 2016];Glob J Med Public Health. 2014 3(4) Available from: http://www.gjmedph.org/uploads/R2-Vo3No4.pdf . [Google Scholar]
- 9.Beatty ME, Stone A, Fitzsimons DW, Hanna JN, Lam SK, Vong S, et al. Best practices in dengue surveillance: A report from the Asia-Pacific and Americas Dengue Prevention Boards. PLoS Negl Trop Dis. 2010;4:e890. doi: 10.1371/journal.pntd.0000890. [DOI] [PMC free article] [PubMed] [Google Scholar]