

Abstract
Background:
Multiple sclerosis (MS) could be considered as one of the most common chronic disorders of the central nervous system. However, patient education tasks in this group are a challenge for health care provider team but due to increase in the incidence of MS, a new category of contact, care, and education seems to be useful. Hence, the aim of this study was to compare the effect of electronic education and illustrated booklet on knowledge of patients with MS.
Methods:
This was a quasi-experimental research was carried out on 120 patients with MS from January 2013 to July 2013. All patients attended MS clinic located at the Ayatollah Kashani Hospital conducted to Isfahan Neurosciences Research Center (INRC). Patients were divided randomly into two equal groups: (1) Electronic education (n = 60) and (2) illustrated booklet (n = 60). Participants’ knowledge score was collected according to the researcher-made questionnaire with 40 questions. Data were analyzed using Student's t-test and paired t-test through SPSS (version 11.5) with a significance level of P < 0.05.
Results:
Although there was not any significant difference between the knowledge score of electronic education and illustrated booklet group before intervention (18 ± 2.2 vs. 17.01 ± 3.4(, (P = 0.434, t = −5.64), but there was a significant difference after 2 weeks intervention (35.74 ± 1.4 vs. 33.74 ± 3.4), (P = 0.021, t = −6.64). Paired t-test showed a statistically significant difference in the knowledge level in both groups after intervention as follow: (1) Electronic education (18 ± 2.2 vs. 35.74 ± 1.4), (P = 0.024, t = −7.55) and illustrated booklet (17.01 ± 3.4 vs. 33.74 ± 3.4), (P = 0.003, t = −8.55).
Conclusion:
The electronic educational program applied in this study appears increased knowledge of patients with MS. Therefore, the conveyance of this program to earn time for patient and healthcare provider team is suggested as a valuable and appropriate teaching method.
Keywords: Electronic education, Iran, knowledge, multiple sclerosis
INTRODUCTION
Due to the increasing incidence of multiple sclerosis (MS) all over of the world and in Isfahan/Iran,[1,2,3,4,5] attention, care and education to these patients in order to alleviate the disease symptoms seem to be essential. In fact, the patient education could be accounted as a major component of any health care facility. Training component determines the level of patient satisfaction and quality of the patient-physician relationship. While health professionals, especially nurses, and doctors have no enough time, therefore educational program, could be involved as (1) Giving brochures (2) teaching traditional education and (3) referrals to other health centers or even (4) not giving any education. It is well known that all of the four mentioned items could influence clinical outcome. Electronic applications could be considered as an alternative method for improving the quality of education offered to the patient. With the increasing popularity of computer-based training methods for both the physician and the patient, these activities could be considered as a way to promote activities related to the education of the patient.[6,7,8,9,10,11,12] Research has shown that virtual method in terms of time, place and even economic conditions have better facilities for the learner.[13,14,15] This kind of learning seems to be learner-centered, and can be tailored to learner needs and information requirements of time and place, pace, and content set.[16,17,18]
Within this electronic program, in addition to text, there are things such as images, animations and sound, which can cause learning more. The virtual training data could be done at home, during traveling, or at any time when necessary to provide them with data and also could be print it out easily by the patient whenever it is needed.[18,19,20] Although e-learning has spread around the world through computer education to patients, but patient education via computer is still rare. A study performed by Neafsey et al. in 2002, and Southard et al. in 2003, confirmed that e-learning could influence patients’ awareness.[21,22] Whereas in a study performed by Street et al. in 1995, and Murray et al. in 2001, such an effect was not recognized.[23,24] However, unfortunately, the medical staff in their training, communication, and education, due to many responsibilities, less emphases on education. It is possible that the content of the lecture related to patients (e.g., with MS) may be forgotten. Using programs based on video or computer depends could be useful in case of not understanding or forgetting things. It seems that it is necessary to health professionals that should have the necessary knowledge related to e-learning.[11,12,13,14,15,16,17,18,19,20,21,22,23,24] Therefore, given the importance of effective teaching methods and appropriate care for patients with MS, several methods of teaching are currently used. Most of these methods particularly in the areas of health are lectures and pamphlets.[11] In order to provide effective methods of teaching for patients with MS, due to contradictory published work, the aim of this study was to investigate and compares two teaching method (e-learning and illustrated booklet) on the knowledge and consent of training in patients who attended MS clinic located at the Isfahan Ayatollah Kashani Hospital.
METHODS
A two groups pool blind quasi-experimental investigation was carried out on 120 patients with MS. According to the formula, 50 patients were calculated for each group.

(n = sample volume, Z = confidence level, P = expected prevalence, d = accuracy).
Due to approximately 20% loss of samples (10 patients), the final sample size of 60 patients, was calculated per each group. Therefore, at the end of this study, 120 patients in each group completed the study packages. The sampling procedure was in order to the easy way and performed on those who referred to the MS clinic located at the Isfahan Ayatollah Kashani Hospital. On the day of experiment based on the lottery, the first runner-up was assigned as e-learning and the second one as illustrated booklet. Inclusion criteria were as follows: (1) Age between 15 and 50 years (2) consent to participate in this study (3) having a phone number to call (4) have at least literate reading and writing (5) having the ability to speak, to hear and to see and finally (6) there is a computer or video device at home and the ability to use these devices (in both educational groups). Exclusion criteria were as follows: (1) Employees working in the medical field (2) those who attended educational classes related to MS.
At first informed consent form was given to patients, and the purpose of the study was explained to them. Then in the group of multimedia, after visiting the MS patients by a neurologist, a CD was given to them. The CD contained MS education through text, pictures, animation, and sound, as well as a slideshow. This 30-min software contained MS education on the following issues: (i) Description of the disease (ii) causes, sign and symptom, effects of disease on health, prognosis, treatment, benefits and side effects of treatment, recommendation on how to alleviate the symptoms of diseases. Access to the internet was not possible for all patients in the form of an open line in the present study, and it was found that in similar studies, the materials were taught through multimedia method. On the other hand, the internet speed is so low that it leads to low quality of sound and image in online education in Iran. Therefore, educational content was in the format of a web page or Flash Video, Windows Media Video, and MPEG-4 (MP4), as these formats can be used in a closed line web. After the explanation was given to the patients as to how to use the CD, they were informed that they would be asked some related questions 2 weeks later. In the second group, after being visited, in the second group were given an illustrated booklet that contained text with pictures (illustration). The subjects were asked to study the material, and after 2 weeks, an awareness questionnaire was again filled for them.[l] Education content in both education groups, designed by the researcher, was similar.
For both groups, demographic information such as name, surname, age and disease data were filled. Another questioner form including the awareness of illness in patients with MS was placed and authorized to research units. Questionnaire related to MS patients’ awareness’ training included eight sides education such as: (1) Explain how patient's illness was started (5 items) (2) causes (5 items) (3) signs and symptoms (5 items) (4) complications (5 items) (5) prognosis (5 items) (6) treatments (5 items) (7) benefits and side effects-related to treatments (5 items) (8) recommendations on reducing symptoms and complications (5 items). The questionnaire was included 40 questions that patients could choose one of these options: Right, wrong or I do not know with a score range of 0–40. Due to lack of availability of a standard questionnaire in this field, so this questionnaire was designed through use of countrywide national project, references, and textbooks, and its validity was confirmed by five faculty members of the of Isfahan University of Medical Sciences. Its reliability was confirmed by use of a pilot study (questionnaire was given to 10 patients with MS) and calculation of Cronbach's alpha (α = 0.89). Data were analyzed by Student's t-test and paired t-test through version 11.5 [SPSS Inc., Chicago, IL, USA] with a significance level of P < 0.05.
RESULTS
The mean age, duration of the disease and visit of patients to MS clinic were (20/3 ± 4/01) years and (2/5 ± 2/02) years and (2.3 ± 1.11) month respectively. Most sources of information related to learning about the disease were as follow: Television 39 (33%), book 15 (12%). To get information some patients were offered family and friends and in others were as follow: Television 39 (33%), radio 26 (22%), and internet 19 (16%).
Two groups before intervention were homogenous, and there were no significant differences related to age, duration of disease, the mean visit of MS clinic (P > 0.05). Table 1 shows that the mean knowledge score related to training diseases within two groups that is, electronic and illustrated the booklet, after the intervention in compared to before the intervention has increased significantly.
Table 1.
Comparison of patients’ awareness and education related to disease training before intervention and 2 weeks after intervention within two groups that is, electronic and illustrated booklet

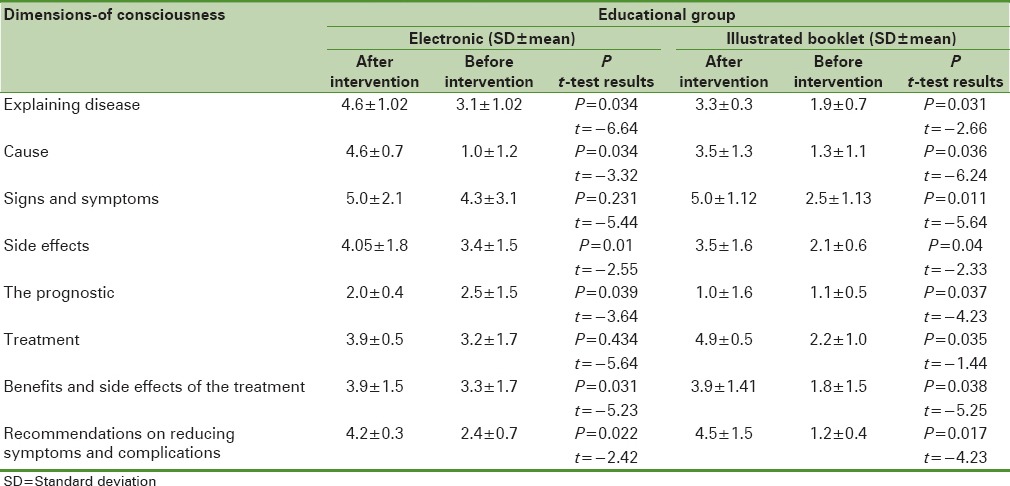
The findings show that the highest (5.0 ± 2.1, 5.0 ± 1.12) and lowest (2.0 ± 0.4, 1.0 ± 1.6) scores on various aspects of knowledge after the intervention in both groups that is, the electronics and the illustrated leaflets, were the signs, symptoms and prognosis of the disease respectively [Table 2].
Table 2.
Comparison of patients’ awareness and education related to disease training before the intervention and 2 weeks after the intervention within two groups that is, electronic and illustrated booklet
DISCUSSION
The result showed that there is a significant increase after the intervention in the mean knowledge score, than before the intervention within two groups of electronic learning and illustrated booklet. In other words, this increase could represent the effectiveness of both educational methods in the awareness of patients with MS. In confirming the effectiveness of education on knowledge and satisfaction of the subjects, it would be pointed out to the studies of Mohamadirizi and Shaygannejad, Mohamadirizi et al.[25,26] In this regard the study of Southard et al., in 2003, on the 104 heart patients showed that 6 months after the intervention within electronic training group, the rate of cardiovascular events were lower than the illustrated booklet group (normal training) respectively.[22] The results of another study performed by Neafsey et al., in 2002, in elderly (age: 85 years) showed that the use of computer-based training (2 weeks after intervention) increased awareness about drug interactions and improved self-efficacy in consumer of drugs.[21]
Our findings showed that e-learning have been associated with increased awareness of patients with MS. Among the features of this study, data collection consisted of eight different training topics that were included as: (1) Explaining disease (2) causes (3) signs and symptoms (4) side effects (5) prognosis (6) different treatments (7) benefits and side effects of the treatment (8) recommendations on reducing signs and symptoms.
Sensory difficulties’ such as vision problems (blurred vision or double vision) are common in patients with MS[27] which could stand as a barrier in front of teaching and learning. Based on e-learning's method, it is quite possible for the patient to use other senses such as hearing.[11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26] With auscultation to the mentioned topics, patients could meet their educational needs. In addition to the items listed, using training computer-based, study performed by Gustafson et al., found no significant differences in terms of improving knowledge of breast cancer between the two groups that is, computer-based training and brochures.[28,29]
Our results within the population studied here, demonstrate the effectiveness of both methods that could be illustrated as pamphlets, and e-learning. Table 1 shows that the significant differences were seen in the percentage change related to awareness’ score in both groups of e-learning and illustrated the booklet. However, the change percentage in awareness’ score in the intervention group (e-learning), have been far greater when compared to illustrated booklets (illustrated instruction booklet). Therefore, it could be assumed that e-learning is more effective in improving patient awareness’. A study performed by Langkamp et al., confirmed that the combination of verbal and written instructions seem to be more useful than theological education alone.[30] In fact, based on e-learning (Multimedia), information in written form with speech and animation could be accessible at home, while traveling or at any time. The content of information could be printed it out easily, at any time that seem to be necessary. Also for many patients who have not the habit of reading, e-learning could be an important source of health information.[31,32]
The results of this study should be considered along with its limitations and strengths. The limitations of the study were the possibility of obtaining Information from other sources on research it could occur in all two groups and out-of-control researchers. Another limitation of this study was that data were collected through self-report. Also due the high cost of travel and time of visit to the door houses to complete the posttest, we tried that in any the two groups were done by phone. The Strength of this study was to compare both methods electronics and illustrated booklet while other studies were done, the only one of the two types of education.[33]
However, it is clear that in all studies, measuring the amount of learning is the score that is normally obtaining by test, but learning due to responsibility for self-learning in e-learning group seem to be deeper than other educational methods.
Finally, it could be imagined that within e-learning method, training focuses on knowledge construction and not necessarily on knowledge accumulation.
CONCLUSION
The results obtained in this study indicated that both electronic education and illustrated booklet methods had a great impact on promoting the knowledge level of MS patients. Also it conveys that the e-learning method could be more effective than the pamphlets in order to increasing awareness of the disease. Therefore, due to spending lower cost and less time e-learning besides the usual training, could be used by patients and the health care team provider.
Financial support and sponsorship
Isfahan University of Medical Science.
Conflicts of interest
There are no conflicts of interest.
Acknowledgments
We would like to gratefully acknowledge MS Clinic located at the Isfahan Kashani Hospital conducted to the INRC for the valuable moral co-operation in respect to providing patients and collaboration of all staff. Special thanks to Professor Fereshteh Ashtari, Head of Isfahan Kashani Neurology ward for her kind, patience and scientific support.
REFERENCES
- 1.Evans C, Beland SG, Kulaga S, Wolfson C, Kingwell E, Marriott J, et al. Incidence and prevalence of multiple sclerosis in the Americas: A systematic review. Neuroepidemiology. 2013;40:195–210. doi: 10.1159/000342779. [DOI] [PubMed] [Google Scholar]
- 2.Tullman MJ. Overview of the epidemiology, diagnosis, and disease progression associated with multiple sclerosis. Am J Manag Care. 2013;19(2 Suppl):S15–20. [PubMed] [Google Scholar]
- 3.Etemadifar M, Maghzi AH. Sharp increase in the incidence and prevalence of multiple sclerosis in Isfahan, Iran. Mult Scler. 2011;17:1022–7. doi: 10.1177/1352458511401460. [DOI] [PubMed] [Google Scholar]
- 4.Etemadifar M, Janghorbani M, Shaygannejad V, Ashtari F. Prevalence of multiple sclerosis in Isfahan, Iran. Neuroepidemiology. 2006;27:39–44. doi: 10.1159/000094235. [DOI] [PubMed] [Google Scholar]
- 5.Tolou-Ghamari Z, Shaygannejad V, Ashtari F. Preliminary study related the incidence of methylprednisolone pulse therapy in patients visited multiple sclerosis clinic located at the Isfahan Kashani Hospital. Int J Prev Med. 2013;4(Suppl 2):S274–8. [PMC free article] [PubMed] [Google Scholar]
- 6.Shaygannejad V, Dehnavi SR, Ashtari F, Karimi S, Dehghani L, Meamar R, et al. Study of type a and B behavior patterns in patients with multiple sclerosis in an Iranian population. Int J Prev Med. 2013;4(Suppl 2):S279–83. [PMC free article] [PubMed] [Google Scholar]
- 7.Shaygannejad V, Tolou-Ghamari Z. What is the real fate of vitamin D in multiple sclerosis? Int J Prev Med. 2013;4(Suppl 2):S159–64. [PMC free article] [PubMed] [Google Scholar]
- 8.Shaygannejad V, Ardestani PE, Ghasemi M, Meamar R. Restless legs syndrome in Iranian multiple sclerosis patients: A case-control study. Int J Prev Med. 2013;4(Suppl 2):S189–93. [PMC free article] [PubMed] [Google Scholar]
- 9.Ashtari F, Shaygannejad V, Farajzadegan Z, Amin A. Does early-onset multiple sclerosis differ from adult-onset form in Iranian people. J Res Med Sci. 2010;15:94–9. [PMC free article] [PubMed] [Google Scholar]
- 10.Ghafari S, Ahmadi F, Nabavi SM, Memarian R, Kazemnejad A. Effect of applying progressive muscle relaxation technique on fatigue in multiple sclerosis patients. Shahrekord Univ Med Sci J. 2008;10:61–8. [Google Scholar]
- 11.Mohamadirizi S, Fahami F, Bahadoran P. Comparison of the effect of multimedia and illustrated booklet educational methods on women's knowledge of prenatal care. Iran J Nurs Midwifery Res. 2014;19:127–31. [PMC free article] [PubMed] [Google Scholar]
- 12.Mohamadirizi S, Bahadoran P, Fahami F. Comparsion between the impacts of e-learning and booklet education on primigravida women's satisfaction about postpartum care. IJOGI. 2013;16:1–8. [Google Scholar]
- 13.Gould D, Papadopoulos I, Kelly D. Tutors’ opinions of suitability of online learning programmes in continuing professional development for midwives. Nurse Educ Today. 2014;34:613–8. doi: 10.1016/j.nedt.2013.06.006. [DOI] [PubMed] [Google Scholar]
- 14.Gordon M, Chandratilake M, Baker P. Low fidelity, high quality: A model for e-learning. Clin Teach. 2013;10:258–63. doi: 10.1111/tct.12008. [DOI] [PubMed] [Google Scholar]
- 15.Toghyani R, Ramezani MA, Izadi M, Shahidi SH, Aghdak P, Motie Z, et al. The effect of prenatal care group education on pregnant mothers’ knowledge, attitude and practice. Iran J Med Educ. 2008;7:317–24. [Google Scholar]
- 16.Fahami f, Mohamadirizi s, Bahadoran p. Effect of Electronic Education on the Awareness of Women about post Partum Breast Feeding. International Journal of Pediatrics. 2014;2(3):57–63. [Google Scholar]
- 17.Bateman J, Allen M, Samani D, Kidd J, Davies D. Virtual patient design: Exploring what works and why. A grounded theory study. Med Educ. 2013;47:595–606. doi: 10.1111/medu.12151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Mohamadirizi S, Bahadoran P, Fahami F. Effect of E-learning on primigravida women's satisfaction and awareness concerning prenatal care. J Edu Health Promot. 2014;3:13. doi: 10.4103/2277-9531.127574. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Duque G, Demontiero O, Whereat S, Gunawardene P, Leung O, Webster P, et al. Evaluation of a blended learning model in geriatric medicine: A successful learning experience for medical students. Australas J Ageing. 2013;32:103–9. doi: 10.1111/j.1741-6612.2012.00620.x. [DOI] [PubMed] [Google Scholar]
- 20.Arastoo AA, Ahmadi A, Zahednejad SH. The comparision of effect of 8 weeks aerobic and yoga training on physiological cost index in multiple sclerosis patients. Sci Med J. 2011;10:153–62. [Google Scholar]
- 21.Neafsey PJ, Strickler Z, Shellman J, Chartier V. An interactive technology approach to educate older adults about drug interactions arising from over-the-counter self-medication practices. Public Health Nurs. 2002;19:255–62. doi: 10.1046/j.1525-1446.2002.19405.x. [DOI] [PubMed] [Google Scholar]
- 22.Southard BH, Southard DR, Nuckolls J. Clinical trial of an Internet-based case management system for secondary prevention of heart disease. J Cardiopulm Rehabil. 2003;23:341–8. doi: 10.1097/00008483-200309000-00003. [DOI] [PubMed] [Google Scholar]
- 23.Street RL, Jr, Voigt B, Geyer C, Jr, Manning T, Swanson GP. Increasing patient involvement in choosing treatment for early breast cancer. Cancer. 1995;76:2275–85. doi: 10.1002/1097-0142(19951201)76:11<2275::aid-cncr2820761115>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 24.Murray E, Davis H, Tai SS, Coulter A, Gray A, Haines A. Randomised controlled trial of an interactive multimedia decision aid on benign prostatic hypertrophy in primary care. BMJ. 2001;323:493–6. doi: 10.1136/bmj.323.7311.493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Mohamadirizi S, Shaygannejad V, Mohamadirizi Sh, Khosrawi S. The effect of electronic package on satisfaction in multiple sclerosis patients. Adv Biomed Res. 2017;6:89. doi: 10.4103/2277-9175.183143. doi:10.4103/2277-9175.183143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Vahabi YS, Tadrisi SD, Ghayem SH, Ebadi A, Daneshmandi M, Nia MS. Comparing the effect of triage education in lecture and multimedia software on nurses learning. Iran J Crit Care Nurs. 2011;4:7–12. [Google Scholar]
- 27.Shaygannejad V, Golabchi K, Dehghani A, Ashtari F, Haghighi S, Mirzendehdel M, et al. Color blindness among multiple sclerosis patients in Isfahan. J Res Med Sci. 2012;17:254–7. [PMC free article] [PubMed] [Google Scholar]
- 28.Gustafson DH, DuBenske LL, Namkoong K, Hawkins R, Chih MY, Atwood AK, et al. An eHealth system supporting palliative care for patients with non-small cell lung cancer: A randomized trial. Cancer. 2013;119:1744–51. doi: 10.1002/cncr.27939. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Gustafson DH, Hawkins R, McTavish F, Pingree S, Chen WC, Volrathongchai K, et al. Internet-Based Interactive Support for Cancer Patients: Are Integrated Systems Better? J Commun. 2008;58:238–57. doi: 10.1111/j.1460-2466.2008.00383.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Langkamp DL, Hoshaw-Woodard S, Boye ME, Lemeshow S. Delays in receipt of immunizations in low-birth-weight children: A nationally representative sample. Arch Pediatr Adolesc Med. 2001;155:167–72. doi: 10.1001/archpedi.155.2.167. [DOI] [PubMed] [Google Scholar]
- 31.Saeedinejat S, Vafaeenajar A. The effect of e-learning on students’ educational success. Iran J Med Educ. 2011;11:1–11. [Google Scholar]
- 32.Mayer RE. Multimedia learning. 2nd ed. London: Cambridge University Press; 2009. [Google Scholar]
- 33.Mohamadirizi S, Bahadoran P, Fahami F. Effect of E-learning on primigravida. J Educ Health Promot. 2014;3:70–4. doi: 10.4103/2277-9531.127574. [DOI] [PMC free article] [PubMed] [Google Scholar]